
Abstract
Keywords
Introduction
Recent advances in arthroscopic techniques in the past decade have led to widespread acceptance of arthroscopic rotator cuff repair as a surgical option for painful rotator cuff tears.1–3 Despite excellent clinical outcomes after arthroscopic repair, a high rate of postoperative recurrent rotator cuff tears is a major concern. 4 The integrity of the cuff repair after arthroscopic surgery using various methods has been extensively studied with the aim of establishing a repair technique that decreases the retear rate following rotator cuff repair, especially for large or massive tears, which have a high retear rate.5–7
Acromial bony erosion is a postoperative complication after arthroscopic rotator cuff repair. Impingement of the knots to the undersurface of the acromion has been suggested as a cause of acromial bony erosion.8,9 Arthroscopic findings at the second surgery revealed that knots on the tendon were impinging on the portion with acromial erosion during shoulder abduction. Acromial bony erosion is relatively rare,8,10 and the influence of knot impingement on clinical outcome has not been determined in the small case series published to date.
Symptomatic knot impingement has recently been reported in two patients with partial-thickness tears that had been repaired by a single-row technique. 9 We have also encountered cases of symptomatic knot impingement and acromial erosion, more often in patients with a partial-thickness tear and small-sized full-thickness tears than in those with large or massive tears. Therefore, we postulated that symptomatic knot impingement would occur more frequently in patients with partial-thickness or small tears. The purpose of this study was to determine the prevalence of acromial bony erosion in patients with partial-thickness or small tears on postoperative magnetic resonance imaging (MRI). The effect of acromial bony erosion on postoperative clinical outcomes and its risk factors was also examined.
Materials and methods
Patient selection
We retrospectively reviewed patients who underwent arthroscopic repair of partial-thickness or small full-thickness rotator cuff tears from April 2016 to October 2019. This study was approved by the institutional review board of our institution, and the need for informed consent was waived. Ninety-seven patients with partial-thickness or small full-thickness rotator cuff tears underwent arthroscopic rotator cuff repair by the first author during the study period.
The inclusion criteria were as follows: (1) pain and disability that failed to respond to conservative treatment such as nonsteroidal anti-inflammatory drugs, steroid injection, and physical therapy for at least 3 months; (2) a partial or small tear (less than 10 mm in the anteroposterior direction) isolated on the supraspinatus tendon detected intraoperatively; and (3) follow-up with serial clinical and MRI evaluations for at least one year. Exclusion criteria were as follows: (1) history of surgery on the same shoulder; (2) concomitant labral tears with shoulder instability; (3) concomitant glenohumeral arthritis; and (4) isolated subscapularis tear or arthroscopic debridement without repair.
Surgical technique
All procedures were performed with the patient in the beach-chair position under general anesthesia with the upper extremity fixed by a limb positioner. Diagnostic arthroscopy was performed to evaluate the rotator cuff and associated pathology. Pathologic intra-articular lesions were treated appropriately. The arthroscope was placed into the subacromial space and a complete bursectomy was performed, followed by subacromial decompression in all patients. Acromioplasty was limited to the removal of large acromial spurs. Minimal decortication of the acromial undersurface and minimal release of the coracoacromial ligament were performed if the undersurface of the acromion was free of osteophytes.
For the articular-sided partial-thickness tear, the exposed medial footprint on the greater tuberosity was cleared of soft tissue, and the degenerative edge of the torn supraspinatus tendon was debrided. The thickness of the tear was then carefully evaluated using a calibrated probe and in situ transtendon repair was performed for tears involving more than 50% of the tendon thickness. When the partial-thickness tear was near full-thickness, involving >75% of the tendon thickness, the remaining bursal cuff tissue was debrided with conversion to a full-thickness tear. Five of the 10 articular-sided partial-thickness tears were repaired using a transtendon technique and the other five tears were repaired after converting to full-thickness tears. A single double-loaded suture anchor was used. Single and transosseous-equivalent double-row repairs were performed depending on the timing of the surgery.
In the case of a tear on the bursal side, the remaining medial cuff tissue was preserved as much as possible. The residual fibers were taken down if the remaining cuff tissue was of poor quality and beyond 75% of the footprint. Five of the 21 patients with bursal-sided partial-thickness tears showed conversion to full-thickness tears during surgery. One or two double-loaded suture anchors were used according to the morphology and size of the tear. The tears were repaired using the single-row technique in seven patients, the transosseous-equivalent double-row technique in 11 patients, and a side-to-side repair without a suture anchor in three patients.
When a small full-thickness tear was identified arthroscopically, a single-row, conventional double-row, or transosseous-equivalent double-row repair was performed according to the tear pattern and preference of the surgeon.
Postoperative management
The same postoperative protocol was applied for both partial-thickness and small full-thickness tears. The shoulder was immobilized with an abduction brace for 3 weeks. Passive gentle range of motion exercises were started immediately after the surgery. Active-assisted exercises were allowed at 8 weeks postoperatively, and strengthening exercises were initiated 3 months after the operation. Patients were allowed to return to their full sports activities gradually after 5–6 months.
Clinical evaluation
All patients were evaluated preoperatively and postoperatively at least 12 months after surgery using the American Shoulder and Elbow Surgeons (ASES) score, University of California at Los Angeles (UCLA) Shoulder Rating Scale, and Simple Shoulder Test (SST). A visual analog scale (VAS) pain score was recorded at the same time.
Magnetic resonance imaging evaluation
Routine MRI scans were obtained at 3 weeks, 6 months, and 12 months after surgery. All MRI scans were performed using a 1.5-T unit (Signa HDi 1.5 T; GE Healthcare Japan, Tokyo, Japan). The affected arm was placed at the side of the body in a neutral rotation position. The examination was performed using spin-echo T1-weighted sequences (repetition time, 450–600 ms; echo time, 10–15 ms) and T2-weighted sequences (repetition time, 3600–4000 ms; echo time, 80–90 ms) in axial, oblique coronal, and oblique sagittal planes. All images were obtained on a 256 × 192 matrix. The field of view was 18 cm, and the slice thickness was 4 mm, with an interslice gap of 1 mm.
Oblique coronal T2-weighted and oblique sagittal T2-weighted images were evaluated to determine the loss of normal contour on the inferior surface of the acromion and the presence of hyperintense lesions. Such lesions were defined as acromial erosions. Magnetic resonance imaging scans taken at 6 and 12 months after surgery were compared with those acquired in the early postoperative period to exclude an influence of excessive acromioplasty (Figure 1). When acromial erosion was suspected, three-dimensional computed tomography was performed for confirmation (Figure 2).
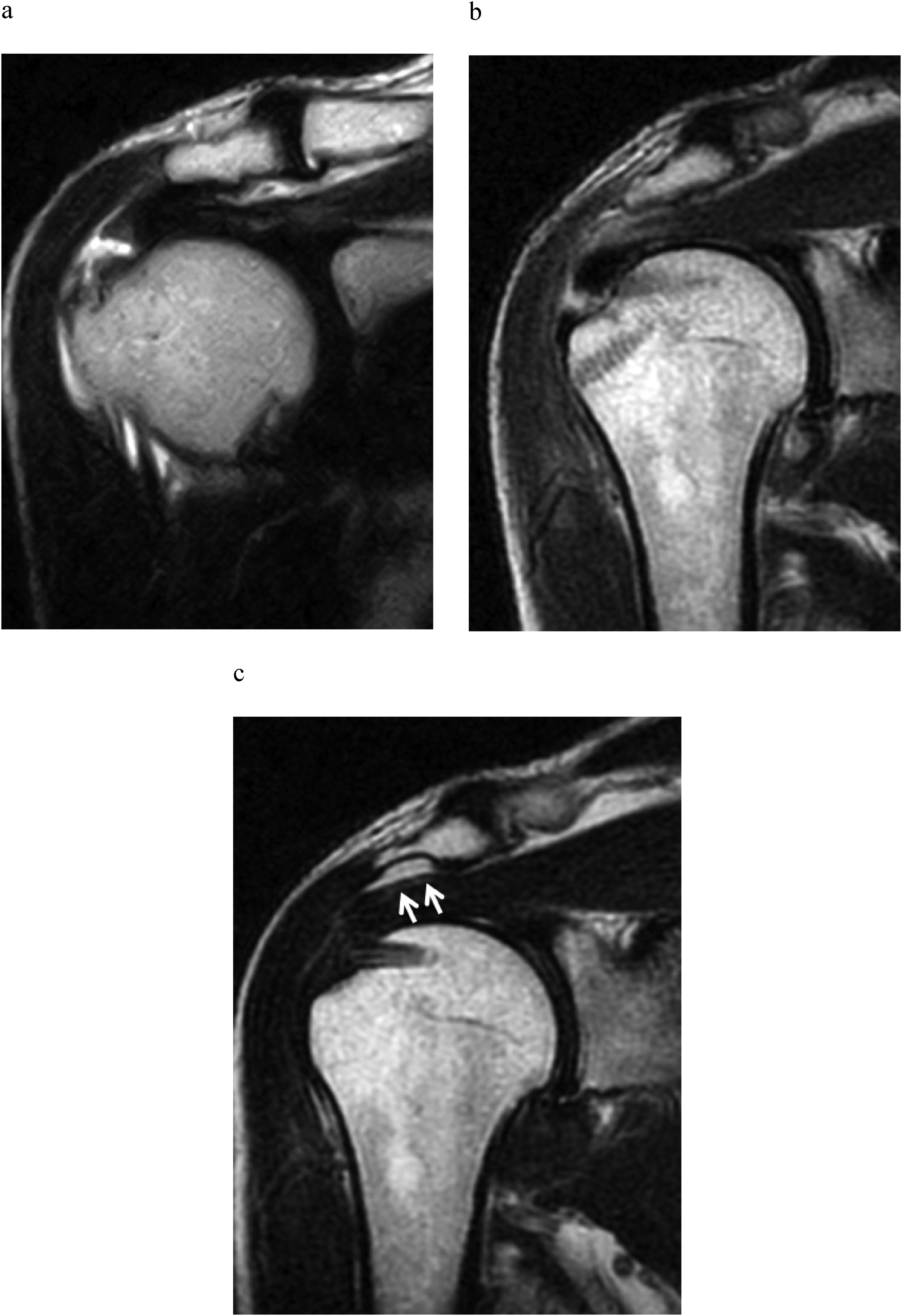
Acromial bony erosion detected on postoperative magnetic resonance images. (a) Preoperative oblique coronal T2-weighted image. (b) Early postoperative T2-weighted image. (c) T2-weighted image at 6 months postoperatively. When compared with the early postoperative magnetic resonance image, acromial erosion with subacromial effusion was detected (white arrows).
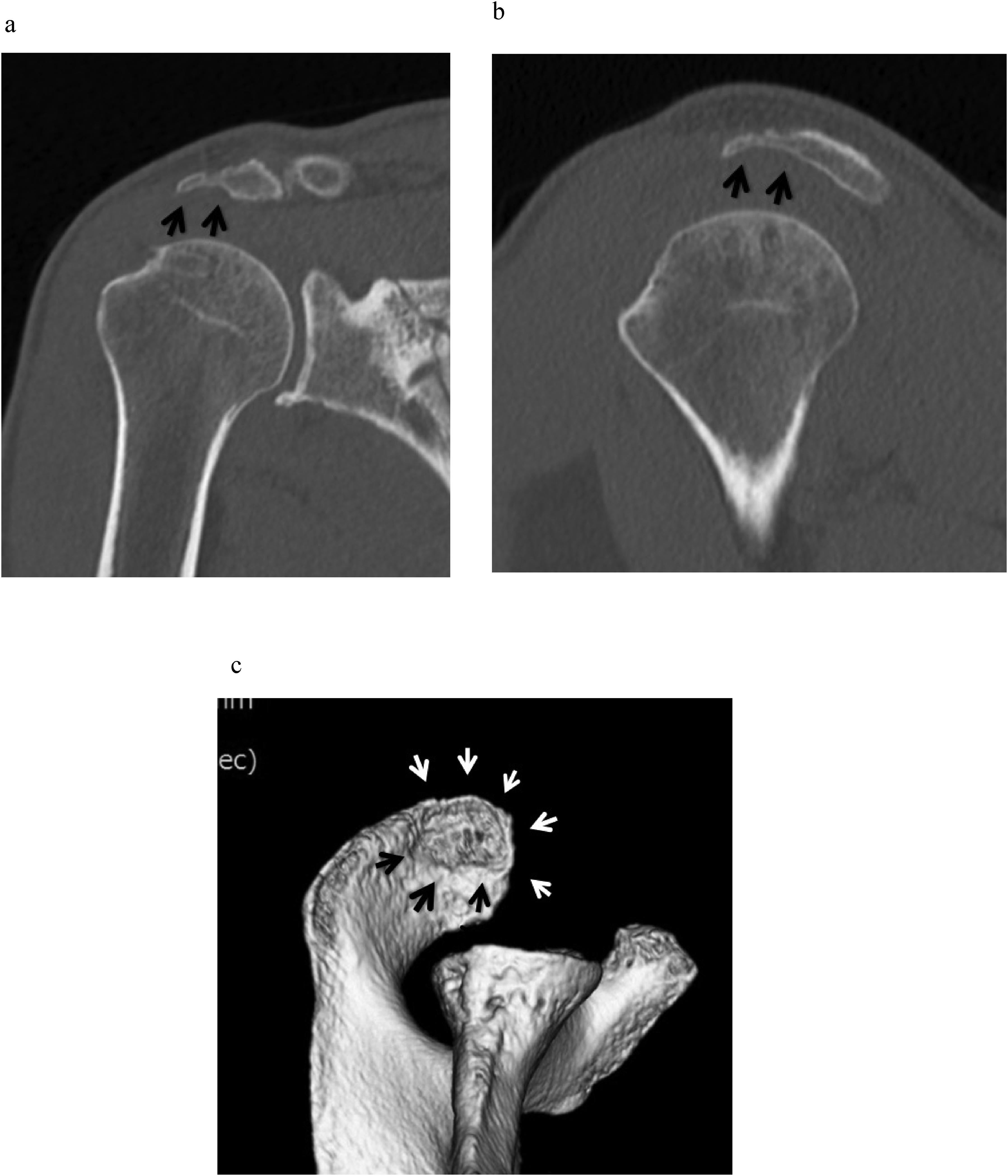
Multiplanar reconstruction and three-dimensional computed tomography scans. (a) Oblique coronal reconstruction image showing thinning of the lateral half of the acromion (black arrows). (b) Oblique sagittal reconstruction image showing thinning of the anterior half of the acromion (black arrows). (c) Three-dimensional image clearly showing acromial erosion on the undersurface of the acromion (black and white arrows).
The integrity of the cuff was evaluated postoperatively by MRI using the classification described by Sugaya et al., 4 and types 4 and 5 were diagnosed as postoperative recurrent tear. All images were reviewed by a single orthopedic surgeon (SF).
Statistical analysis
Statistical analysis was performed to compare patient groups according to whether or not acromial erosions were present. An unpaired t-test or the Mann–Whitney U test was used to compare age, VAS pain score, STT, active forward flexion, ASES score, UCLA score, and the number of suture anchors used between the two groups depending on whether the data were parametric or nonparametric, respectively. The chi-squared test or Fisher's exact test was used to compare sex, affected side (dominant or nondominant), cuff-tear pattern (articular-sided partial-thickness, bursal-sided partial-thickness, small full-thickness), and repair method (side-to-side, single-row, double-row, suture-bridge technique). All statistical analyses were performed using SPSS Statistics software (version 25.0; IBM Corp., Armonk, NY). A p-value of <0.05 was considered statistically significant.
Results
Seventy-four patients satisfied the inclusion criteria, 31 of whom had partial-thickness tears (10 articular-sided, 21 bursal-sided) and 43 had small full-thickness tears. Mean age at surgery was 62.5 ± 10.3 (range, 21–80) years. There were 44 men and 30 women. Forty-three patients had involvement of the dominant shoulder and the mean follow-up duration was 18.1 (range, 12–48) months.
Overall, erosion on the undersurface of the acromion was observed in 17 (23.0%) of the 74 patients. All erosions were observed at 6 months and did not progress until 12 months. Mean age at surgery for acromial erosions was 56.9 (range, 21–68 years), which was significantly younger than that of patients without acromial erosion (Table 1). There was no significant difference in sex or dominant involvement between the two groups. The incidence of acromial erosion was 10.0% for articular-sided partial-thickness tears, 42.9% for bursal-sided partial-thickness tears, and 16.3% for small full-thickness tears. Acromial erosion was observed more frequently with bursal-sided partial-thickness tears. The arthroscopic repair technique used did not affect the occurrence of acromial erosion.
Demographic and surgical data of the patients.
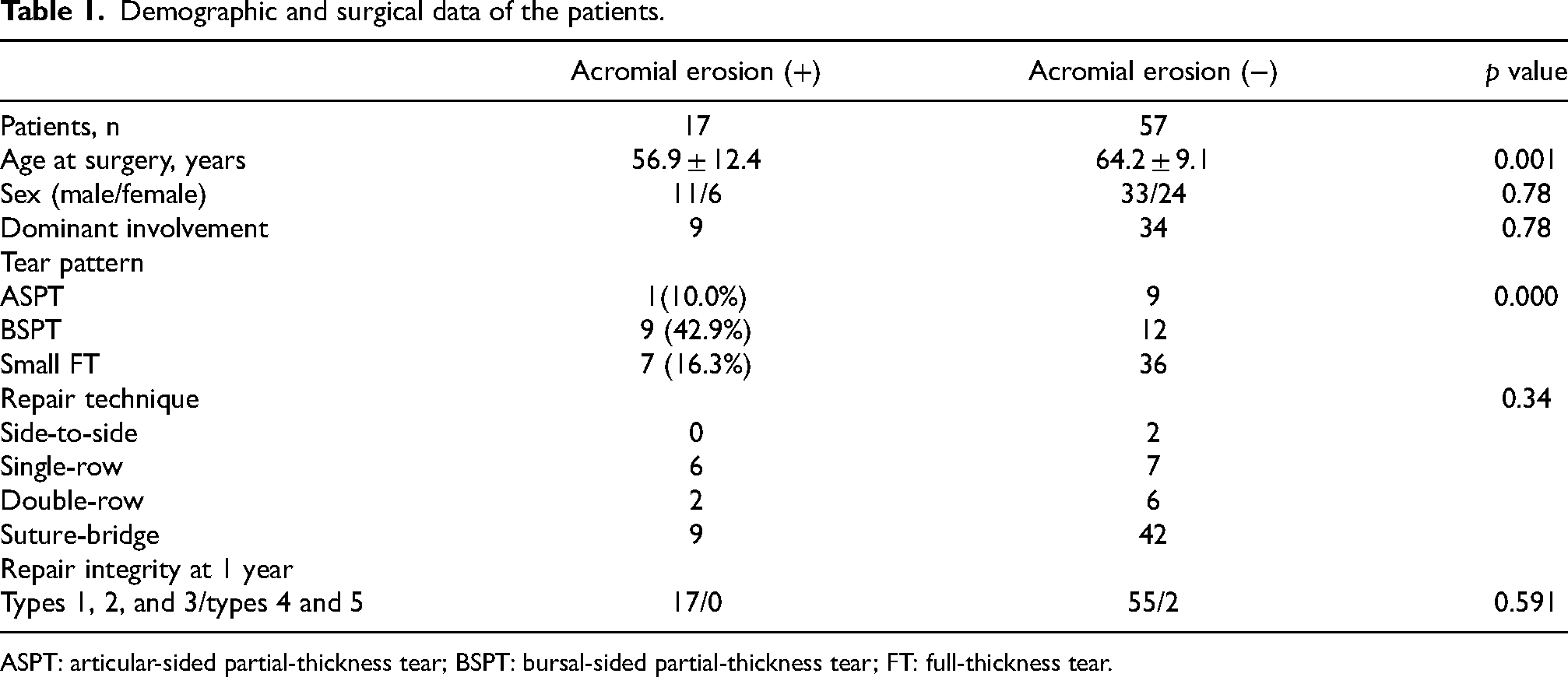
ASPT: articular-sided partial-thickness tear; BSPT: bursal-sided partial-thickness tear; FT: full-thickness tear.
Overall, most patients achieved significant improvements in their functional scores at the latest follow-up (Table 2). Mean VAS pain score improved from 7.1 ± 2.0 preoperatively to 1.3 ± 1.5 postoperatively, mean SST score from 7.4 ± 2.6 to 11.0 ± 1.2, mean UCLA score from 17.1 ± 5.9 to 32.3 ± 4.2, and mean ASES score from 44.8 ± 21.0 to 89.8 ± 12.8. There was no significant difference in clinical outcome scores between the two groups. The repair surgery was successful in all patients who developed acromial erosions. Overall, the retear rate was 2.7% in this series.
Preoperative and postoperative clinical scores according to acromial erosion status.
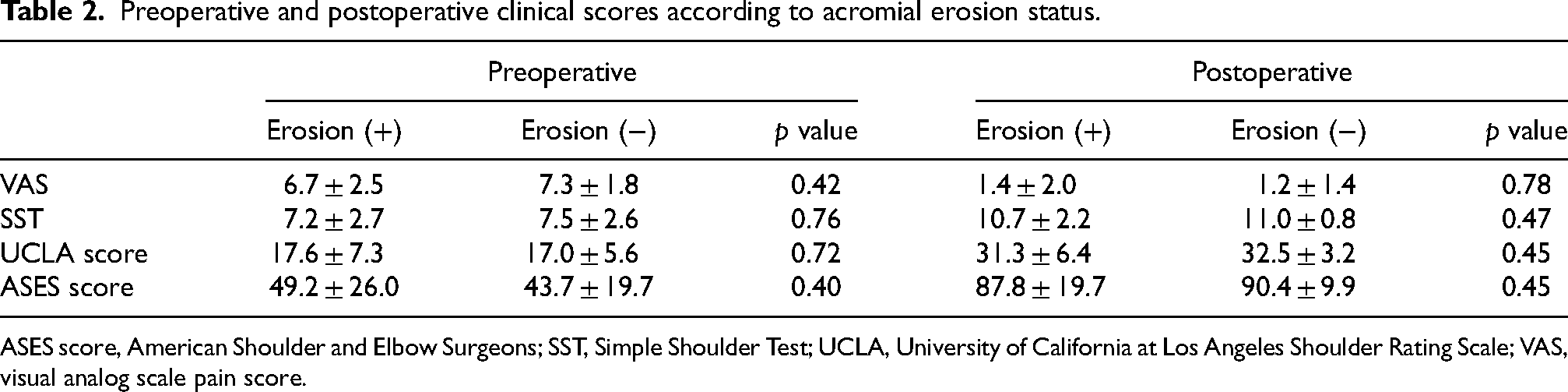
ASES score, American Shoulder and Elbow Surgeons; SST, Simple Shoulder Test; UCLA, University of California at Los Angeles Shoulder Rating Scale; VAS, visual analog scale pain score.
Two cases required knot removal due to symptom impingement. Both were partial-thickness tears; one was articular-sided and the other was bursal-sided.
Bony erosion was observed arthroscopically on the undersurface of the acromion facing the suture knots on the repaired tendon (Figure 3). After removal of the sutures, the pain and impingement sign were relieved in both patients.
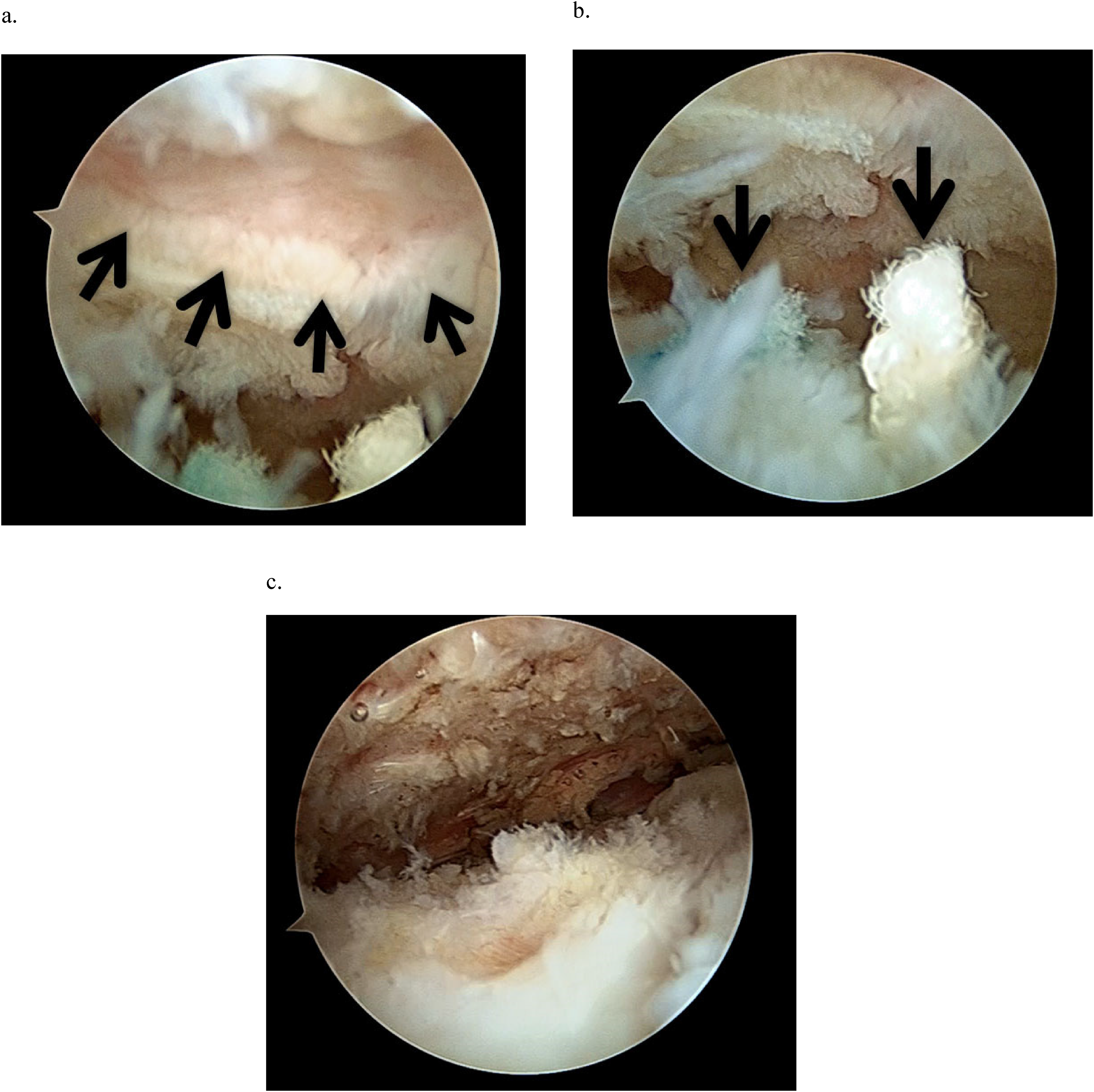
Arthroscopic views of the right shoulder from the standard posterior portal showing (a) crater formation on the undersurface of the acromion (black arrows), (b) prominent suture knots on the repaired supraspinatus tendon (black arrows), and (c) healing of the repaired tendon after knot removal.
Discussion
Subacromial osteolysis after arthroscopic rotator cuff repair was first reported by Hotta and Yamashita 8 in 2010. They suggested impingement of the suture knots in the subacromial space as the cause and described these pathologies as knot impingement. In their series of nine patients with knot impingement, mild pain on movement or dullness was common, and range of motion at the shoulder and muscle strength were almost normal. Osteolysis of the undersurface of the acromion was usually identified within 3 months after the repair and increased in size over time. Second-look arthroscopy confirmed that knots on the greater tuberosity corresponded to the osteolytic area on the inferior surface of the acromion and removal of the sutures relieved symptoms. In a later study by Park et al., 10 the incidence of acromial erosion was compared according to whether patients had undergone single-row repair or suture-bridge repair. Acromial erosion was observed in 2 (1.7%) of 118 patients with single-row repair and in 1 (1%) of 103 patients with suture-bridge repair; the difference was not statistically significant. No additional surgery was performed to remove the knots in their cases, and thus the pathology of the knot impingement was not determined.
Although knot impingement is a complication after arthroscopic rotator cuff repair, it has not been well recognized because of its mild symptoms and relatively rare incidence. Furthermore, factors related to its occurrence have not been examined in detail because of the small number of cases reported. Recently, Uchida et al. 11 reported two cases of subacromial bone erosion after arthroscopic single-row repair for a bursal-sided partial-thickness tear of the supraspinatus tendon. Arthroscopic dynamic assessment confirmed that the suture knots were engaged with the eroded bone during 60–120 degrees of shoulder elevation, external or internal rotation of the abducted shoulder, and horizontal abduction at 90 degrees of shoulder abduction. They did not find any symptomatic knot impingement in patients with medium, large, or massive tears and concluded that the number of knots might not be a risk factor for knot impingement. However, the prevalence of subacromial erosion was not determined in their study.
Since Hotta and Yamashita 8 published the first report on knot impingement, we have focused on acromial bony erosion after rotator cuff repair. Our impression had been that acromial erosion was more common in patients with partial-thickness tears than in previous reports. Therefore, we performed this retrospective study to investigate the incidence of acromial erosion in partial-thickness tears. Small full-thickness tears were also included because some partial-thickness tears were repaired after converting to full-thickness tears. In our series, erosion on the undersurface of the acromion was observed in 23.0% of the patients with partial-thickness or small full-thickness rotator cuff tears. The prevalence was higher in patients with bursal-sided partial-thickness tears than with other types of tear. Ichida et al. 9 similarly found symptomatic knot impingement only in patients with small partial-thickness rotator cuff tears. They suggested that a thicker tendon could be more likely to cause knot impingement in patients with partial-thickness tears than of those with complete medium-to-massive tears by decreasing the distance between the knot and the undersurface of the acromion. However, their suggestion does not explain the lower incidence of knot impingement in patients with articular-sided partial-thickness tears.
In this case series, the average age of patients with acromial erosion was 56.9 years, which was significantly younger than that in those without acromial erosion. The average age of the nine cases reported by Hotta and Yamashita was 54.1 years, which was similar to the age of our patients. They suggested that young athletes were at higher risk of knot impingement; however, there were no athletes in our series. The arthroscopic findings in the two patients in our study who underwent repeat surgery were similar to those reported by Uchida et al., supporting the notion that acromial bone erosion resulted from impingement of the suture knots. Only about 10% of the cases with acromial erosion in the present study underwent repeat surgery, and thus it is not clear whether these arthroscopic findings are pathologically representative of all cases. The reoperation rate was low because the clinical outcomes were not adversely affected by knot impingement and were mostly asymptomatic. Even when present, symptoms were often mild and most patients did not want to undergo repeat surgery for suture removal. A knotless repair is recommended for partial-thickness tears to prevent knot impingement. Repair with suture tape is another option.
This study has several limitations. Firstly, it was a retrospective study and the study population did not include patients with medium or large tears. While we did not directly compare the prevalence of acromial erosion in partial-thickness and small full-thickness tears was not directly compared to that of larger tears, we clearly demonstrated a significantly higher incidence when compared to the results reported in previous studies. Secondly, image evaluation was performed by a single rater. Although most cases of acromial erosion were visibly apparent and confirmed by computed tomography, subtle morphological changes might be overlooked and intrarater and inter-rater reliability was not established. Finally, the reason for the higher prevalence of acromial erosion in partial-thickness and small full-thickness tear remained unclear. In this study, acromial erosion was more prevalent in bursal-sided tears. Bursal-sided tears often result from subacromial impingement during abduction of the arm, and imbalance of the rotator cuff muscles may persist postoperatively, potentially leading to acromial erosion. However, further study is required for a better understanding of the pathomechanism of acromial erosion.
Although the mechanism of knot impingement is still unclear, the incidence of partial-thickness and small full-thickness tears may be higher than previously reported. Surgeons should be aware of these pathologies after arthroscopic rotator cuff repair, especially when the patient complains of a residual impingement sign. Arthroscopic removal of the knots might be effective for symptomatic knot impingement.
Conclusion
In this study, the prevalence of acromial erosion after arthroscopic repair of partial-thickness and small full-thickness rotator cuff tears was 23.0% and was highest for bursal-sided partial-thickness tears. Two of the 74 patients required revision surgery due to postoperative impingement. Arthroscopic removal of the knots relieved the pain and impingement in these cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.