
Abstract
Introduction
Hallux valgus is a common foot deformity that causes forefoot widening, difficulty fitting shoes, bunion pain, and transfer metatarsalgia. Studies have shown that correcting the 1,2 intermetatarsal angle (IMA) can significantly reduce forefoot width and improve symptoms. This study aims to review the radiological and functional outcomes of hallux valgus reconstruction with IMA closure using mini-tightrope suture buttons.
Methods
A case series of 52 consecutive patients who underwent minimally invasive surgical reconstruction of hallux valgus deformity utilising the dynamic tightrope fixation was included. All patients had >1 year follow-up with interim assessments at baseline, 3 months, 6 months, and 1 year. Primary outcomes included IMA in weight-bearing feet X-rays, and secondary outcomes included the hallux valgus angle (HVA) and clinical function via the Foot and Ankle Outcome Score.
Results
Based on radiological analysis, the 1,2 IMA and the HVA significantly improved. Clinical function also showed significant improvement in symptoms, pain, activities of daily living, and quality of life subsection. No major intra-operative complications occurred in this series; however, ∼5% of the patients required revision surgery due to a recurrence of the hallux valgus or overcorrection into hallux varus.
Conclusion
Dynamic tightrope fixation is a simple surgical technique that effectively corrects the 1,2 IMA during hallux valgus surgery.
Introduction
Hallux valgus, a common forefoot deformity,1–4 affects nearly one-third of the population. It can cause a range of symptoms, from bunion pain and metatarsalgia to complications from footwear impingement.1–3 Surgical intervention is the only evidence-based option for correcting this deformity, and various techniques are available. Minimally invasive surgery is becoming more popular due to its improved cosmetic outcomes and lower risk of wound complications. Surgeons often perform multiple procedures based on their preferences and equipment.4,5 One important part of the surgery is closing the 1,2 intermetatarsal angle (IMA), 6 which can be achieved through osteotomies, arthrodesis of the tarsal–metatarsal joint, 7 or dynamic fixation after soft tissue procedures.8–11 While much of the published literature describes open surgery, there have been previous reports that have shown positive long-term results with sutures passed through the metatarsals through a minimally invasive surgical approach, although this procedure has a steep learning curve. 6 Orthopaedic procedures commonly use endobuttons for fixation,12,13 and they have been proven effective for ankle syndesmosis.14–16 However, there have been complications in forefoot surgeries, such as iatrogenic fractures, due to large sutures intended for the ankle.17,18 To address this, smaller dynamic fixation devices with modified drilling directions have been designed to minimise complications. This study will use the mini-tight rope technique to present a case series of patients who underwent 1,2 IMA closure with percutaneous dynamic fixation. To the best of our knowledge, this will be the largest series utilising this method for Hallux valgus surgery. 19
Methodology
This retrospective single-centre case series was conducted at the Prince of Wales Hospital, Hong Kong. It will be performed following the STROBE checklist for observational studies. Data were retrieved via the Clinical Data Analysis and Reporting System database.
Eligibility criteria included consecutive patients receiving hallux valgus surgery utilising the dynamic mini-tightrope (Arthrex, USA) recruited from January 2019 to July 2022. Definition of hallux valgus was HVA ≥ 20° and IMA ≥ 9°. Exclusion criteria included those who underwent concomitant procedures that may affect rehabilitation, such as concomitant lesser toe surgery, 2 revision cases for previous Hallux valgus surgery, and those with active physical or psychological comorbidities affecting the post-operative rehabilitation.
All patients underwent a standardised surgical procedure with an arthroscopic assisted lateral soft tissue release 20 utilising a 1.9 mm arthroscope, 8 an arthroscopic-assisted bunionectomy and a percutaneous medial capsular plication.5,6 The intervention explored in this study is the technique of 1,2 IMA closure, which is performed in conjunction with the aforementioned procedures. The 1,2 intermetatarsal space was then closed with two 1.1 mm mini-tightropes through one proximal and one distal percutaneous incision (Figure 1). A 5 mm skin incision is created between the second and third metatarsal under fluoroscopic guidance at the anticipated level; the skin is incised and then bluntly dissected down to the lateral aspect of the second metatarsal. A 1.1 mm interosseous tunnel is drilled through the second metatarsal and the first metatarsal, with the aim of drilling the longest diameter possible. A looped guide wire was passed through the interosseous tunnel, and a percutaneous incision was created at the medial first metatarsal and bluntly dissected down the bone; a looped suture was then brought from medial to lateral, shuttling the mini-tightrope implant through until the button sat flush with the medial first metatarsal cortex. The procedure is repeated proximally; then the 1,2 IMA is closed, and the lateral end buttons are tightened. The additional step of shuttling the implant from the medial towards the lateral is performed so that the endobutton suture knots sit in the second to third metatarsal webspace and cause minimal impingement in contrast to having the surgical knot at the medial foot (Figure 2).

Post-operative and pre-operative radiograph after dynamic fixation of the 1,2 intermetatarsal angle (1,2 IMA).

Intraoperative fluoroscopic images of application of dynamic fixation endobuttons.
All patients followed the same rehabilitation protocol 3 : non-weight bearing for 2 weeks, followed by 10 weeks of heel walking before they could resume normal shoes.
Outcomes were assessed at baseline, 3 months, 6 months, and 12 months post-surgery. The primary outcome measure was the 1,2 IMA on weight-bearing X-rays. Secondary outcome measures included the hallux valgus angle (HVA), tibia sesamoid position, 7 and the functional outcome via a standardised patient-reported outcomes score,21–23 the Foot and Ankle Outcome Score (FAOS). 24
Statistical analysis was performed on SPSS (IBM) and paired t-tests with significance determined by a p-value of <0.05.
Results
Fifty-two patients who met the eligibility criteria were included in the analysis. The mean age at operation was 58.7 (19–75), and the female/male ratio was 6:1.
Radiological results are shown in Table 1. After one year, the angle of the IMA significantly improved from 14.5° (±2.87) to 9.42° (±2.56) with a p-value < 0.05 (Figure 3). The HVA also improved from 39.3° (±9.33) to 15.3° (±14.08) with a p-value <0.05 (Figure 4). Additionally, various aspects of the foot and ankle outcomes score – including symptoms, pain, activities of daily living, and quality of life – showed significant improvement from the baseline. In terms of complications, there were no significant issues during the surgery and no wound complications afterwards 25 (Table 2). Six patients experienced a radiological recurrence of hallux valgus, defined as an HVA >20°. Four of these six patients were asymptomatic, and one declined revision surgery. Moreover, two patients experienced hallux varus and both required revision surgery. Overall, 3 out of 52 patients (5.78%) required revision surgery due to alignment loss.
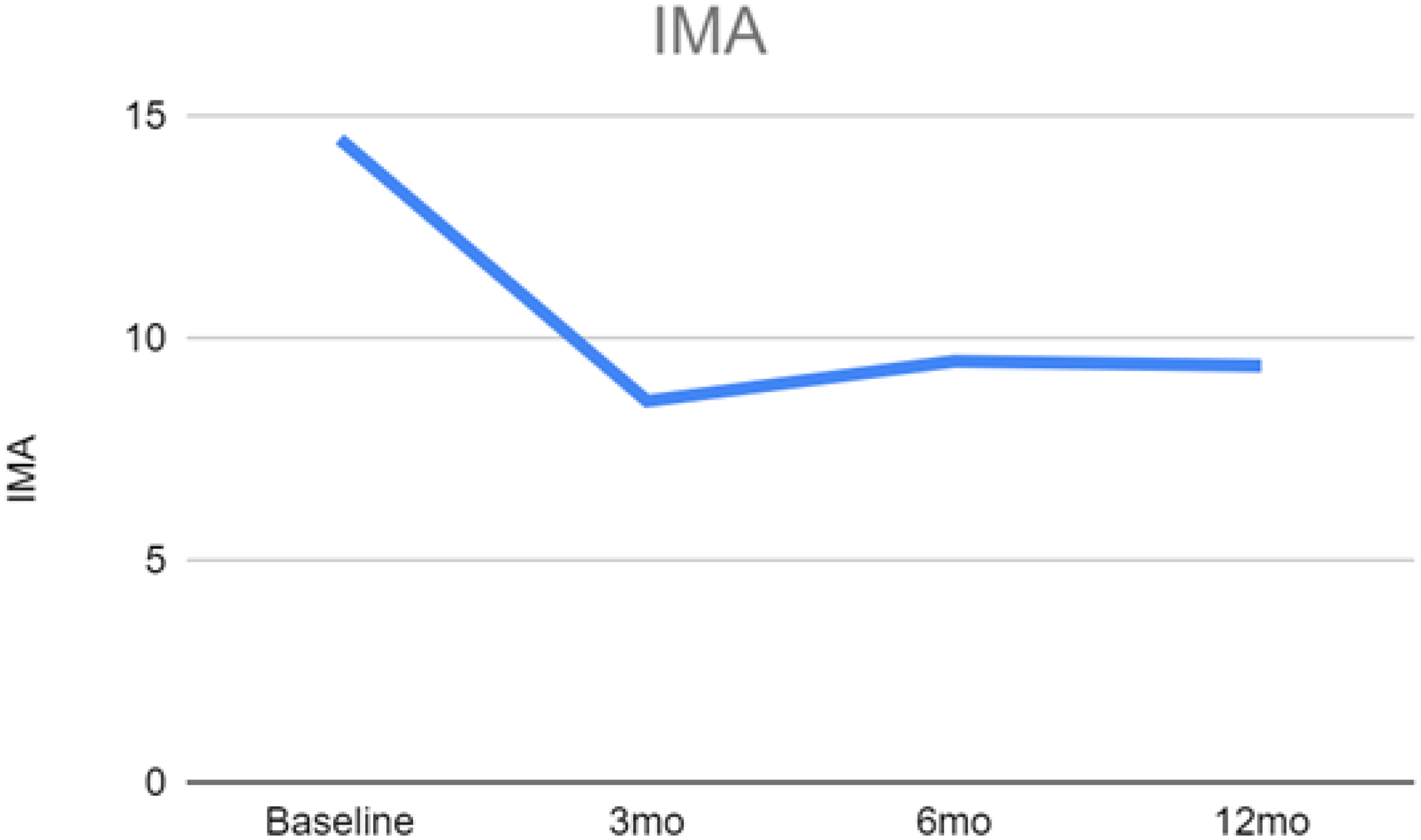
Changes in the 1,2 intermetatarsal angle (1,2 IMA).
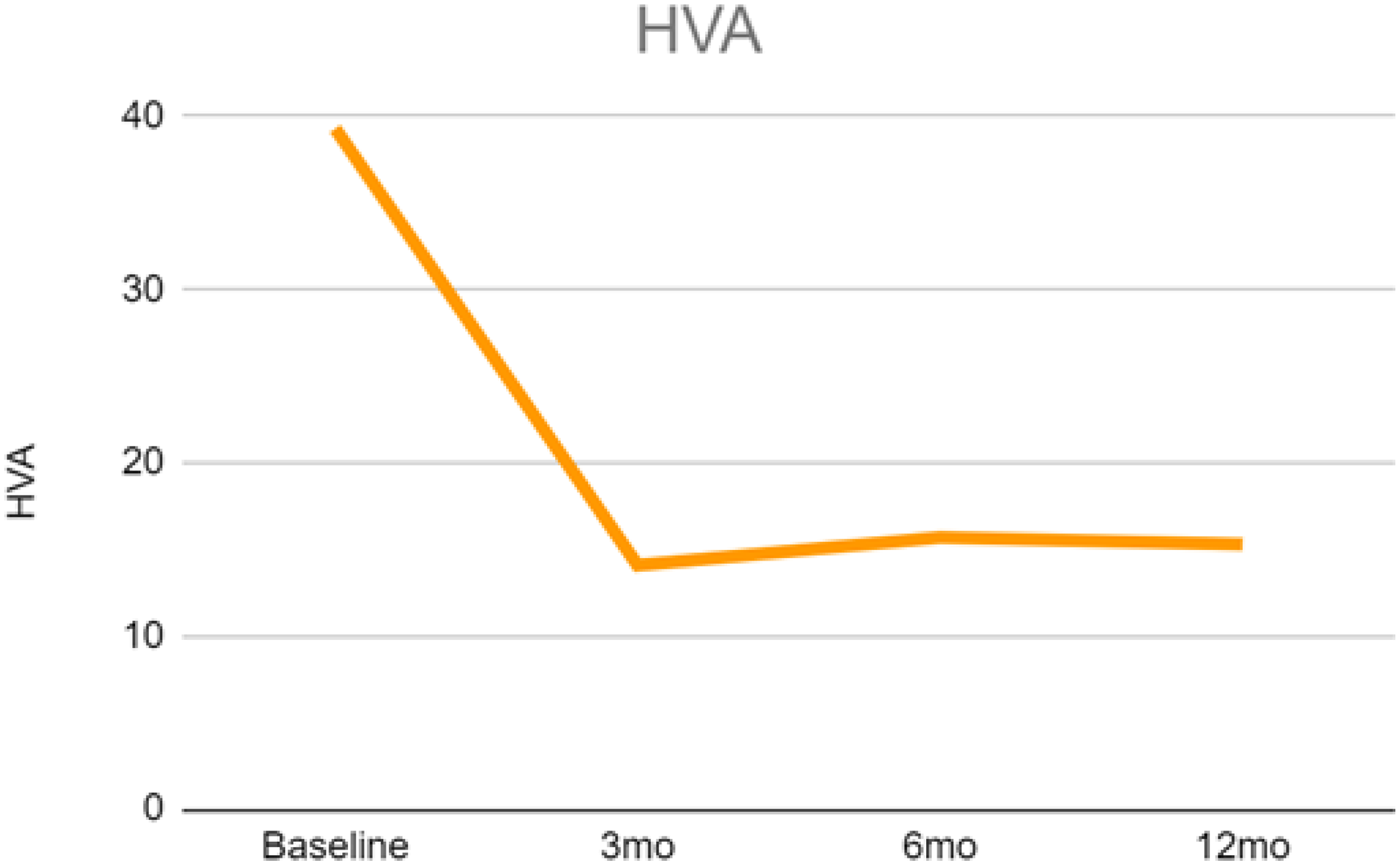
Changes in the hallux valgus angle (HVA).
Radiological changes on weight-bearing dorsal-plantar feet radiographs.
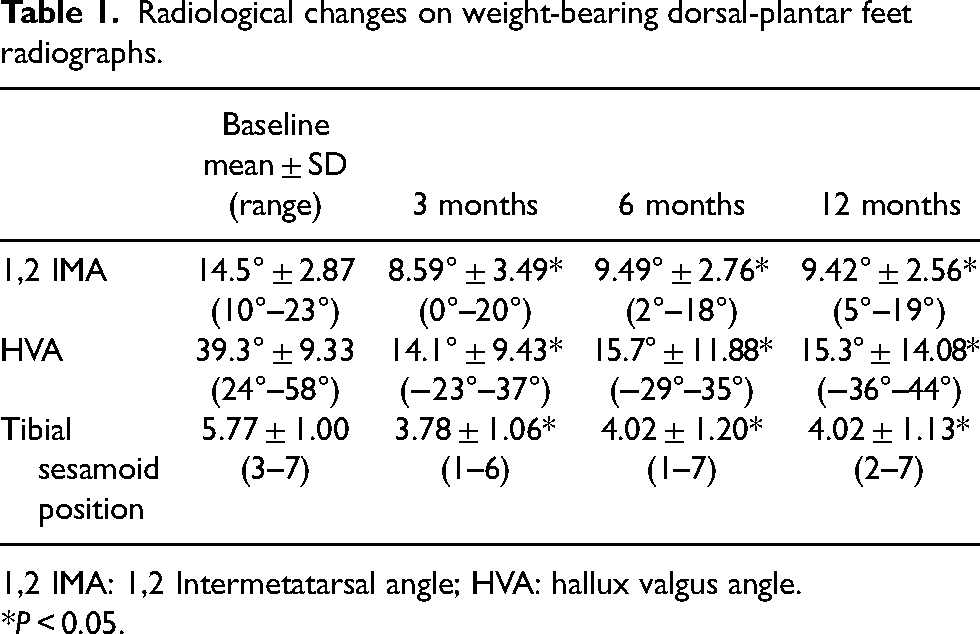
1,2 IMA: 1,2 Intermetatarsal angle; HVA: hallux valgus angle.
*P < 0.05.
(FAOS) at various time points.
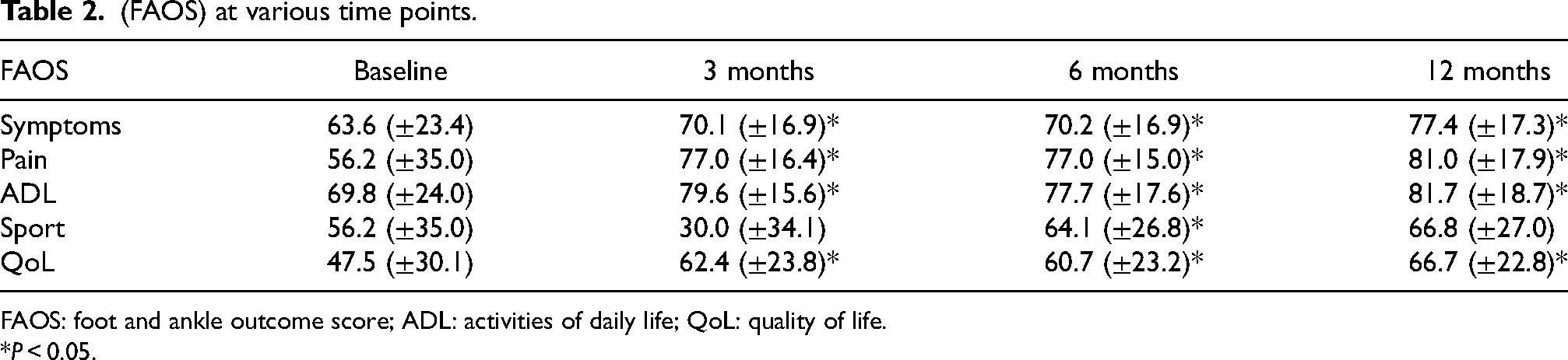
FAOS: foot and ankle outcome score; ADL: activities of daily life; QoL: quality of life.
*P < 0.05.
Discussion
Dynamic fixation of the 1,2 IMA with a tightrope device effectively improves clinical and radiological outcomes and can maintain a good alignment for 1-year post-surgery. Clinical symptoms and function improved significantly except for higher physical functions, including squatting, running, and jumping. This may be a selection bias as the Hallux valgus demographic in our series included many elderly females. Results are comparable to a long-term follow-up study 4 utilising a percutaneous proximal screw in addition to a percutaneous distal first and second metatarsal cerclage suture construct published by our group; however, the procedure of closing the IMA with a dynamic endobutton described in this paper is technically much simpler. 26 The limitations of this study include a relatively short follow-up period, and the authors believe a re-analysis of these patients after >10 years will be a fruitful exercise. In addition, this is a single-centre case series describing one of many available surgical procedures; future studies should prospectively compare different surgical options in a multi-centre randomised controlled clinical trial to help delineate which surgical technique is superior. Future studies should include subgroup analysis of different deformity severities as it is often suggested that bony procedures may be more effective than soft tissue procedures when treating more severe deformities.
Conclusion
This case series has shown that closure of the 1,2IMA can be effectively performed by utilising a mini-tightrope dynamic fixation with minimal complications. Both radiological correction and functional improvement were maintained at 1-year post-surgery.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.