
Abstract
The objective of this study was to assess the educational quality and reliability of YouTube videos related to lower extremity amputation (LEA) versus limb salvage. Pertinent YouTube videos were identified using specific search terms and video educational quality was assessed via validated assessment tools. Fifty-nine videos met inclusion criteria and the mean Journal of the American Medical Association (JAMA) score was 2.3 ± 0.65 (range: 0–4), indicating poor reliability. The mean Global Quality Score (GQS) was 2.66 ± 0.99 (range: 1–5), reflecting suboptimal educational quality. The mean Limb Salvage versus Amputation (LSA) score was 5.59 ± 3.66 (range: 0–15), indicating limited content quality specifically related to LEA versus limb salvage. Longer video duration was positively correlated with higher JAMA, GQS, and LSA scores. Hospital/University-sponsored videos had higher JAMA and GQS scores and videos by Healthcare Professionals (Nonphysician: PhDs and medical educators) content creators had the highest LSA scores. The study highlights the need for improved patient educational resources on LEA versus limb salvage, as the overall reliability and educational quality of YouTube videos on this topic is poor.
Keywords
Introduction
In the United States alone, approximately 185,000 lower extremity amputations (LEAs) are performed annually, with 54% indicated for systemic disease and 45% for trauma. 1 In developed countries, up to three quarters of LEAs are associated with systemic disease such as diabetes mellitus and peripheral arterial disease. In developing nations, amputations are more commonly performed due to trauma, infection, or cancer.2–4 While the overall incidence of amputation has declined in the US, the proportion of amputations performed by orthopedic surgeons has increased. The decision of whether to perform an orthopedic LEA is multifactorial. The patient and medical team must carefully consider patient-specific factors (preinjury functional status, medical comorbidities), injury factors (extent of soft tissue injury, location, and contamination), and socioeconomic factors (occupation, access to a caretaker, housing accessibility). Surgical decision-making is reviewed on a case-by-case basis as management and expected outcome will vary based on a patient's unique situation. 5 Some studies showed no significant differences in postoperative outcomes at two-year follow-up between patients that had LEA versus limb salvage procedures; but patients treated with LEA had lower economic burden, shorter hospital stay, and fewer procedures. 6 The lack of consensus among experts further complicates decision-making for both the patient and their trauma team and motivates the use of supplemental patient education resources.5
Traditionally, clinicians have served as the primary reference point for patients and families for medical information. However, in today's digital age, patients often turn to internet-based resources, such as YouTube, to augment their medical fund-of-knowledge. It is estimated that over half of patients research their condition before medical consultation and over a third have turned to YouTube for health information.7,8 While online resources provide patients with direct, supplemental content, the quality and accuracy of information patients often obtain is unclear. Although YouTube is easily accessible, it has been shown to disseminate unverified and misleading medical content.9,10 This may in part be due to YouTube's search results algorithm which is based on popularity, relevancy, and view history rather than content quality or accuracy.
Accurate and complete patient education is paramount for the physician–patient relationship and shared decision-making. 11 This is particularly true in cases of serious illness and major surgery, such as LEA. While the reliability of YouTube as a patient education resource has been previously assessed in the orthopedic literature (i.e., in rotator cuff tear repair, knee arthroplasty, and posterior cruciate ligament reconstruction),12–14 there are no studies which specifically examine its utility in regard to LEA versus limb salvage. In this study, we examined and assessed the quality and reliability of YouTube videos as a source of patient education for LEA versus limb salvage.
Methods
Video identification
Educational content review of limb salvage versus amputation was completed on the largest video search engine site, YouTube. 15 The search terms “limb,” “amputation,” and “salvage” were used for index search. These terms were additionally combined to create the query string: “limb amputation versus limb salvage.” Browser history, cache, and cookies were cleared, and a private browsing window was used to prevent personalization of search results. This query initially yielded 65 videos. Videos not in English or those pertaining to veterinary medicine were excluded. No specific exclusion criteria were applied to remove videos also reviewing systemic infection indications. A final sample of 59 videos (Figure 1) was assessed. Prior orthopedic studies have used methodology in which the top 50 videos were reviewed,13,16 but due to the paucity of videos on LEA, a decision was made to perform a review of all relevant videos. For this reason, all videos meeting inclusion criteria were assessed. Videos were searched in 2022 and uploaded between 2011 and 2022.
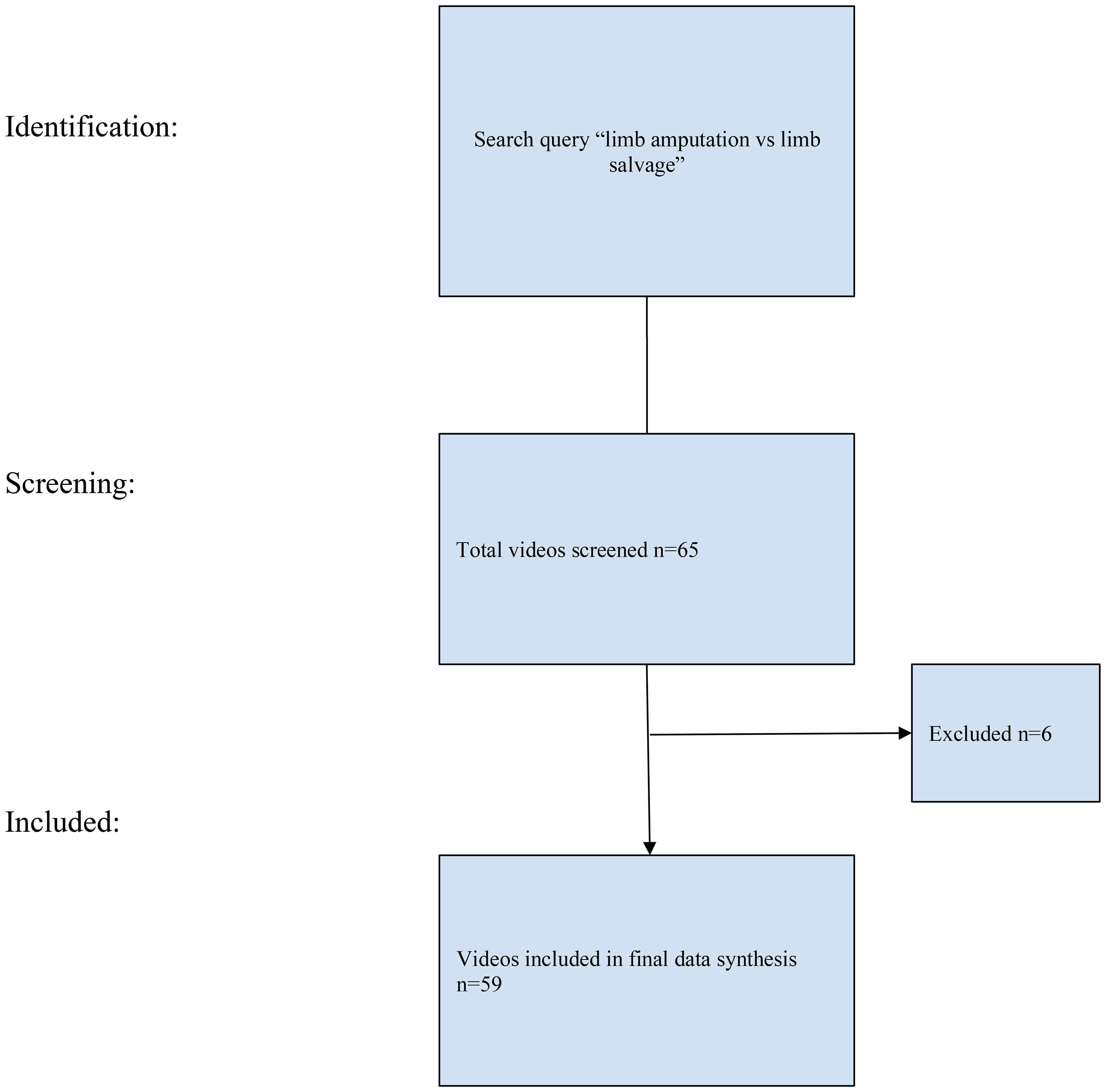
Flow chart depicting video identification and selection process.
Video data acquisition
Video characteristics that were analyzed included content creator occupation, video duration, video creation date, number of views, likes, and dislikes, and video power index (VPI) for each video were recorded. Video power index is a validated measure of video popularity used in various similar studies. 16 Video power index was calculated as like ratio×view ratio/100, where view ratio = views/day, and like ratio = like×100/like + dislike. 15 Each video sorted into subgroups based on content creator affiliation and assigned into one of the following categories: (1) “Hospital/University” (which constituted authors/uploaders with hospital or university affiliations), (2) “Physician/Physician Group “(which constituted authors/uploaders who were physicians or physician groups without hospital/university affiliations), (3) “Healthcare Professionals (which constituted authors/uploaders who were health professionals other than licensed physicians: PhDs and medical educators), and (4) “Patient Source” (which constituted authors/uploaders who were patients).
Assessment of video reliability and educational content
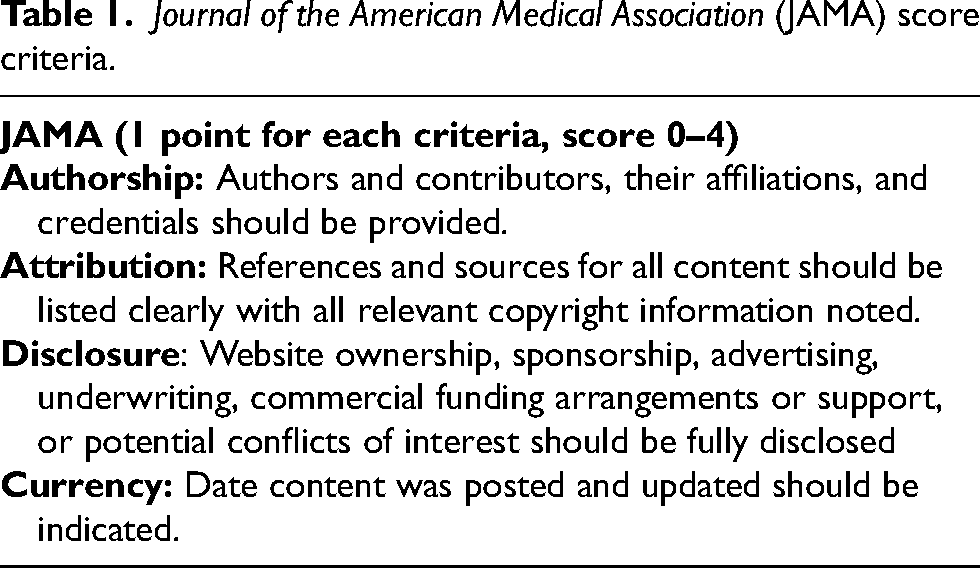
To assess the reliability of each of the included videos, the Journal of the American Medical Association (JAMA) benchmark criteria was used (Table 1). This score has been previously reported in peer reviewed in medical literature, and specifically orthopedic surgery literature, to assess reliability of online resources. 12 These guidelines served as an objective criterion to assess and score each video based on four categories: (1) Authorship, (2) Attribution, (3) Currency, and (4) Disclosure. 17 One point can be assigned for each of the categories resulting in a total score of 0–4 with 0 being the least reliable and 4 being the most reliable.
Journal of the American Medical Association (JAMA) score criteria.
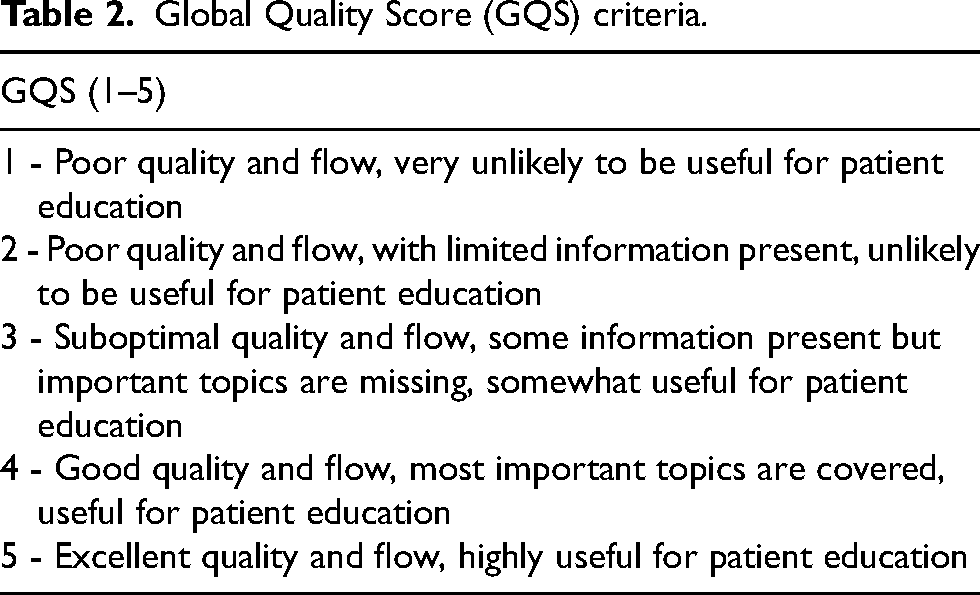
Educational quality was assessed using the Global Quality Score (GQS). The GQS system is a measure of video quality, flow, relevancy, and usefulness for patients. Scores range from 1 to 5, with a score of one being of low education utility and score of five being highly useful (Table 2). This scoring system has not yet been validated but has been used in previous peer-reviewed articles. 18
Global Quality Score (GQS) criteria.
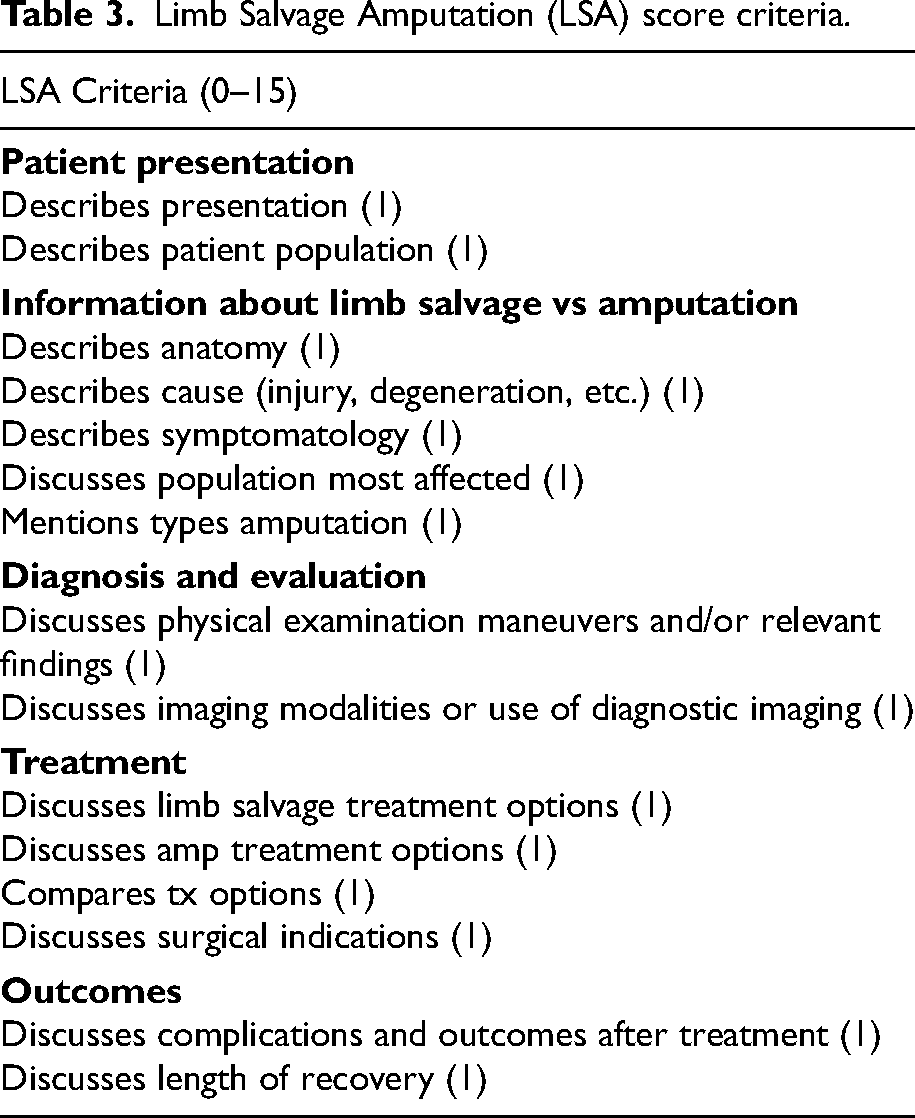
A novel scoring system was created to assess educational content quality explicitly relating to limb salvage versus amputation. The Limb Salvage versus Amputation (LSA) score was generated from 15-item criteria indicated by the American Academy of Orthopaedic Surgeons (AAOS) bulletin on amputation versus limb salvage. 19 Using the LSA criteria (score range 0–15), videos were rated by two independent medical professional observers (Table 3). In the case of scoring discrepancies, the two reviewers’ scores were averaged. This methodology for content assessment is consistent with prior publications.10,13
Limb Salvage Amputation (LSA) score criteria.
Statistical analysis
Descriptive statistics (mean, standard deviation, median, 25th, 75th percentiles, minimum and maximum values for continuous variables [video characteristics]; frequency and percent for categorical variables) were calculated for each video category. Video reliability (JAMA score) and educational quality (GQS and LPS scores) were compared according to author type. Subgroup analysis was performed comparing video quality by author type. For all analyses, the standard assumptions of Gaussian residuals and quality of variance were tested using the Shapiro–Wilk test. For normally distributed data, one-way analysis of variance and Tukey's post hoc tests were used to determine if video reliability and quality differed based on video source. For nonparametric data, the Kruskal–Wallis test, with a post hoc Dunn test to assess individual pair comparisons, was utilized. Pearson or Spearman correlation coefficients, as deemed appropriate, were used to assess the correlation between video characteristics and video quality. Multivariable linear regression was performed to characterize relationships between video duration, days up, and VPI, with video reliability (JAMA score), and educational quality (GQS and LPS scores). A result was considered statistically significant at the p < 0.05 level of significance. Analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
Search summary and video characteristics
Fifty-nine videos met the inclusion criteria, and, at the time of data collection, this group of videos accumulated a total of 714,608 views. Mean views per video were 12,025 (±54,625). Content creators associated with a Hospital/University represented 36 (61.02%) of videos and 582,958 (81.58%) of views (16,193 views/video). Physician/Physician Group author sources totaled 14 (23.73%) of videos and 113,587 (15.89%) of views (8113 views/video). Healthcare professionals (nonphysician) author types totaled 4 (6.78%) and 14,199 (1.99%) of views (3550 views/video). Patient authors totaled 5 (8.47%) of videos and 3864 (0.154%) of views (773 views/video) (Table 4).
Video characteristics.
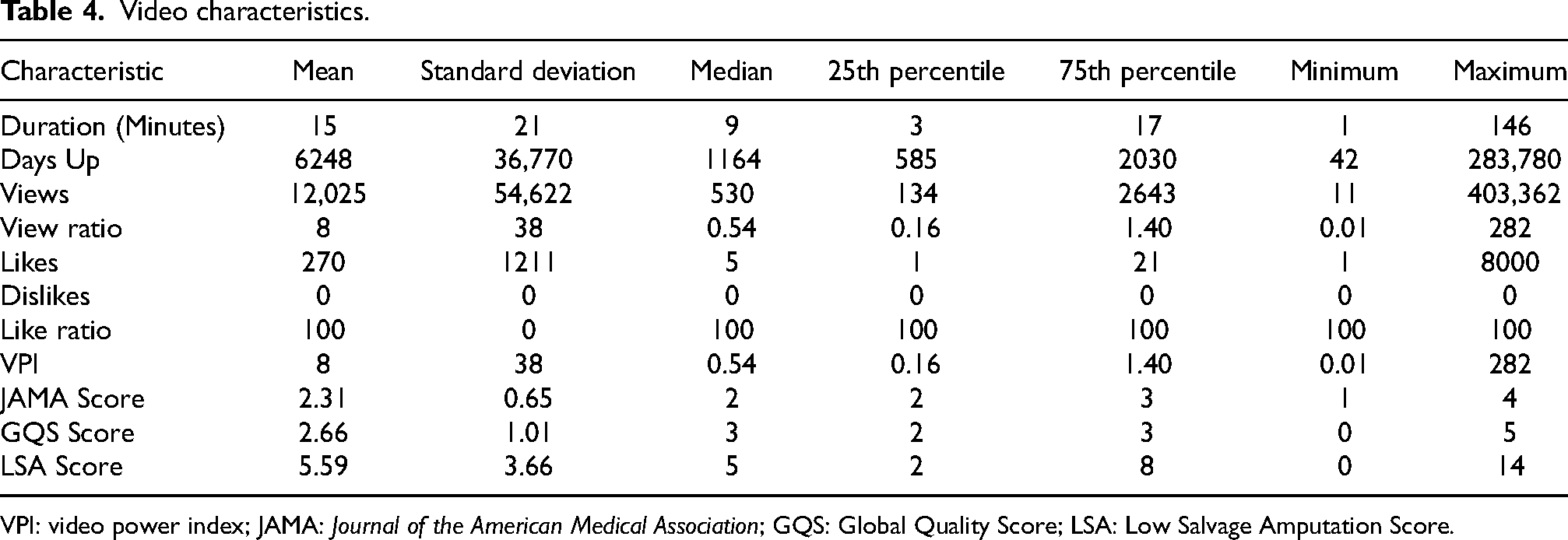
VPI: video power index; JAMA: Journal of the American Medical Association; GQS: Global Quality Score; LSA: Low Salvage Amputation Score.
Video quality according to video source and characteristics
Video educational quality was similar between author type subgroups. Journal of the American Medical Association (p = 0.084), GQS (p = 0.155), and LPS (p = 0.303) scores showed a difference that was not statistically significant. Hospital/University uploaders average scores for JAMA, GQS and LSA were 2.44 ± 0.65, 2.86 ± 0.99 and 6.11 ± 3.62, respectively. Physician/Physician Group uploader average scores for JAMA, GQS, and LSA were 2.21 ± 0.7, 2.29 ± 1.14, and 4.64 ± 3.62, respectively. Healthcare Professionals (Nonphysician) uploader average scores for JAMA, GQS, and LSA were 2.00, 2.5 ± 1.00, and 6.75 ± 4.99, respectively. Patient source uploader average scores for JAMA, GQS, and LSA were 1.80 ± 0.45, 2.40 ± 0.55, and 3.60 ± 1.52, respectively (Table 5).
Qualitative assessment of video quality according to video source.

JAMA: Journal of the American Medical Association; GQS: Global Quality Score; LSA: Limb Salvage Amputation Score.
There was a significant positive correlation between video duration and JAMA (rho = 0.35, p = 0.007), GQS (rho = 0.40, p = 0.002), and LPS (rho = 0.41, p = 0.001) scores. There was also a significant positive correlation between such as count and GQS (rho = 0.27, p = 0.04) score. No significant correlation was found between days up from upload, views, and VPI among JAMA, GQS, and LSA scores (Table 6).
Quantitative assessment of video characteristics according to quality measures.
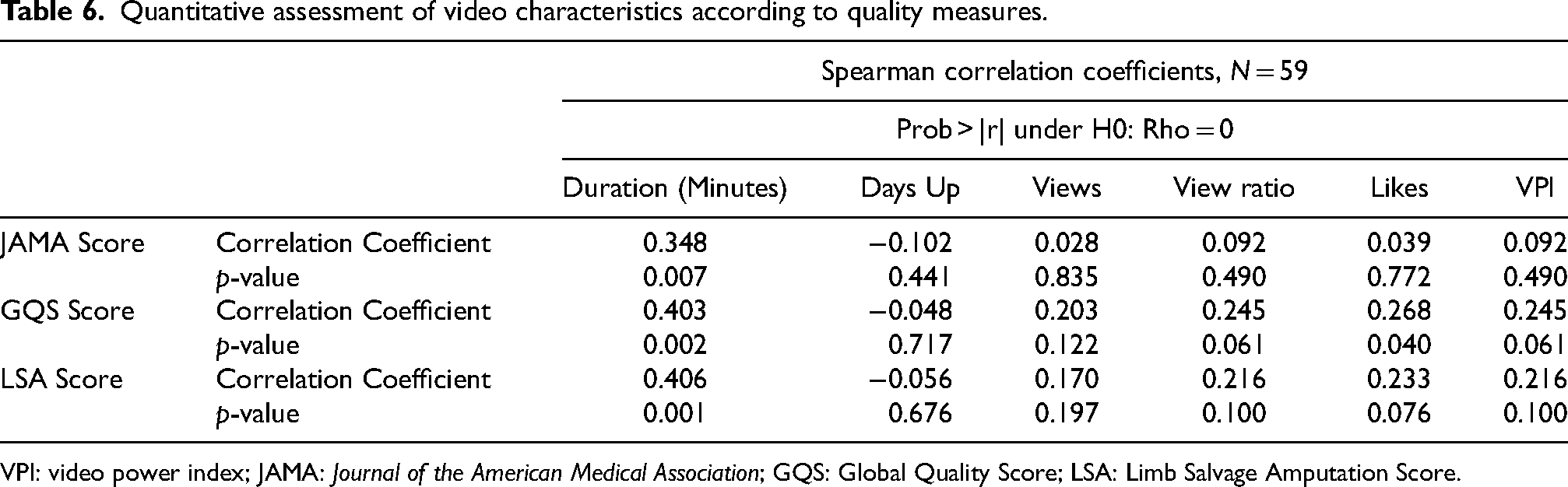
VPI: video power index; JAMA: Journal of the American Medical Association; GQS: Global Quality Score; LSA: Limb Salvage Amputation Score.
Multivariate linear regression
Multivariate linear regression was performed to assess the JAMA, GQS, and LSA scores, identifying any potential associations between the VPI and video duration. Video duration was the only significant predictor of higher JAMA (p = 0.019), GQS (p = 0.047), and LPS (p = 0.016) scores (Table 7).
Multivariate linear regression between video characteristics and educational quality scores.
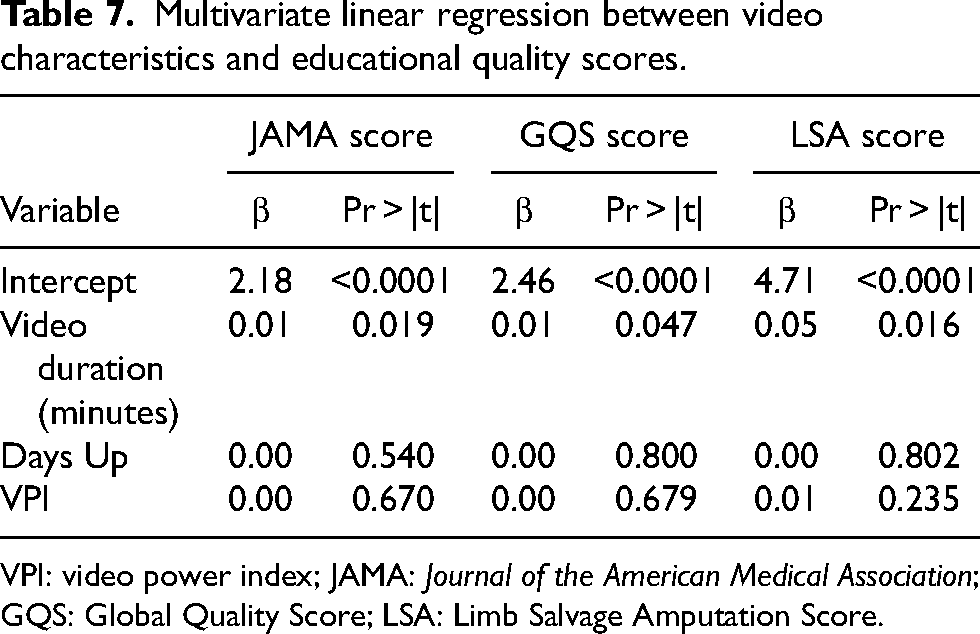
VPI: video power index; JAMA: Journal of the American Medical Association; GQS: Global Quality Score; LSA: Limb Salvage Amputation Score.
Discussion
Following a devastating lower extremity injury, patients may face the complicated, multifactorial decision to pursue LEA versus limb salvage. High-quality patient education has the potential to assist patients with this life-altering decision. Access to quality education and support has been found to improve mental health outcomes following major lower extremity trauma. 20 Over the past two decades, patients increasingly turn to the internet to provide insight into their medical conditions.21,22 YouTube has become a widely utilized tool for medical education; however, the accuracy of information provided by YouTube is often called into question.14,23,24 We sought to evaluate YouTube as a medical education tool for LEA versus limb salvage.
The mean number of views per video in our study was 12,025. Notably, the range of view count in our cohort was broad, from only 11 views to over 400,000. This mean is also lower than similar assessments of other orthopedic conditions in the literature. Wong et al. assessed knee arthritis related videos and found mean views to be 135,074. 14 Hornung et al. assessed YouTube videos related to low back pain and found average views to be 826,014. 10 Notably, these are very common conditions which likely explains the comparatively high view count. Studies on relatively less common conditions such as scoliosis and distal radius fractures have much lower viewership, less than 100,000 per video.25,26 Furthermore, measurements of average viewership are subject to methodology differences. Inherently, as researchers choose to include more videos (a larger sample cohort size), it is likely these videos will have less views, as more popular videos are more likely to appear first in YouTube's search algorithm. The topic of amputation versus limb salvage represents a relatively small population of patients, therefore, a smaller quantity of views. This is in part be due to the, often, urgent nature of traumatic LEA vs limb salvage, limiting time available for research relative to more chronic conditions.
We utilized JAMA and GQS to assess video reliability. We found JAMA and GQS scores to have a mean 2.3/4 and 2.66/5, respectively, across all videos. When broken down by video source, both JAMA and GQS were highest among videos from either hospitals/universities or physician/physician groups. Only video duration was found to significantly correlate with both JAMA and GQS, however, this correlation was weak. Regarding JAMA, a relation to duration could be expected, as taking time to disclose relevant conflicts, authorship, and sources inherently leads to longer videos. While GQS is a more subjective scale, again, increased duration allows a video to present more useful information, which is a key component to the GQS. The mean JAMA and GQS values in our study, while considered poor, appear relatively consistent with other studies assessing YouTube videos for various orthopedic conditions. Hornung et al. in their analysis of low back pain found JAMA and GQS somewhat lower than in our cohort. 10 Yüce et al. assessed videos addressing patellofemoral pain syndrome and found very poor-quality videos with 42% and 59% of videos scoring less than 2 on JAMA and GQS, respectively. 27
Our study utilized LSA score as an assessment of quality and extensiveness of specific information regarding LEA versus limb salvage covered in each video. Out of a maximum of 15 points, we found the mean LSA score across all videos to be 5.59 ± 3.66 (range 0–14). When further assessed by video source, “Healthcare Professionals (Nonphysician)” videos offered the highest LSA score followed by Hospital/University, Physician/Physician Group, and finally Patient Source. As with JAMA and GQS, only video duration offered a weakly positive, statistically significant correlation with LSA score.
Patient education regarding posttraumatic amputation versus limb salvage is particularly important due to the severity of injury and the impact on their quality of life. Unfortunately, availability and quality of information on this topic is limited. To the authors’ knowledge, there is no specific assessment of patient education materials on this topic for the traumatic setting, rather the literature focuses on oncologic or diabetic related indications. In a recent assessment of internet patient education materials for limb salvage focusing on diabetic-related indications, authors found 90% of materials were above the American Medical Association recommended 6th-grade reading level and found the quality of information to be inconsistent. 28 Evaluations of overall orthopedic trauma-related patient education materials have also been noted to be poor. Two separate analyses of the AAOS online patient education materials regarding traumatic injuries have been performed. Both found a mean of an approximately 9th-grade reading level for materials with only one and three articles judged to be at or below a 6th-grade reading level.29,30 While we did not specifically assess for understandability in our study, as stated previously, the overall quality of videos on LEA versus amputation was somewhat poor. These findings represent the need for the orthopedic academic community to provide more easily understandable, quality patient education materials for amputation versus limb salvage and for orthopedic traumatic injuries as a whole.
The majority of videos included in our cohort were from hospital/universities or physicians/physician groups. However, there were four videos from Healthcare Professionals (Nonphysician) and five videos from Patient Sources. While not statistically significant, there were some notable trends in our evaluation metrics. Journal of the American Medical Association scores in the Healthcare professionals (nonphysician) and Patient Sources tended to be lower. Global Quality Score was somewhat higher among hospital/university videos compared to other sources. Interestingly, Healthcare professionals (nonphysician) had the highest mean LSA score, followed closely by hospital/university, then somewhat lower scores for the Physician and Patient Sources. This finding is difficult to explain. It is possible that a lack of sufficient statistical power due to the sample size of the Healthcare Professionals (Nonphysician) group caused the mean to be positively affected by a particularly thorough video, as evidenced by this group also having the largest standard deviation. Further, Hospital/University authors had the largest viewership (81.58% of views) with an average of 16,193 views per video, while Healthcare professionals (nonphysician) videos (1.99% of views) were watched an average of only 3550 times per video. Compared to other similar investigations, the video sources in our study tended to be more likely from an academic or physician source and less likely from patients or nonphysician sources.10
This study has several limitations. Only the first 65 videos of our search were considered, and after removing non-English and veterinary sources only 59 were evaluated. It is, therefore, possible that the results of this study do not reflect the overall quality of all pertinent, available videos. The sample size was based on feasibility and availability of resources, and not a formal power calculation. Results from this study can be used to power a future study. Our study utilized JAMA and GQS to assess overall video reliability and quality. These are not specific to online content or videos as there is no validated tool to assess the quality of video-based health information. However, these scores have been used previously in the literature to evaluate videos with similar methodology. Furthermore, we utilized LSA to assess information specific to our topic which was developed based on the AAOS bulletin on limb salvage versus amputation. While we believe this was a useful metric, this score has not been validated. Additionally, there was no grading system utilized in our study to assess for inaccurate information. Furthermore, YouTube represents a dynamic source. Not only are new videos uploaded daily but also there are modifications to its search algorithm which could affect results. Therefore, over time the information and its quality will evolve over time and the results in this study may need to be revisited later.
Conclusion
The JAMA, GQS, and LSA scores revealed that, on average, YouTube videos about limb salvage versus amputation were of poor reliability, general educational quality, and content quality explicitly relating to limb salvage versus amputation. However, if YouTube is to be utilized as a source for patient education, both video duration and author type should be considered upon video selection. The Medical Education author type, which was associated with higher LSA scores, produced videos most geared toward general patient audiences, while the Physician/Physician Group author type, which was associated with lower LSA scores, produced videos most geared toward niche medical/specialist audiences. A gap exists in patient-facing educational resources surrounding limb salvage versus amputation and orthopedic trauma more broadly. Future directions may involve bridging this gap through physician-driven patient education initiatives, potentially implementing novel technologies such as artificial intelligence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.