
Abstract
The terrible triad literature reports data across wide ranges of patients ages and the treatment allocation for the radial head is commonly based on fracture severity. These observations raise the question of selection bias which can hinder comparative efficacy. Propensity score matching analysis may provide better control of patient variables and treatment allocation. We convey two conclusions from this analysis. Firstly, clinical outcome metrices were favorable for both radial head arthroplasty and open reduction internal fixation following terrible triad injury. This finding supports the recent literature which describe satisfactory outcomes for acute surgical management of these injuries. Secondly, the analysis suggests that revision rates may be lower for both treatment options than previously reported in the literature.
Keywords
Introduction
Terrible triad (TT) injuries of the elbow are complex injury patterns which have historically been problematic for surgeons due to high rates of complications and a lack of consensus on treatment.1,2 Hotchkiss initially used this nomenclature to describe elbow ligament injury with concomitant radial head and coronoid fractures. 3 This triad of disruption produces loss of the primary and secondary stabilizers of the elbow. 4 The most common injury mechanism involves forceful ground contact with an outstretched arm. Force transmits proximally leading to increased axial, rotary and valgus loads at the elbow causing catastrophic failure of the bony and capsuloligamentous structures.
It is now more widely accepted that surgical treatment that addresses each component of the triad of disruption improves outcomes.5–10 The radial head is a secondary stabilizer of the elbow, providing buttress support against valgus stress.11,12 Thus, repair or replacement of the radial head in TT injury is crucial in restoring elbow stability. 2 Algorithms for surgical treatment of TT injuries have been developed in order to facilitate standardized surgical intervention which have produced increasingly favorable outcomes.6,13,14
Utilization of radial head arthroplasty (RHA) is increasing,15–17 with substantial increases seen in the presence of traumatic elbow instability. 18 The driving forces behind this increase in arthroplasty utilization may include the favorable outcomes of RHA in older adults and the short-term failure rates reported for open reduction internal fixation (ORIF).5,18–21 Although short term findings for RHA are compelling, concerns remain for long term complications due to the prosthesis.5,21
Based on aggregate findings, RHA and ORIF yield equal outcomes in TT injuries22–24 but these findings may be confounded by two important selection biases. The first is inclusion of patients from a broad age range (mean 20–77, SD 14.25, N = 403).1,5,7,14,21,22,25 These reports pool results from patients with widely different postoperative functional demands. The second is the treatment allocation of ORIF to fractures of lower severity and RHA to those of higher severity. A review by Kyriacou et al. concluded a significantly higher number of Mason III fractures in the RHA (79%) group compared to the ORIF group (48%) (P = 0.0001). 22
These observations raise the question of comparative efficacy if studied in better controlled circumstances. Therefore, the objective of this systematic review was to utilize propensity score matching to compare the results RHA and ORIF in TT injury. This analysis will provide better control of patient variables and treatment allocation.
Materials and methods
Data sources
Ethics approval was not required for this work. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to structure the format. PubMed database was queried for publications with the following terms: radial head fracture AND Mayo, terrible triad AND Mayo, terrible triad AND outcomes, elbow dislocation AND Mayo, elbow dislocation AND outcomes. English language articles published prior to July 15, 2021, were available for inclusion.
Study selection
Study inclusion required stages of screening. The initial requirement was a table with individual patient reporting. Within the table, the following data were required for inclusion: patient age, patient gender, follow up term, radial head fracture classification and the reporting of a numeric Mayo Elbow Performance Score (MEPS). If the specific value of the MEPS was not provided, the study was excluded. These covariates provided the basis for propensity score matching. Further matching by injury characteristics and treatment variables were not possible due to heterogeneity of reporting. The terrible triad literature commonly classifies the radial head fracture using the Mason classification (I–IV). This variable was reported as described in the included articles. Selection was independently assessed by 2 authors.
Data extraction
The outcome measures evaluated were MEPS, Disabilities of the Arm, Shoulder and Hand (DASH), failure/revision of the surgical construct, and the functional parameters of elbow arc of flexion/extension and forearm arc of rotation. Revision data represents all-cause revision. Additionally, revision cases were excluded therefore the outcomes analyzed represented primary surgical intervention.
Propensity score matching
Propensity score matching (PSM) provides statistical analysis based on individual patient covariates in order to better equalize potential confounding factors. 26 By limiting selection bias, causal effects can be derived from the data which strengthens the conclusions. PSM application has increased due to the monetary cost and time investment associated with prospective randomized study designs. 27 Covariates used to match patient pairs included age, gender, term of follow up, and fracture classification. Matching was done using the matchit package within R software (Lucent Technologies, Murray Hill, NJ, USA). The method used was nearest neighbor with caliper set to 0.1. 28 The caliper determines the allowable difference between values of the covariates. The caliper used for this analysis maintained a narrow range of allowable variance between matched pairs for the covariate values. 29
Data synthesis
Pearson's chi square with Yates’ continuity correction was used to determine trends in treatment based on patient gender. Fisher's exact test was used to determine trends in treatment based on radial head fracture classification. Wilcoxon rank sum test was used to compare the follow up term between treatment groups given the non-normal distribution of the sample. Pearson's chi square test, Fisher's exact test and Student t-test were used to compare matched pair data. Significance level was set at P < 0.05.
Results
Following appropriate exclusions, the database query generated 15 articles which met the inclusion criteria (Figure 1). Within the included articles, analysis was based on 77 cases of RHA (mean age 49 years, mean follow up 43 months) and 97 cases of ORIF (mean age 42 years, mean follow up 36 months).
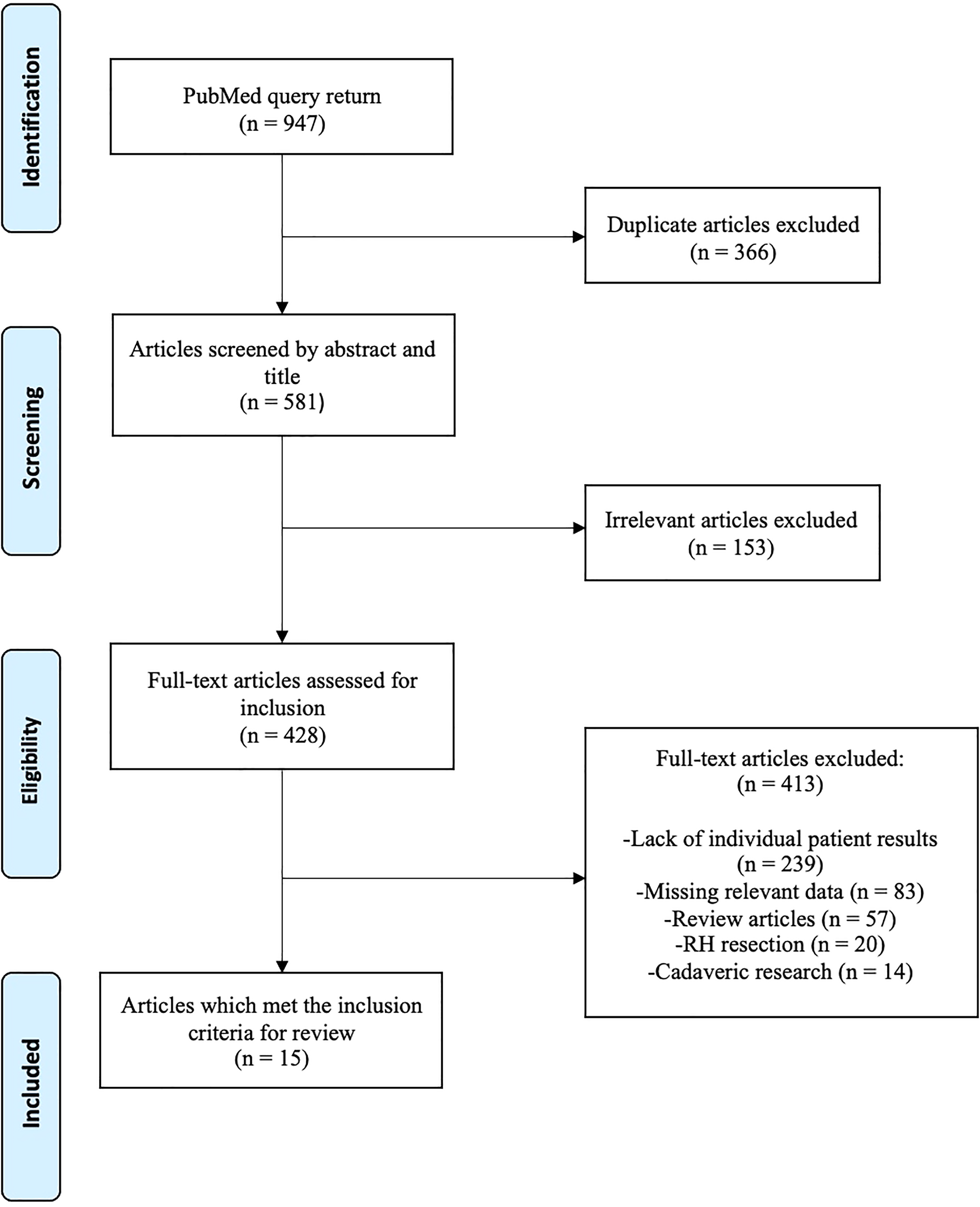
Flowchart depicting literature search and article selection process with exclusion criteria.
Propensity score matched pairs
Sixteen (16) patients with Mason III fractures were matched from the RHA and ORIF groups for outcome comparison (Table 1). When matched for age, gender and follow up term, MEPS (P = 0.90) and DASH (P = 0.80) comparisons between RHA and ORIF were not significant. Consistent with the finding across the entire sample, patients with Mason III fractures who were treated with RHA were significantly older than patients with Mason III fractures who were treated with ORIF (P = 0.02).
Covariate and outcome comparison between RHA and open reduction internal fixation for Mason III fractures in terrible triad injury.
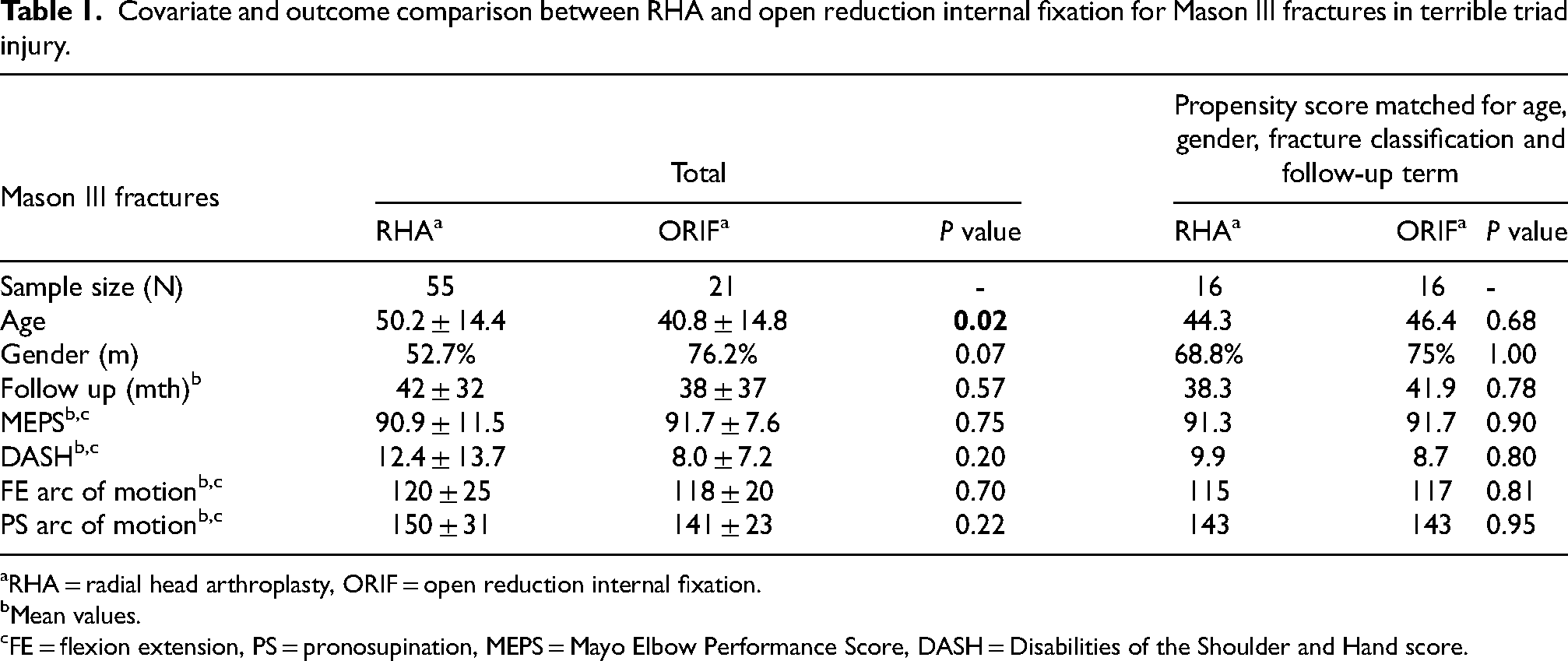
RHA = radial head arthroplasty, ORIF = open reduction internal fixation.
Mean values.
FE = flexion extension, PS = pronosupination, MEPS = Mayo Elbow Performance Score, DASH = Disabilities of the Shoulder and Hand score.
Overall sample
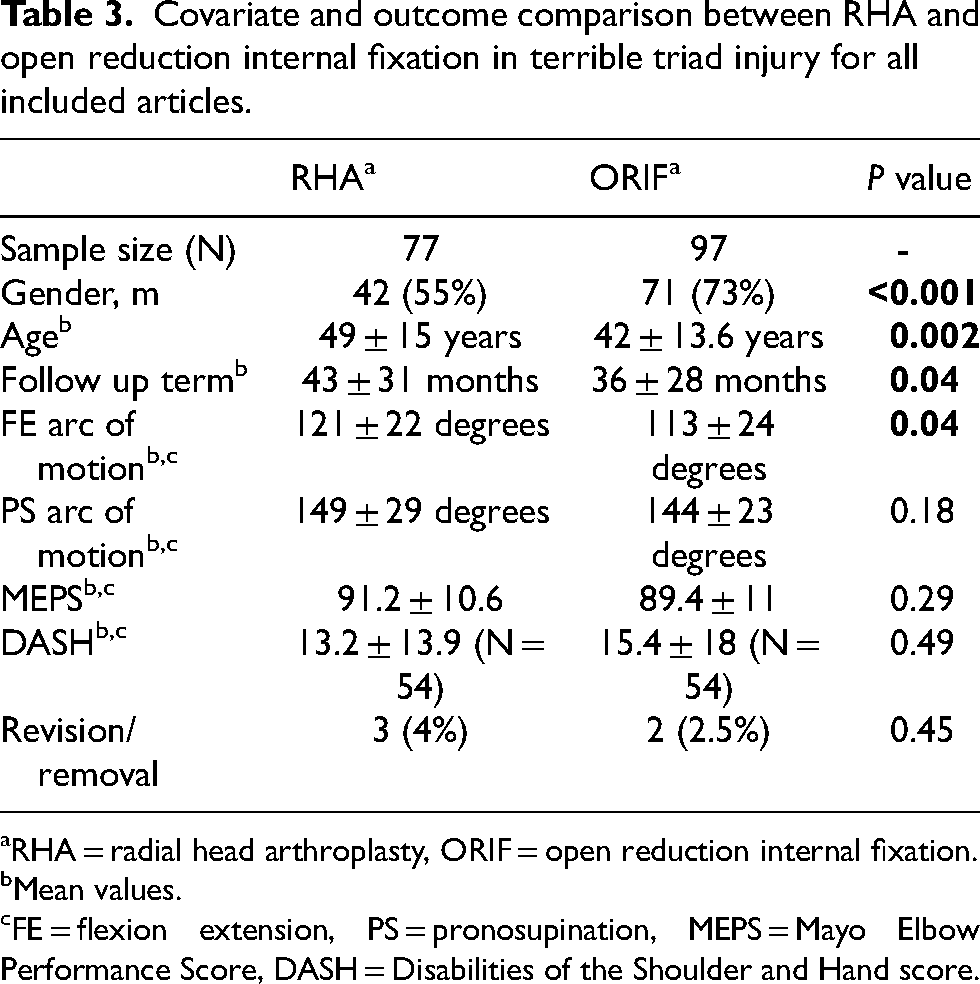
Mean age was significantly higher in the RHA group compared to the ORIF group (P = 0.002). Evaluating treatment method and gender, males were significantly more likely to be treated with ORIF while females were significantly more likely to be treated with RHA (P = 0.01) (Table 2). Evaluating treatment method and radial head fracture classification, patients were significantly more likely to be treated with RHA with increasing levels of Mason fracture classification (P < 0.01) (Table 2). Comparisons between the RHA and ORIF groups are shown in Table 3. Comparison between ORIF and RHA for categorical MEPS is shown in Figure 2 and for DASH scores in Figure 3.
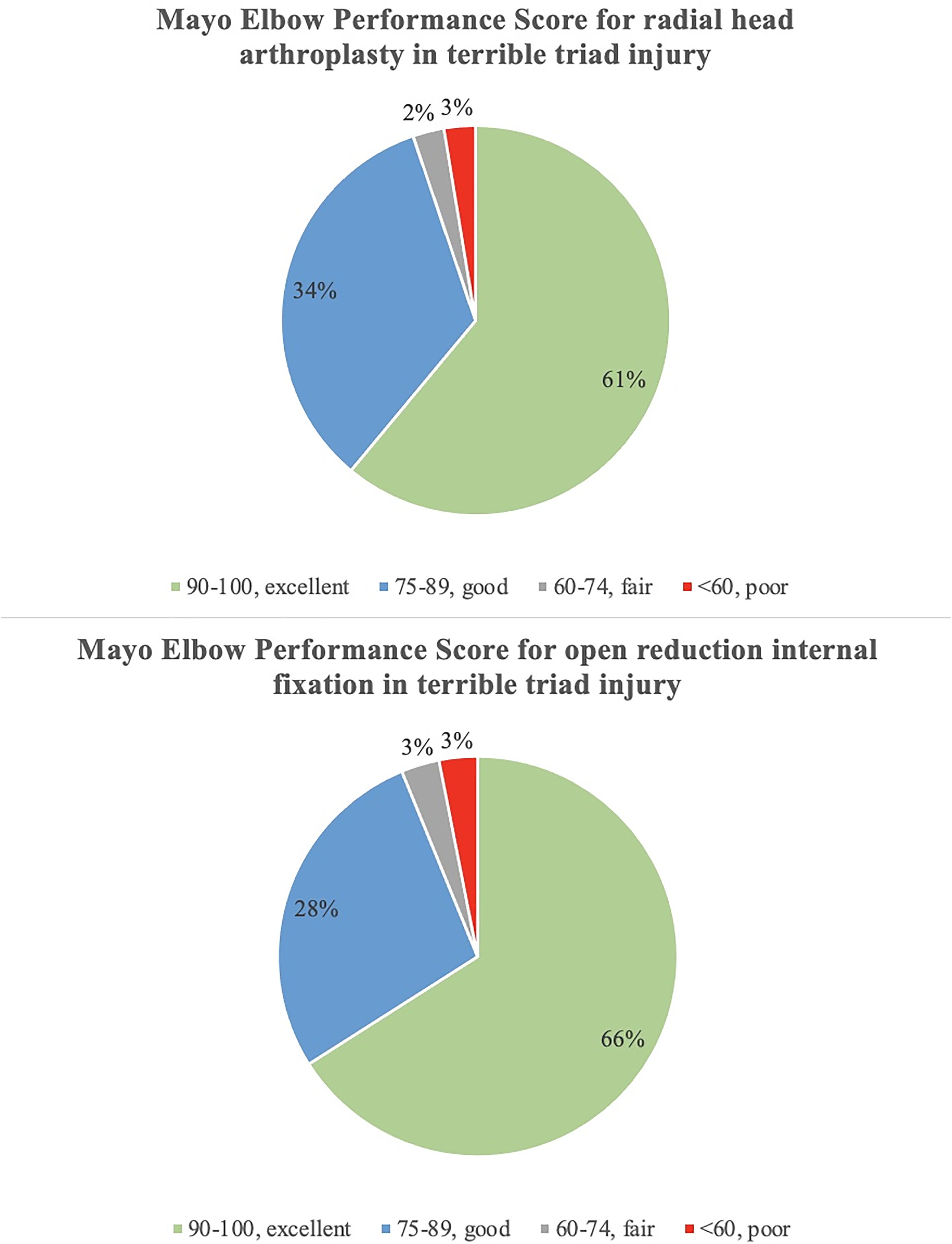
Mayo elbow performance scores for RHA and open reduction internal fixation in terrible triad injury.
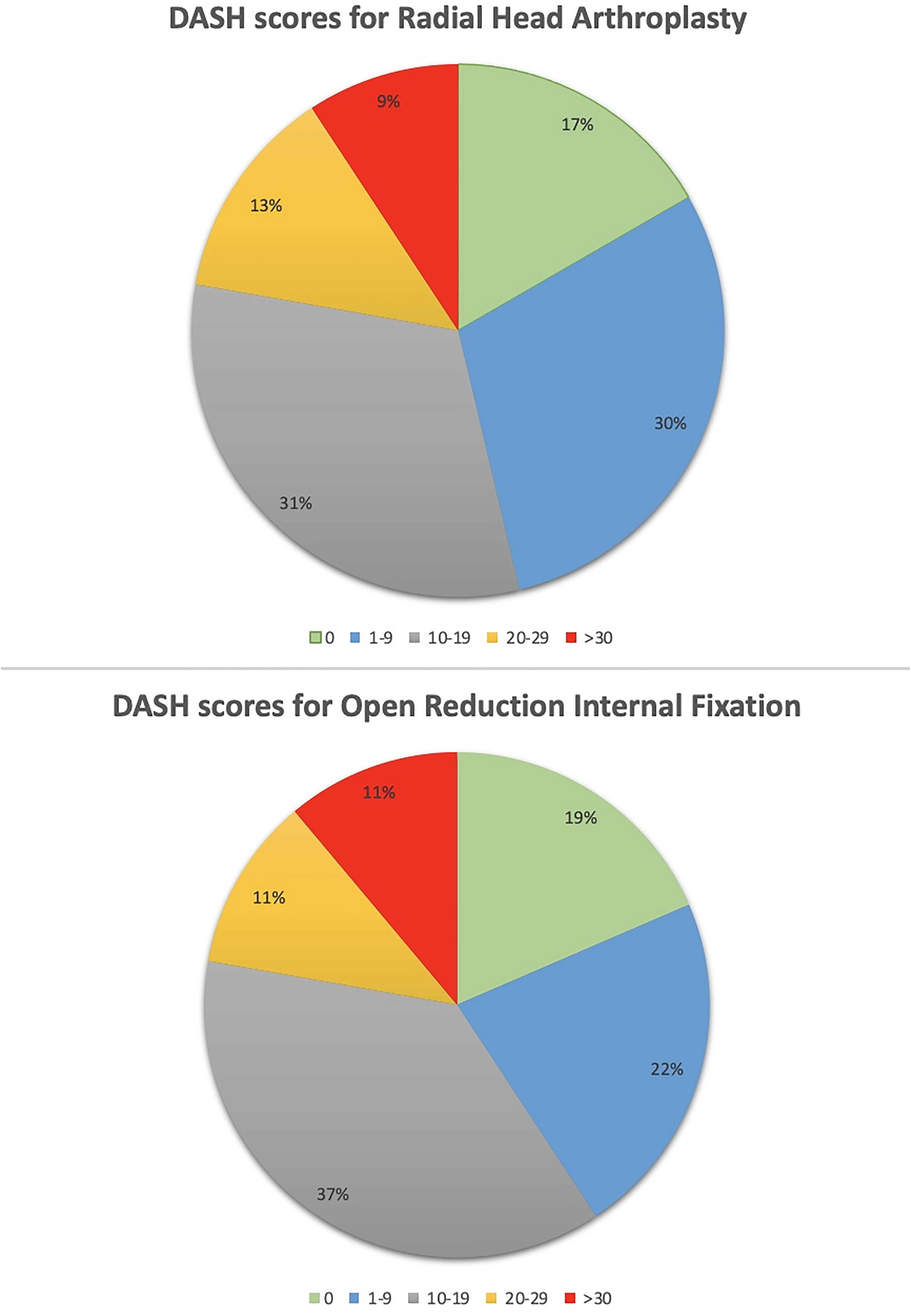
Disabilities of the arm, shoulder and hand scores for RHA and open reduction internal fixation in terrible triad injury.
Trends for radial head treatment method in terrible triad injury based on gender and fracture classification.
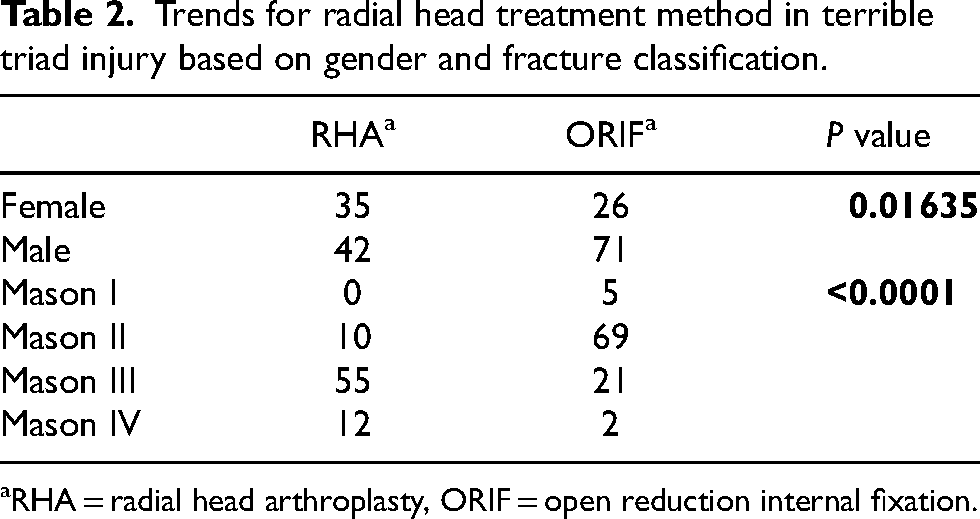
RHA = radial head arthroplasty, ORIF = open reduction internal fixation.
Covariate and outcome comparison between RHA and open reduction internal fixation in terrible triad injury for all included articles.
RHA = radial head arthroplasty, ORIF = open reduction internal fixation.
Mean values.
FE = flexion extension, PS = pronosupination, MEPS = Mayo Elbow Performance Score, DASH = Disabilities of the Shoulder and Hand score.
Discussion
Propensity score matching is a statistical method that reduces the confounding potential of selection bias.28,30 This novel application of PSM in a systematic review generated 16 matched pairs for Mason III radial head fractures in TT injury. Our overall results demonstrate favorable outcomes for RHA and ORIF which differ from some existing reports. 25 Further, functional outcomes and MEPS were not significantly different between RHA and ORIF. While the conclusion of similar clinical outcomes between RHA and ORIF is consistent with some reports, 22 our results showing low rates of ORIF failure are in contrast with some of the literature.5,18,19,21 In totality, these results demonstrate that prospective randomized trials for this complex fracture pattern can be confidently and ethically initiated due to the favorable outcomes between these 2 treatment methods.
The literature has demonstrated a shift in radial head fracture management which may not be completely validated by the currently available data. Utilization of RHA is increasing, due in part to favorable outcomes in RHA and reports of short-term failure in ORIF.5,21 Across the pooled data of 97 ORIF cases, 1 case was revised due to malunion, and 1 case required reoperation due to failure of the LCL repair, equating to a reoperation rate of 2.5%. Therefore, our results suggest a low rate of ORIF reoperation at a mean patient age of 42 and a mean follow up of 36 months. This finding is in contrast to prior reports of high reoperation rates for ORIF following TT injury, ranging up to 33% (mean age 42 years, mean follow up 41 months) and 44% (mean age 48 years, mean follow up 18 months).5,21 Reoperations following ORIF may be due to the complexity of the injury pattern,1,31 disruption of the vascular anatomy of the radial head,32,33 and the surgical dissection required for anatomical reduction and fixation.1,31
Although RHA continues to gain momentum due to favorable outcomes, these findings have been less demonstrable in the terrible triad literature. Our pooled data across 77 arthroplasties yielded a 4% rate of revision at a mean follow up of 43 months. This finding is in contrast to a previous review which calculated rates of revision exceeding 40% for RHA in TT injury (mean age 50 years, mean follow up 36 months). 34 Arthroplasty failures are due to inappropriate prosthesis size and position which may lead to painful aseptic loosening.35,36 Lengthening of the radius with the prosthesis—termed joint overstuffing—can lead to alterations in ulnohumeral and radiocapitellar pressures which can predispose to degenerative changes. 37 Symptoms due to overstuffing include pain, stiffness, loss of motion, and aseptic loosening. Rates of loosening may vary based on polarity and stem fixation.36–38 The aggregated results for RHA and ORIF reinforce the increasing body of evidence which describe satisfactory outcomes following acute surgical management of terrible triad injury.1,6,25,36,39,40
Weaknesses of this review include the inherent limitations of amalgamating the work of others into a cohesive summary. Measurement bias from multiple practitioners and the variation in diagnostic and surgical skill may confound the current work. Matching cases by fracture classification allowed analysis on a specific fracture pattern but this classification does not account for displacement. Mason III fractures represent a wide spectrum of injury severity. The magnitude of injury severity may be a more important variable than fracture pattern when determining surgical treatment. The inclusion criterion of individual case reporting and MEPS was necessary for application of propensity score matching but reduced the available sample of literature and may bias the results. Further, this statistical analysis yielded a small sample for comparison of ORIF and RHA. Changes in the parameters within propensity score matching may alter the sample size and the similarity of the covariates. Revision/reoperation was aggregated for the entire sample however due to insufficient reporting this variable was not included in the propensity score matched analysis. Further, revision/reoperation was not a component of the inclusion criteria thus, our conclusions therein are limited. Finally, the current work compared treatment options for radial head fracture in terrible triad injury. Clinical outcomes for these injury patterns are also influenced by the magnitude of coronoid fracture and the subsequent treatment of this component of the injury. Strength of the current work include the broad search parameters which returned an appropriate volume of literature. The applied statistical analysis homogenizes the outcomes and provides a reproducible foundation for future review work. The intended consequence of a systematic review is to derive generalizable conclusions from a large albeit variable sample. Utilizing propensity score matching, a more specified conclusion may be obtained. Matching patients for fracture classification, age, gender and follow-up term allowed better control of some of the confounding variables which are inherent to systematic reviews.
Conclusion
In summary, we convey two conclusions from this analysis. Firstly, clinical outcomes were favorable for RHA and open reduction internal fixation following terrible triad injury. This finding supports the recent literature which describe satisfactory outcomes for acute surgical management of these injuries. Secondly, the analysis suggests that revision rates may be lower for both treatment options than previously reported in the literature.
Footnotes
Acknowledgments
The authors appreciate the support of Rachel Elaine York.
Declaration of conflicting interests
The authors would like to declare the following conflict of interest with respect to the research, authorship, and/or publication of this article: Deana Mercer, speakers bureau Skeletal Dynamics, Axogen.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.