
Abstract
The technique of ultrasound-guided regional anesthesia has demonstrated satisfactory efficacy and safety in fixation of various fractures. There are limited studies performed concerning the applicability of a surgeon self-performed ultrasound-guided regional anesthesia. This study aimed to evaluate the efficacy of a self-performed ultrasound-guided regional anesthesia by surgeon for distal radius fracture fixation in terms of intraoperative and post-operative characteristics.
Keywords
Introduction
Distal radius fracture is one of the most common injuries among upper limb trauma. 1 Significant malalignment can lead to devastating outcome to patients’ function and therefore operative management is often warranted for indicated patients. 2 Open reduction and internal fixation with plating and screws is often performed for this type of injury.
The aim of operation is to allow anatomical reduction of the fracture and stable fixation for healing at optimal position. General or regional anesthesia are often performed in those patients to allow painless experience for patients throughout the operation. 3 Regional anesthesia is routinely performed by anesthetists in many centres in Hong Kong. Due to shortage of anesthetist manpower in our centre, we adopted the ‘All Surgeons Led Regional Anesthesia’ program in which the regional anesthesia was carried out by well-trained orthopaedic surgeons with the use of ultrasound guidance.
According to our knowledge, there are very few publications in the literature regarding the surgeons’ self-performed ultrasound-guided regional anesthesia, particularly for patients suffered from a traumatic condition. In various literatures, the feasibility of surgical treatment of traumatic conditions under regional anesthesia performed by anesthetist was well proven. 4 However, there is lack of conclusive literature proving surgeons can perform the same degree of effective anesthesia.
The aim of this study was to investigate whether the regional anesthesia, performed by orthopaedic surgeons, is a safe and acceptable technique for fixation of distal radius fracture.
Patient and method
Research design and object
The retrospective study was conducted with 12 patients (2 males, 10 females; Mean age 60.6, range 16–78) who underwent open reduction and internal fixation for distal radius fracture at our centre from August 2023 to January 2024. All patients included in the study accepted the surgery to be performed with regional anesthesia by trained orthopaedic surgeons of our department.
Inclusion and exclusion criteria
The inclusion criteria were adults suffered from distal radius fracture with fixation done under ultrasound-guided regional anesthesia performed by orthopaedic surgeons.
The exclusion criteria for fracture fixation under regional anesthesia in our program were as follows:
Paediatric patients, Uncooperative psychiatric or demented patients, patients with uncontrolled bleeding tendency, patients with poor soft tissue condition at site of anesthesia injection and surgeries performed under general anesthesia or regional anesthesia by anesthetists.
Data collection
Patients’ basic information, including sex, age, injury date, side and type of injury by AO classification were collected according to medical record. The type of operation, mode of regional anesthesia, operative time and blood loss was referred by the operative records. Post-operative length of stay was referred by the discharge summary of the patient. Base on the visual analog scale (VAS) from 0 to 10, patients were told to grade the degree of pain control during operation and 6 h post-operatively.
Anesthesia technique
Anesthesia was carried out by trained group specialists orthopaedic surgeon at our centre, who would also subsequent performed the operation after anesthesia. We performed the axillary regional anesthesia for blockage of median, ulnar, radial and musculocutaneous nerve. A 20 mL of mixture was prepared with 10 mL 2% lignocaine with 1: 200,000 adrenaline and 10 mL 0.5% levobupivacaine. The volume of mixture used was tailored according to individual patients’ body weight.
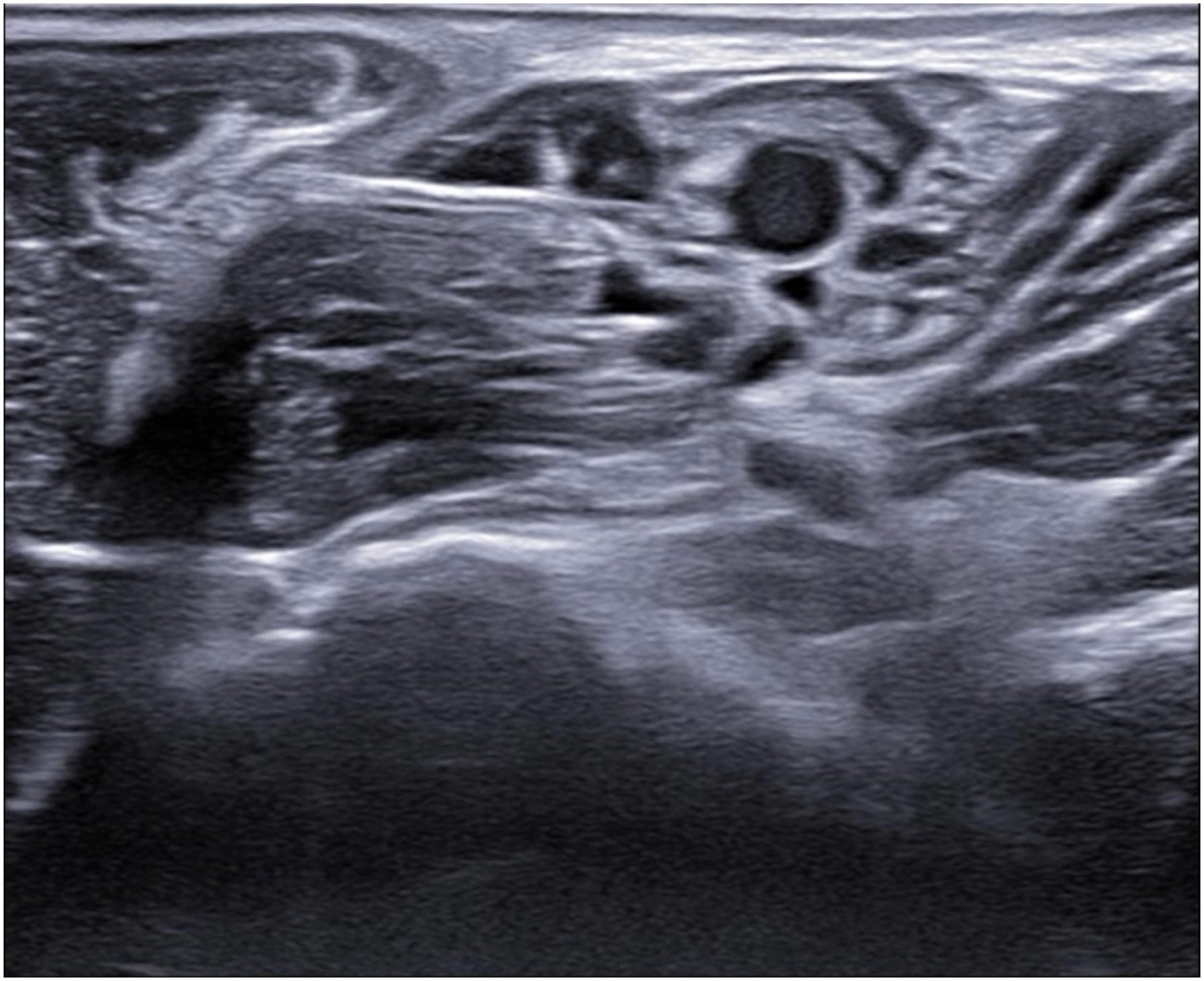
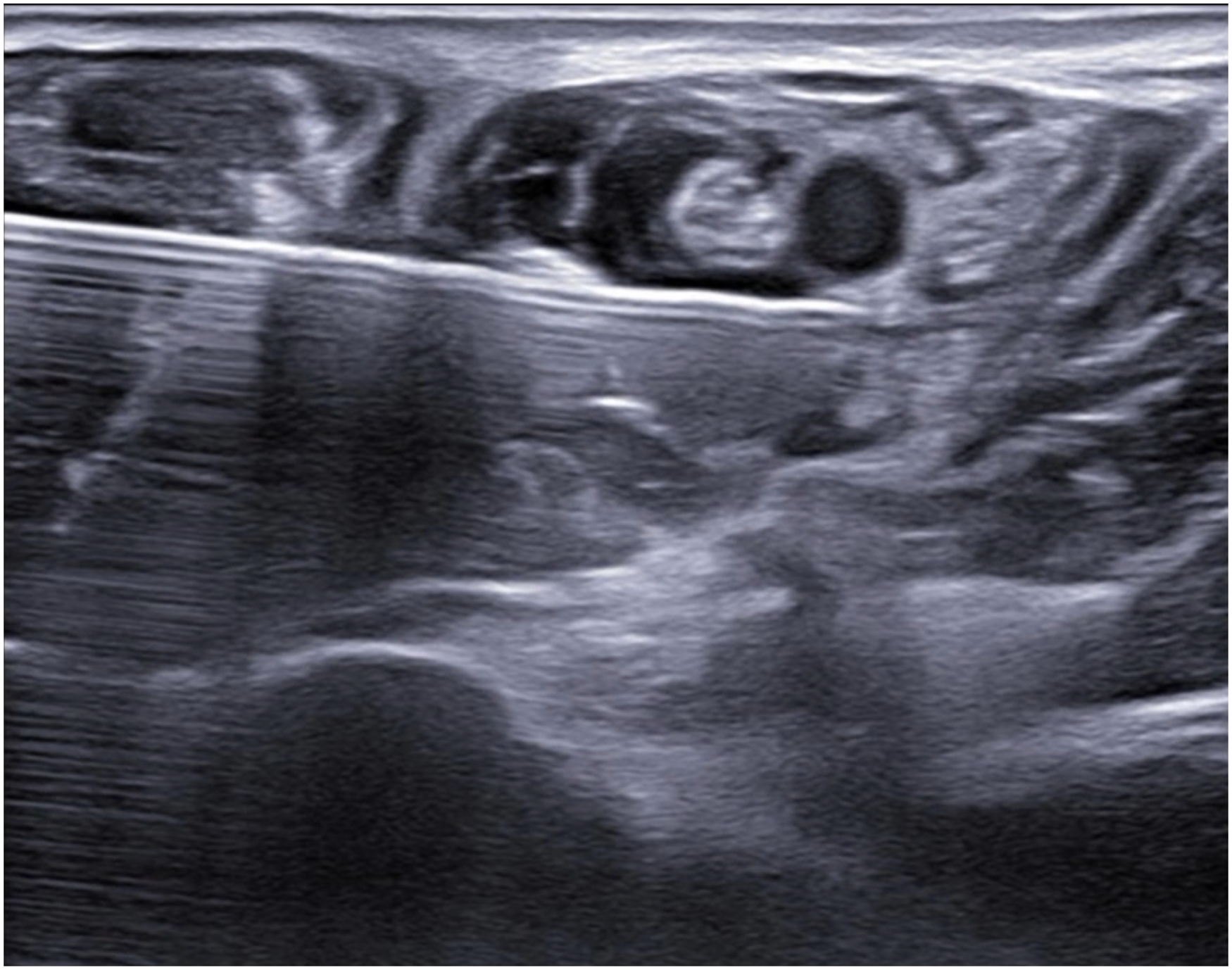
Ultrasound examination at level of axilla was performed to identify the axillary artery, vein, median, ulnar, radial and musculocutaneous nerve. Infiltration of anesthetic agent mixture to respective nerves was performed under ultrasonic guidance as shown in Figures 1–7.
Needle tip was visualised under ultrasound at all time. Injection was performed after negative aspiration with no blood. Resistance was ensured not excessive during injection. Painful numbness was looked for and avoided during injection.
Surgical technique
The operations were performed by the specialist surgeons after performing the regional anesthesia. The operation would carried out with meticulous hemostasis without the use of tourniquet. We adopted the modified Henry approach for all the patients. Dissection by layers were done with flexor carpi radialis retracted medially. Pronator quadratus was incised for fracture site exposure. Fracture haematoma was cleared, and open reduction of the fracture was performed under fluoroscopy guidance. Fixation with Synthes 2.4 mm variable angle distal radius anatomical plate and screws were performed. Surgical wound would then be closed in layers, and surgical drain was not necessary.
Follow-up
All patients were assessed and monitored throughout the operation. Pain control intraoperatively and 6 h post-operatively were assessed and documented. Panadol and tramadol would be used as standard oral analgesics regimen if the pain was deemed intolerable to patient at 6 h post-operatively.
Result
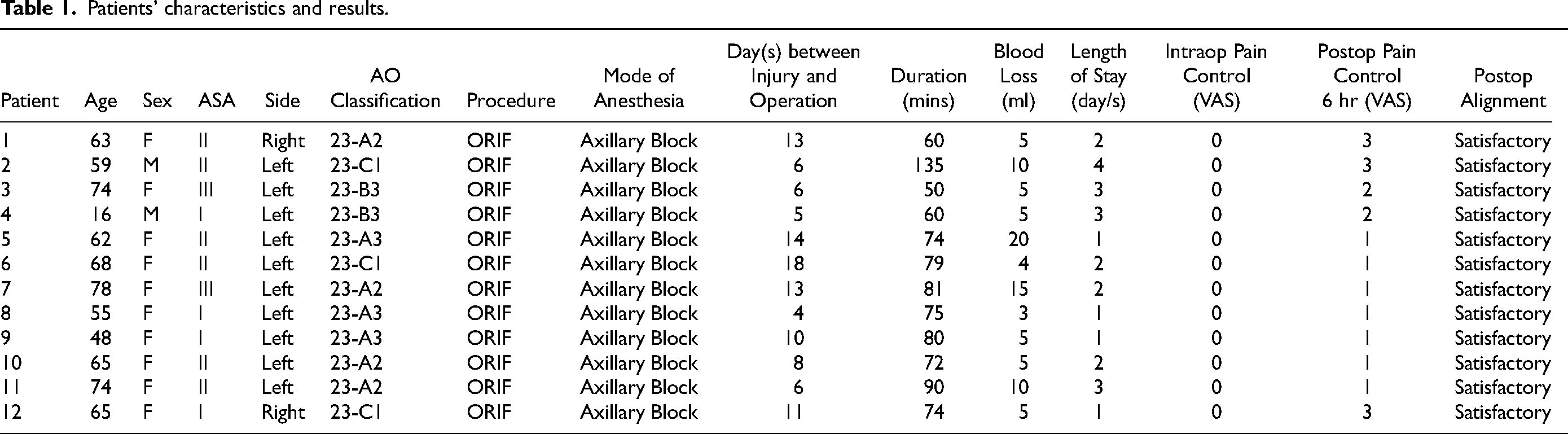
There were 2 men and 10 women included in the study. The average age of the population is 60.6 (range 16–78) years. All of them suffered from distal radius fracture with volar plating performed, of which 10 of them suffered from left-sided injury. All patient had operation performed within two weeks from the injury except one patient who have delayed surgery due to interval fracture displacement noted at follow-up. As for the fracture pattern: four patients suffered from 23-A2 type, three patients suffered from 23-A3 type, two patients suffered from 23-B3 type and three patients suffered from 23-C1 type. All of them experience complete pain control with VAS 0 throughout the operation. Average operative time was 77.5 min. Average blood loss was 7.7 mL. We achieved satisfactory pain control at 6 h post-operatively ranging from VAS 1 to 3 (VAS 1: seven patients, VAS 2: two patients, VAS 3: three patients). No patient requested oral analgesics at 6 h post-operatively. There was no complication arising from the regional anesthesia in all patients. Post-operative X ray of all patients’ wrist showed satisfactory alignment according to objective radiological criteria suggested by Lalone 4 (Table 1).
Patients' characteristics and results.
Discussion
Regional anesthesia provides improved post-operative analgesia and reduced pain intensity, less post-operative symptoms such as nausea and vomiting and better patient satisfaction while compared to general anesthesia. 5 Traditionally, peripheral nerve blocks rely heavily on anatomical surface landmark. The traditional technique also rely on the tactile sensation of fascial clicks, loss of resistance and neurostimulation for peripheral nerves with a motor component. More reliable regional anesthesia was made possible after the introduction of ultrasound guidance in the second millennium. 6 With the use of ultrasound guidance, the needle placement at site without an anatomical or bony landmarks was made possible. The risk of inner structure as well as neurovascular injury during needle advancement can also be minimised while the inner structures became well visualised in ultrasound. Literatures and researches concerning ultrasound-guided regional anaesthesia of the upper limb continue to grow and also concluded earlier sensory onset and better block success compared with landmark-based techniques. 7
Distal radius fracture accounted for nearly 20% of fractures in the active elderly population. 8 The estimated cost of treating distal radius fractures in older patient in 2025 is $600 million in the United States. 9 The cost of health care would possibly be increased by unplanned hospital admission and prolonged hospital stay caused by suboptimal pain control and persistent nausea and vomiting after general anesthesia. 10 It was proven that the application of regional anesthesia in hand and wrist surgery could result in a significant decrease in post-operative recovery room observation time, fewer post-operative complications and associated unplanned admissions, resulting in a significant decrease in perioperative costs.11,12 From our study, we also noted there were short post-operative hospital length of stay for all patients. We are optimistic about the likelihood of significant healthcare cost reduction with the use of regional anesthesia in treatment of distal radius fracture patients.
‘Regional anesthesia’ was first described by American Surgeon Dr Cushing in 1902 in which cocaine was applied to nerve trunks in to provide anaesthesia covering an operative field. 13 In older days, regional anesthesia was a surgeon-performed procedure until 1920 when percutaneous technique started to develop. 14 Combined with the blooming development of the specialty of anesthesiology, regional anesthesia increasingly became a procedure routinely performed by anesthetist. In fact, the use of ultrasound for injection or infiltration at or around an anatomical structure is not uncommon for an average orthopaedic surgeon. After acquiring the knowledge concerning the pharmacological characteristics of anesthetic agents as well as the knowledge regarding management of possible complications, for example, local anesthetic systemic toxicity, it is believed that a well-trained orthopaedic surgeons can carry out regional anesthesia as effective as an anesthetist without compromising safety and quality of fracture fixation and alignment.
The limitation of this study includes its retrospective nature which may lead to bias in the information as well as inaccuracy due to recall. This study mainly focus on the intraoperative and early post-operative pain control from the regional anesthesia. Functional outcome in short term as well as long term from the operation was not studied.
Conclusion
According to our centre's experience, regional anesthesia performed by orthopaedic surgeon could provide comfortable and pain-free experience during fixation of distal radius fracture.
The same principle maybe applied to other traumatic or elective orthopaedic conditions requiring regional anesthesia. However, further studies need to be continued for adequate power for formal analysis of feasibility.

Patient positioning and setting for application of regional anesthesia.

Needle insertion for application of regional anesthesia under ultrasound guidance.
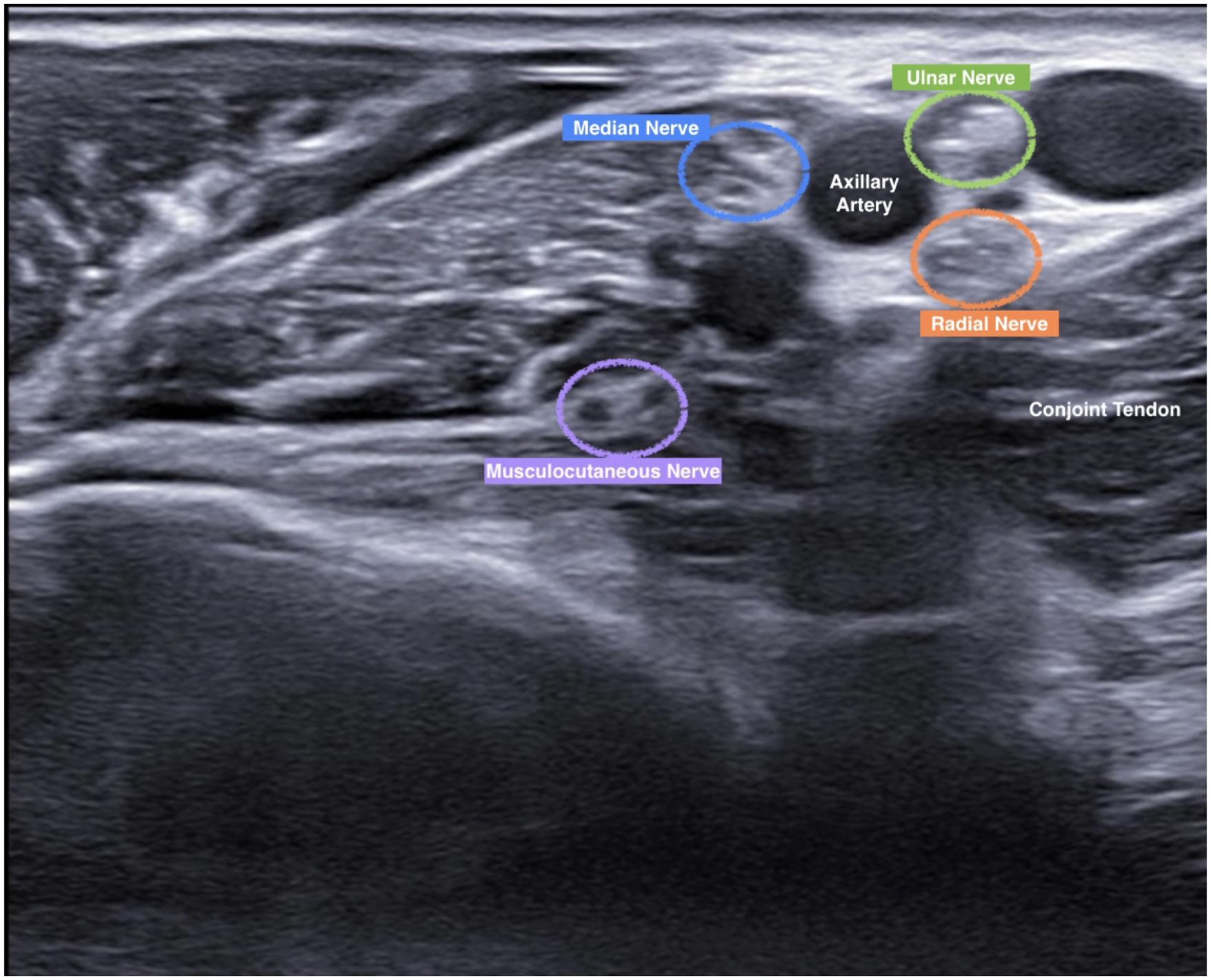
Ultrasound image of various structure.
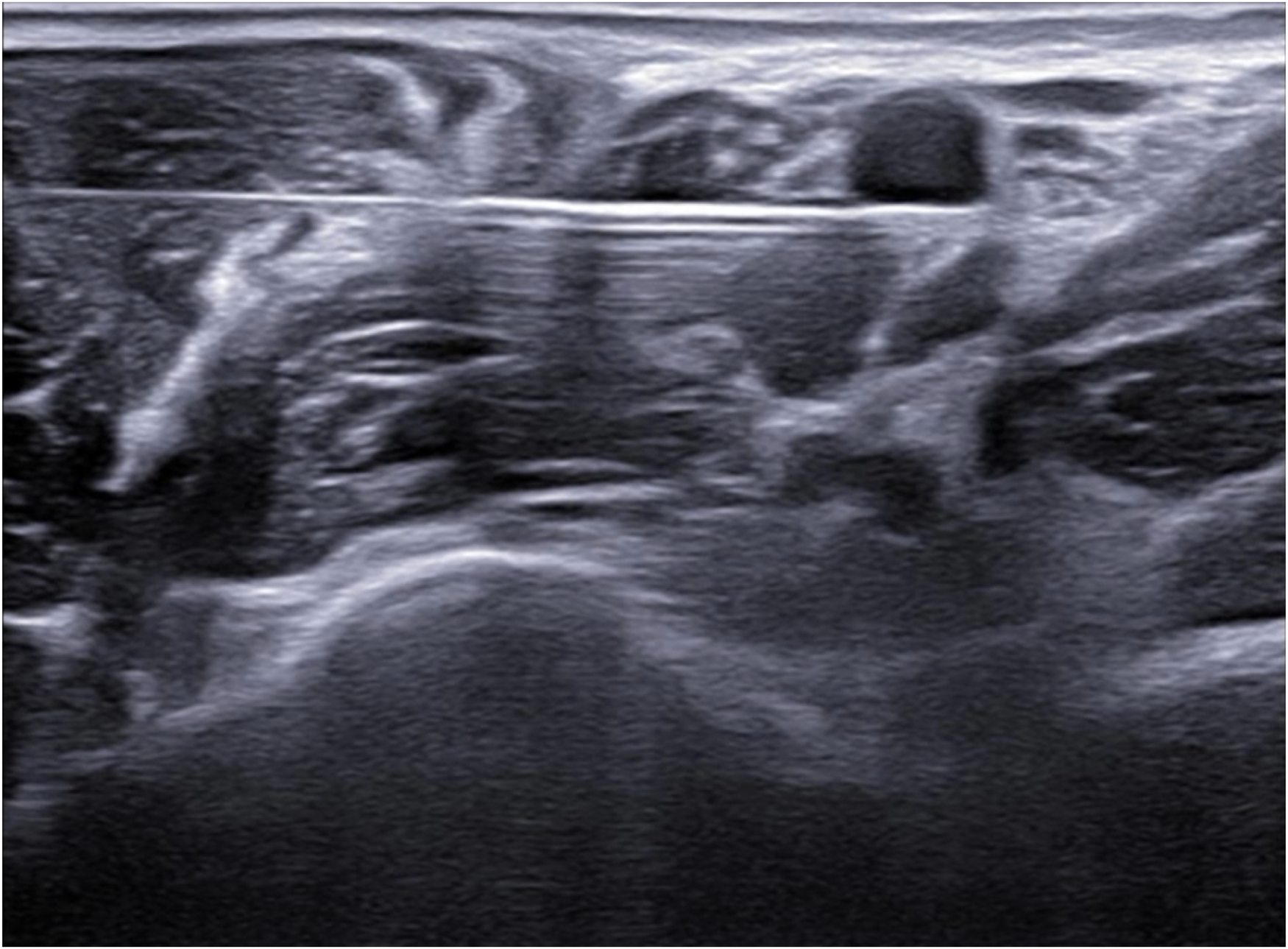
Radial nerve block.
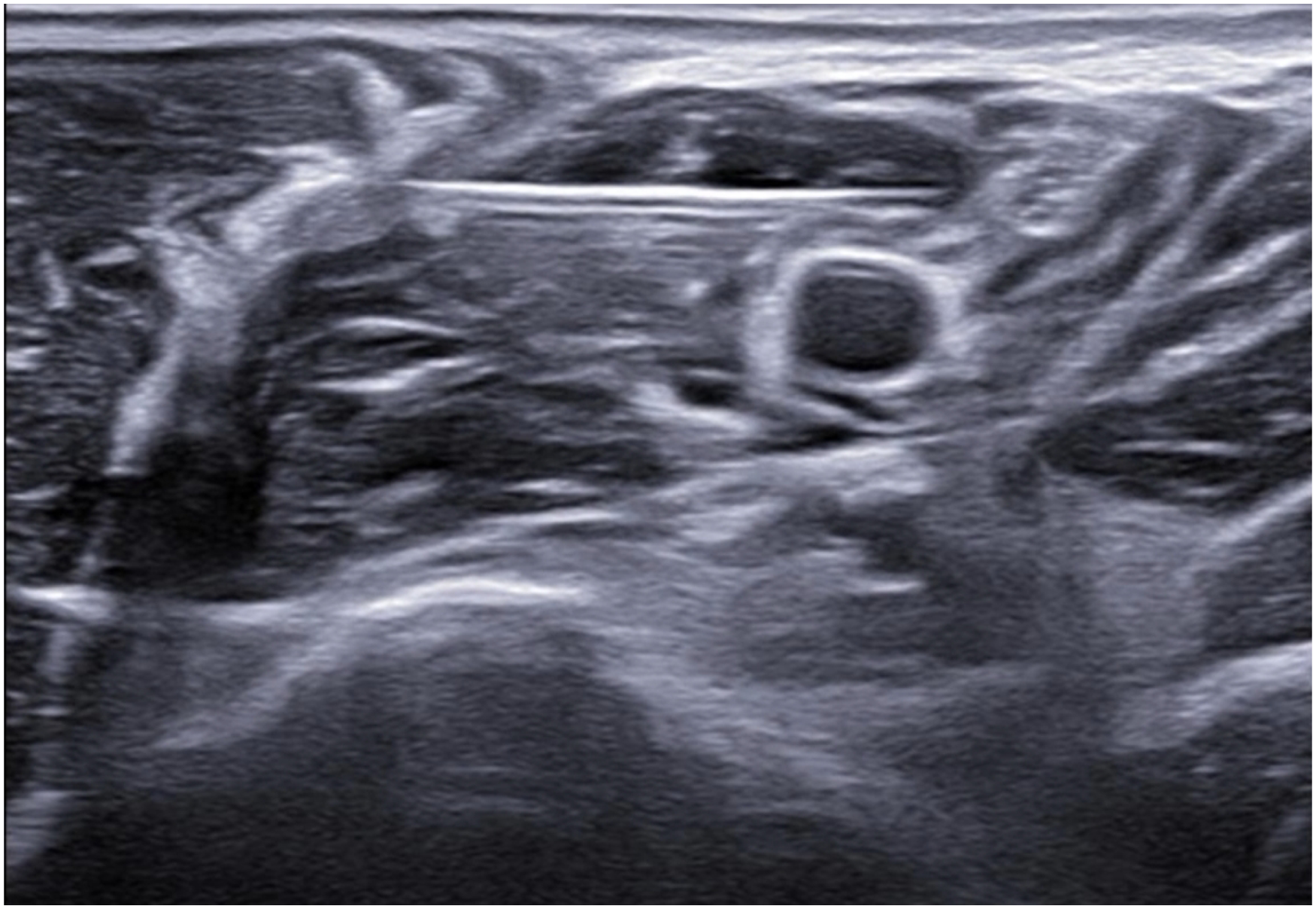
Ulnar nerve block.
Median nerve block.
Infiltration of anesthetic agent around median nerve.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.