
Abstract
Introduction
Management of orthopaedic fractures involves acute intervention and follow up through to recovery. Patient-centered care needs to encompass all aspects of this treatment. Limited research is available on outpatient satisfaction and patient-reported outcomes from fracture clinic (FRCL). The purpose of this evaluation is to report on pain levels perceived by patients from minor orthopaedic procedures that were necessary for the continued management of fracture care.
Methods
Patients were recruited in the FRCL if they were planned to undergo minor orthopaedic procedures. They were asked to report the pain they experienced at baseline, during the procedure, 20 min post-procedure, and 24 h following the procedure on a verbal numeric rating scale of 0–10. Healthcare professionals (HCP) were then asked to rank their perception of the severity of pain from each procedure type. Finally, qualitative interviews were conducted on a convenience sample of patients.
Results
51 patients were included in this evaluation. Halo pin, external fixation device, Kirschner wire, and screw removal exhibited a mean increase in pain from baseline greater than 3 units during the procedure. The external fixation device removal group showed the greatest pain reported with a statistically significant increase from baseline to the end of the procedure (mean = 7.1; p = 0.002). There was good concordance of pain perception by the HCP to patient experience. Qualitative interviewing revealed two major themes.
Discussion
This study provided valuable qualitative and quantitative insight into the pain perceptions by FRCL patients. This data may help improve the patient experience inside the FRCL.
Introduction
The fracture clinic (FRCL) is an outpatient hospital setting which serves as the continuum of care for patients with orthopaedic injuries. Patient-centered care should not only encompass the acute management, but the entirety of treatment as well, from injury to rehabilitation (2). Secondary procedures are often required which are performed in the FRCL. Many procedures done in this outpatient clinic involve the removal of medical devices placed during surgery. These procedures are performed by orthopaedic technicians, nurses, physician assistants or physicians and include Kirschner wire (k-wire) removal, external fixator (ex-fix) removal, casts, halo fixator removal, staple and suture removal.
Little information is currently available surrounding patient-perceived pain and experience in these outpatient settings. Two studies reported on pain levels of suture and staples removal found that patients reported higher pain levels in staple removal than in suture removal.1,2 A study by Ryder et al. reporting on ex-fix removal recorded an average pain of 3.6 (range 0.2–10) in 106 patients. 3 K-wire removal is a procedure in which much of the literature focuses on children and not adults.4,5 Overall, the literature reporting on patient reported outcomes (PROs) in a FRCL setting is quite limited. Although these procedures often induce pain, all were completed without the use of any anaesthetic and were deemed by the authors as “tolerable”.
Pain scores have also been shown to vary considerably between clinicians and patients performing the same assessment.6,7 In a study by Tay et al., clinician-reported outcomes (CRO) of pain and expectations of pain did not accurately reflect the pain experienced by patients for k-wire removal in children. 8 Nevertheless, the authors did not feel there was an indication for analgesia use. Incorporating PROs may improve the delivery of care to patients. 9 Other studies investigating ex-fix removal, suture, staple removal and others also have not routinely used analgesia.3,4,8,10,11
Based on the available literature, there is an evident knowledge gap of the patient experience and clinician perspectives on pain in the FRCL setting. There is a heterogeneity of procedures performed in the FRCL setting with variable degrees of invasiveness. There is also an opportunity to improve pain management in this environment.
It is common for there to be a variety of procedures that are done in the FRCL. These have varying degrees of invasiveness, may or may not include local anaesthetic, and can be done by a variety of health care personnel. This observational study aimed to evaluate the “real world experience” from common practice in the FRCL for patient-reported pain associated with several outpatient procedures. Additionally, this study aims to better understand the patient experience and clinician-perceived pain in the FRCL by conducting qualitative interviews with these patients and a survey with healthcare professionals (HCPs).
Material and methods
Patient population
Our institutional research ethics board granted approval to conduct this study. Patients were considered eligible for this study if they underwent one of the following outpatient procedures performed in the FRCL: ex-fix hardware pin removal, k-wire removal, staple removal, suture removal, cast and splint removal, bone fixation screw removal, removal or re-torquing of halo fixator pins and patients requiring casting or splinting. Patients were not eligible for this study if they were under the age of 18 or if they were receiving intravenous sedation during their procedure. A research assistant approached eligible patients in the FRCL after arrival to their appointment.
Data collection
Patients were enrolled in this prospective study from March 2021 to December 2021. Before the procedure, patients recorded any pain medication taken in the last 24 h. Patient demographic and treatment information such as age, gender, previous opioid use, and diagnosis were collected. Pain was recorded using a verbal numeric rating scale, a 0 to 10-point scale, with 0 being no pain and 10 being the worst imaginable pain (Figure 1). Pain scores were recorded at four different time points, baseline, during the procedure, and both 20 min and 24 h post-procedure. Patients’ highest pain score was recorded in 5 min intervals during the procedure and for 20 min post-procedure. Finally, 24 h after their procedure patients were asked to record their pain and any pain medication taken since their procedure via telephone.

Verbal numeric rating scale.
In patients who had two procedures done on the same day, one baseline score was collected. Separate scores for each procedure were then collected and compared to the one baseline score individually. To the best of our ability, questions were posed based on each procedure.
There was no standard post procedure analgesic regime for all procedures. Patients were given the option to take their normal oral analgesia that they have been taking previously. Local anaesthetic was used for two patients if a stab incision was required in the skin.
Qualitative interviews were also conducted. Using convenience sampling, several patients were invited to participate. Each interview was approximately 10 min in length and employed a qualitative approach outlined by Sandelowski. 12 A semi-structured interview guide was constructed to address specific aspects of the patient's experience with pain during minor procedures. The guide was constructed to begin with open, broader questions about the patients’ experiences leading up to being seen in the FRCL, followed by questions about each stage of their clinical process. Finally, a series of questions were asked concerning the patients’ preferences for pain management. All questions were designed to be exploratory and rely on probes to allow differences between patients’ perceptions and experiences to emerge during the interview. All interviews were recorded and transcribed verbatim for data analysis.
HCPs working in the FRCL were also asked to complete a short survey about their pain perception for these outpatient procedures. This survey asked HCPs to rank the eight procedures in order of least to most painful, as well as to estimate what they believe the average pain score would be for each procedure. Physicians, including residents and fellows, were emailed this survey, and nurses and technicians were given the survey in person.
Statistical analysis
To summarize patient demographics and treatment characteristics, mean (standard deviation; SD), median (inter-quartiles), range, or proportions were calculated for continuous or categorical variables. To compare the worst pain scores at each time point and the baseline pain score, the Wilcoxon Signed Rank test was performed. Two-sided p-value < 0.05 was considered statistically significant. To analyze the patient interviews, all transcriptions were read in their entirety multiple times to identify a coding framework. Then, the data were further analyzed for similarities and differences to reveal overarching or reoccurring themes. All analyses were conducted using R package (v4.2.1).
Results
Patient and treatment related factors
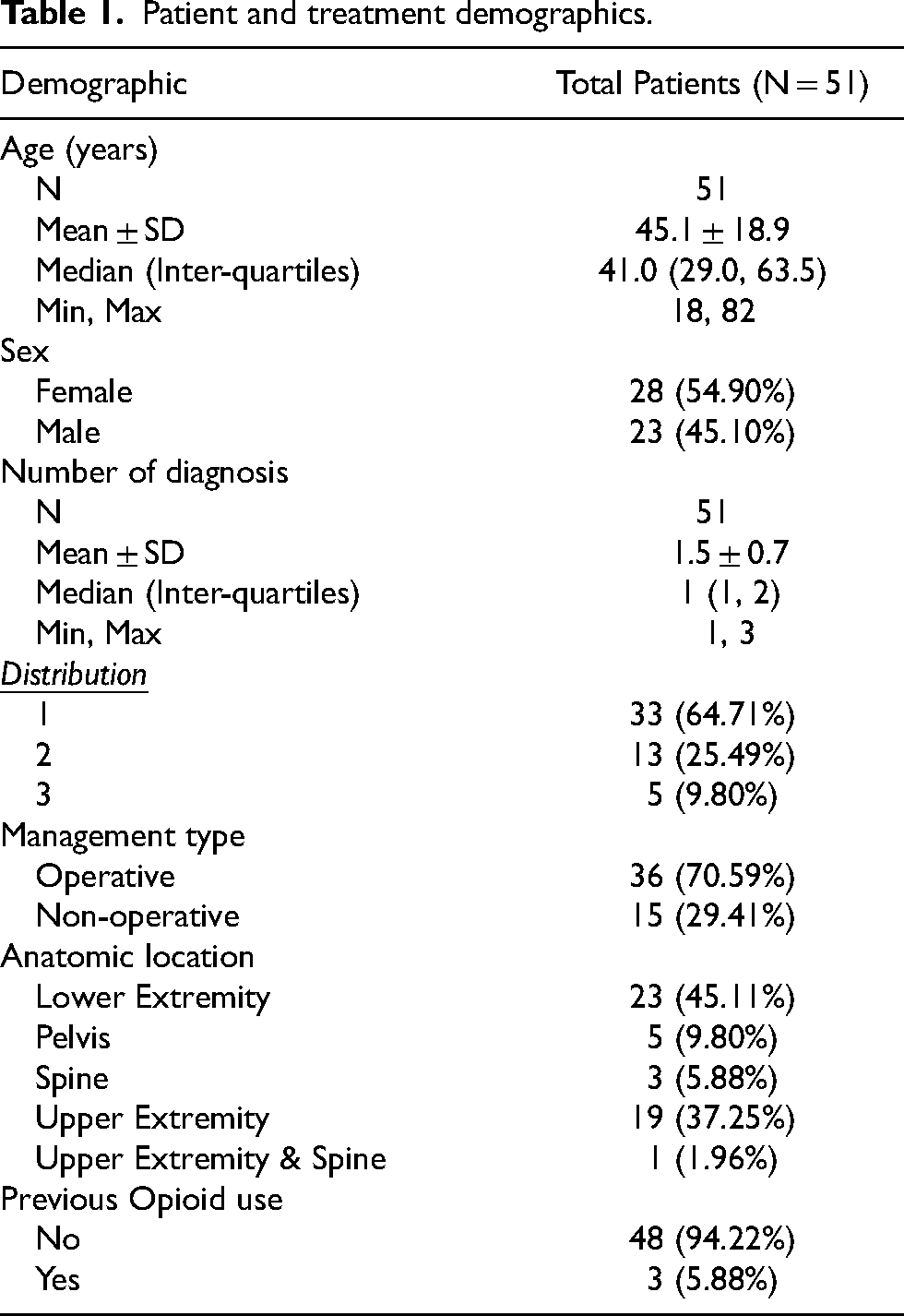
A total of 69 procedures in 51 patients were included for analysis. Some patients underwent two procedures that were evaluated as separate procedures. Patient and treatment characteristics are shown in Table 1. The median age of patients was 41 years (range: 18–82), 28 (54.9%) were male and 23 (45.1%) were female. Thirty three patients (64.71%) had only one diagnosis. The majority of patients, (n = 36; 70.59%), were treated operatively for their injuries. Injuries were most commonly in the lower extremity (n = 23; 45.11%). Most patients, (n = 48; 94.22%), reported no previous opioid use.
Patient and treatment demographics.
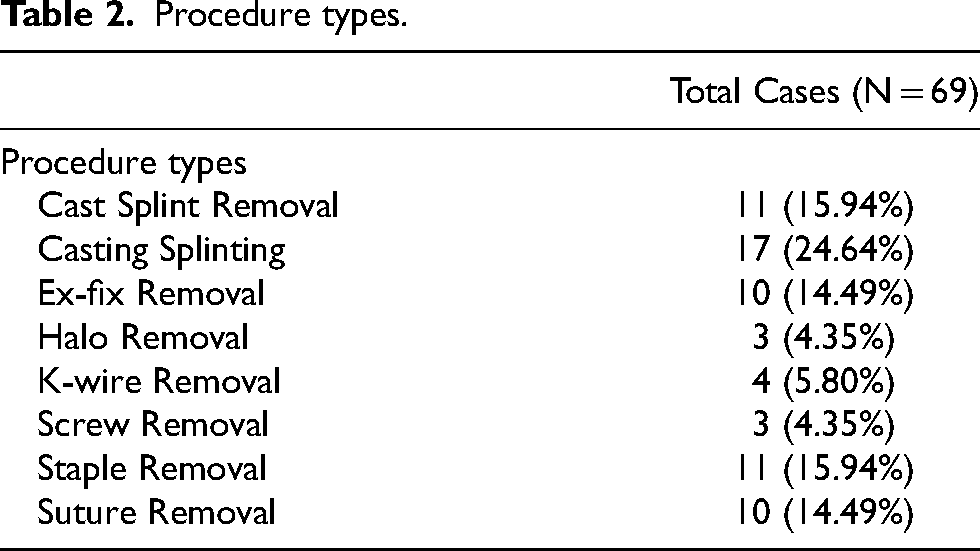
Eight procedure types were included in 69 cases. The procedure types and the number of cases in each procedure type are summarized in Table 2. Local anaesthetic was used in just two procedures. There was no regional anaesthesia used. Different HCPs performed different tasks; a nurse or cast technician removed staples or sutures, a cast technician removed or applied casts and removed percutaneous pins/external fixator or k-wires, a nurse removed halos and a surgeon removed buried screws where a stab incision was required with re-closure of the skin.
Procedure types.
Patient reported outcomes
Patients were asked to report any pain medication taken 24 h before their procedure (Table 3). The majority of patients had not taken any pain medication prior to halo removal, cast/splint removal, and k-wire removal. For the remaining procedures, most patients reported taking pain medication prior to the procedure. For suture removal, screw removal and staple removal, all patients reported taking pain medication before the procedure. Of the patients taking analgesics, acetaminophen was the most common (n = 20), followed by hydromorphone (n = 19).
Pain medication reported.
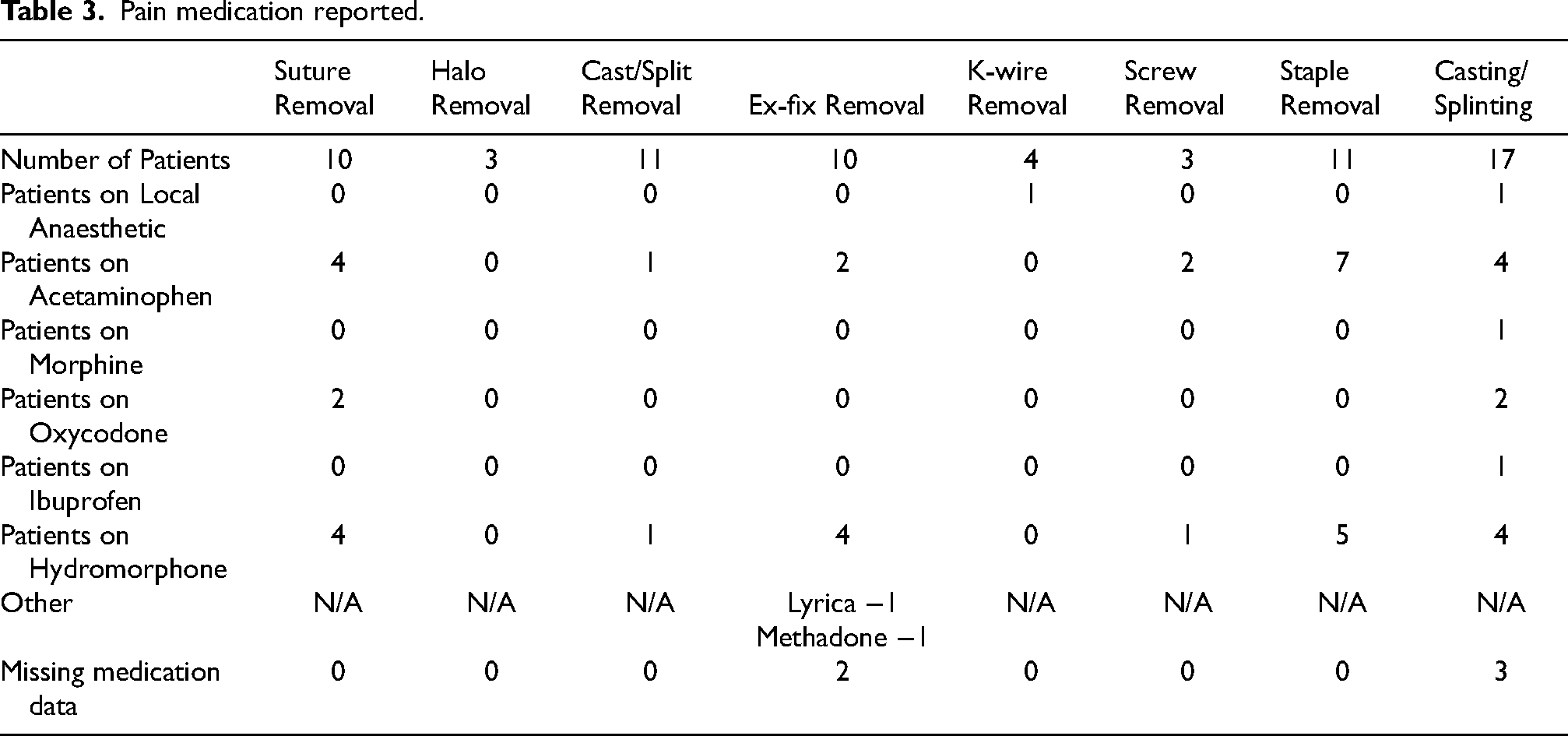
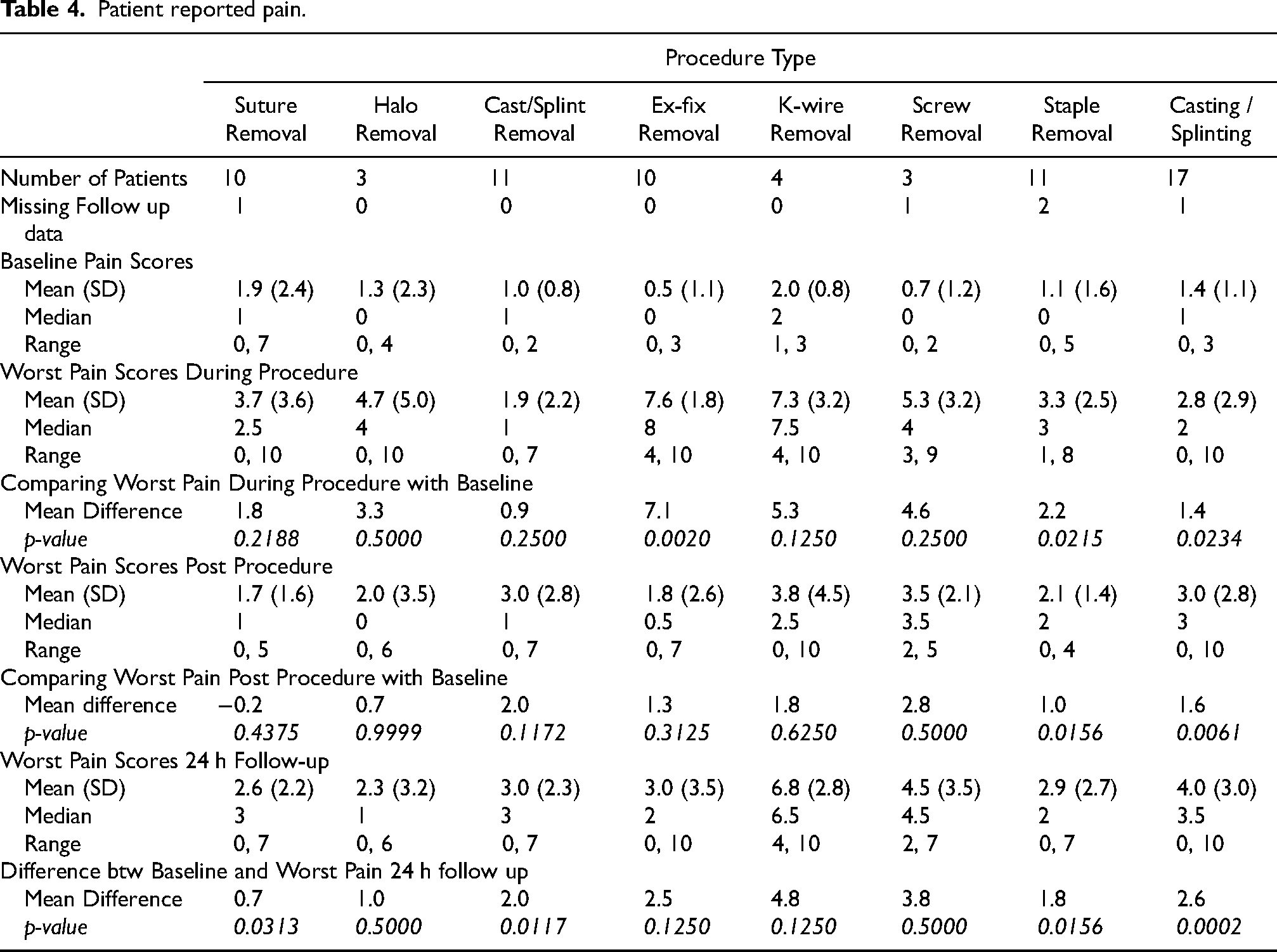
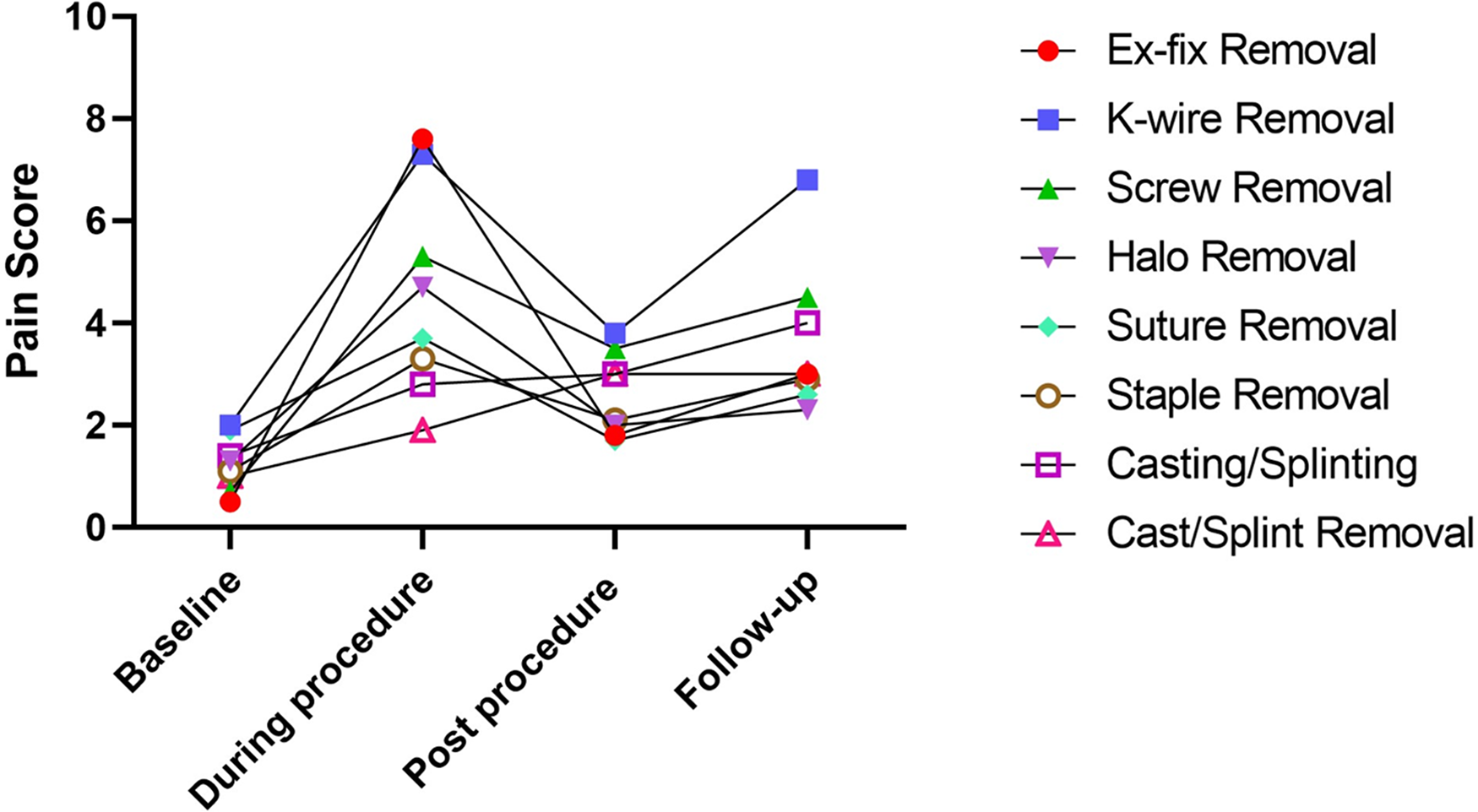
Table 4 and Figure 2 show the rankings and trends of pain scores at baseline, during the procedure, post-procedure, and 24 h following the procedure, along with the associated mean difference to baseline pain score. The baseline pain scores reported were low, with no group recording a mean pain score above 2.0. During the procedure, ex-fix removal, k-wire removal, and screw removal had the highest mean differences reported compared to mean baseline pain scores (7.1, p = 0.002; 5.3, p = 0.125; 4.6, p = 0.25; respectively). In the 20 min after the procedure, screw removal, cast/splint removal, and k-wire removal reported the highest mean differences for pain compared to baseline (2.8, p = 0.5; 2.0, p = 0.1172; 1.8, p = 0.625; respectively). The pain reported in the 20 min post-procedure was less than that reported during procedure for all except cast/split removal and casting/splinting. The procedures which reported the highest mean differences in patient-reported pain compared to baseline in the 24 h after the procedure were k-wire removal (4.8, p = 0.125), screw removal (3.8, p = 0.5) and casting/splinting (2.6, p = 0.0002). Halo, k-wire, and screw removal groups exhibited mean differences in pains scores greater than three without statistical significance (3.3, 5.3, 4.6; respectively) during the procedure compared to baseline.
Patient reported pain.
HCP survey
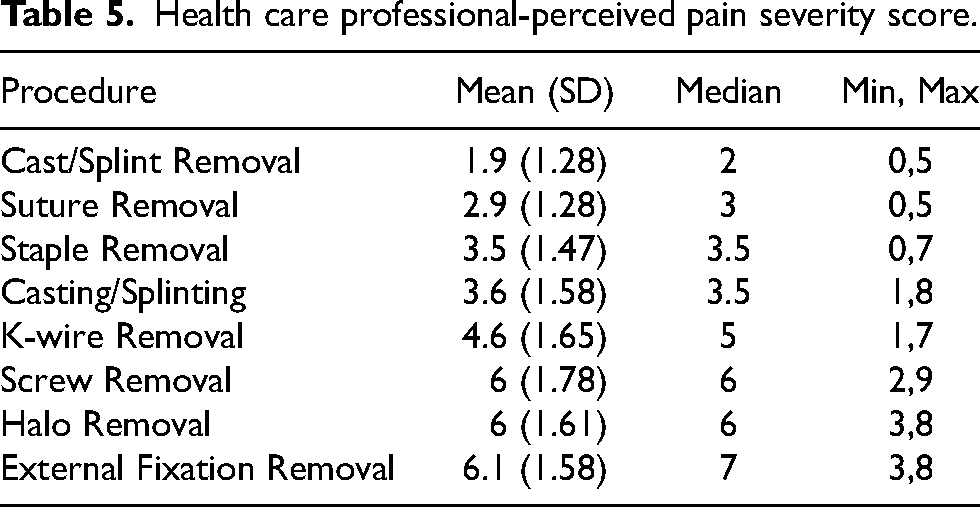
A total of 18 HCPs completed a short survey on their perception of pain associated with each outpatient procedure. They were first asked to rank the eight procedures from least to most painful (Figure 3). Halo removal, ex-fix removal, and screw removal ranked the most painful consistently among the HCPs. In comparison, ex-fix removal, k-wire removal, and screw removal had the highest mean differences reported compared to mean baseline pain scores for patients during the procedure. HCPs were then asked to provide an average worst pain score for each procedure (Table 5). Halo removal (mean = 6; SD = 1.61), screw removal (mean = 6; SD = 1.78), and external fixator removal (mean = 6.1; SD = 1.58) received the highest average worst pain scores from the HCPs. K-wire removal received an average pain score of 4.6 (SD = 1.65).
Trends in pain scores by procedure type.
Health care professional-perceived pain severity score.
Qualitative interviews
Eight qualitative interviews were conducted where patients were asked about their general experience with the FRCL before, during, and after their procedure. They were also asked for any recommendations that would have improved their experience. All procedures were discussed during the interviews except for screw removal. Two major themes emerged associated with the nature of patient experience.
Theme 1: negative patient experiences were associated with pain severity for select procedures
Two patients expressed explicit dissatisfaction and unpleasant emotions regarding their experience with the FRCL. In particular, the participants that underwent halo and k-wire removal expressed that the pain caused by their procedures was unbearable. In the following account, the patient described their procedural experience: “It was horrible. I have never felt so much pain in my whole life… I asked to be put under. They gave me a needle to freeze my foot but that was painful too… I was still screaming as they were trying to remove the rods… Nothing helped, one doctor was holding my leg down and other one was pulling the rods… I felt everything.” (Patient 2043, K-Wire Removal, Male)
Another patient who underwent k-wire and suture removal, although not expressing explicit dissatisfaction, spoke about the level of pain associated with their procedures: “It's like a double-edged sword, the best part of my experience was getting everything removed, but the worst part was that it was so painful. I was on pain medication, and they gave me this numbing cream, but they did not help much… I was still in a lot of pain.” (Patient 2041, K-Wire & Suture Removal, Female)
Theme 2: positive patient experiences were associated with perceived good quality of care
Irrespective of pain experienced, six of eight patients reported positive experiences associated with perceived high quality of care. Notably, despite varying levels of pain, patients expressed satisfaction with FRCL staff competency, efficiency, and friendliness.
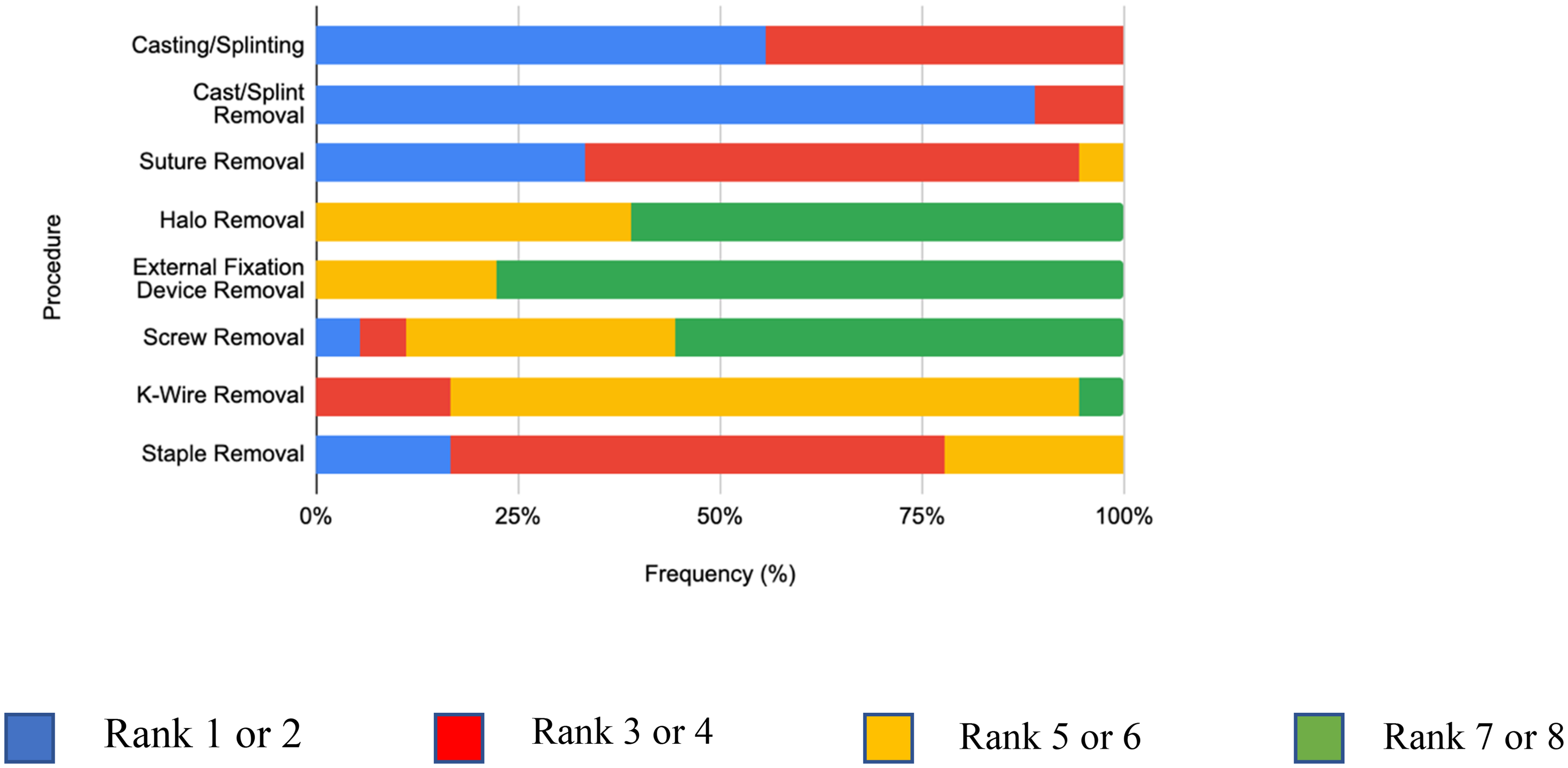
Health care professional-perceived pain severity ranking.
The last portion of the interview asked patients for recommendations that would have improved their experience. Four of eight patients had no recommendations (staple and suture removal, casting, and splinting), expressing satisfaction with their care and experience. One patient (k-wire removal) recommended that numbing the procedure area or another way to alleviate pain during the procedure would have improved their experience. Another patient, a second k-wire removal, expressed that being put under local anaesthesia was the only way the experience could have been improved. The patient that had a halo removed also expressed that finding a way to alleviate pain during the procedure would have improved their experience, but doubted that it was possible. All three patients described the pain during their procedures as the worst they ever experienced and were still dealing with residual pain and soreness post-visit. The last patient expressed that shorter wait times would have improved their experience (cast removal).
Discussion
The present study prospectively evaluated patient-reported pain in outpatient FRCL procedures. Since existing literature reporting the patient perspective is limited, this study demonstrates the real-world patient experience in the FRCL. Additionally, this study may be used as a historical control group for future studies to evaluate the effectiveness of alternative analgesics for use in the FRCL.
When comparing to the literature for staples versus suture removal, Shantz et al. noted staple removal being more painful than suture removal at two weeks (2.5 suture; 3.7 staple). In contrast, our results showed suture removal is more painful than staple removal (3.7 suture; 3.3 staple). Variability in the type of suture (i.e., mattress vs. simple) or the length of time the sutures are left in may account for the difference with the results of Shantz et al. 13
The literature available for k-wire removal is also limited. The few articles reporting pain associated with k-wire removal are in children.4,5,14,15 Our sample only included those 18 years of age and older, and many of these studies evaluate the child's level of pain using different tools which base pain on the child's reactions, facial expressions and presence or absence of crying. Alternatively, in children a surrogate (caregiver) was used for evaluating pain response.4,14
Two studies that reported pain associated with ex-fix removal were conducted by Pereira et al., and Ryder et al.3,10 Pain was reported with their removal in 29 and 106 patients, respectively.3,10 Using the visual analog scale and Numerical Pain Scale, the mean pain reported was 6.68 and 3.6, respectively.3,10 The mean pain reported during the procedure for our study was 7.6. Interestingly, these two studies concluded that removing ex-fix devices without anaesthesia is well tolerated by patients.3,10 This opinion of the authors is not our experience as “tolerated” is a very subjective assessment. Our assessment demonstrated that patients reported severe pain during the procedure despite eight of the ten patients taking some form of analgesia.
The other procedures we evaluated (halo removal, casting/splinting, screw removal and cast/splint removal), again have limited literature available on patient-reported pain. Much of the literature evaluated the efficacy of these procedures, but not pain associated with their removals.
There is a considerable gap in the literature regarding CROs and PROs for evaluating FRCL procedures completed in an outpatient setting. Few studies have compared PROs to CROs in the setting of the FRCL. One study on children undergoing k-wire removal evaluated the differences between clinician-perceived and patient-reported pain where it was found that clinicians underestimated the pain experienced by patients during this procedure. 8 Contrary to this previous study, our results show overall concordance between the patient's real time experience of pain and the HCP perceived pain. The three procedures rated as the most painful by HCPs (halo removal, ex-fix removal, and screw removal) each showed a mean increase in pain of greater than 3 points on the verbal numeric rating scale from baseline to during the procedure. Of note, all three patients that underwent halo removal and four of 10 patients in the ex-fix removal group did not report using pain medication for their procedures, suggesting a potential need for HCPs to provide improved analgesia in this group of patients.
High pain scores reported during these outpatient procedures are a potential concern and provides an opportunity to improve patient experience. The HCPs also understood how painful these procedures are. It is important to examine the current clinical practice for pain medication recommendations. Patients in this study were taking a variety of analgesics and still reporting high pain scores, especially in the screw removal, k-wire removal, and ex-fix removal groups.
The limitations for pain relief in the FRCL are well recognized. In the outpatient setting (typically a busy clinic), it is often not practical, and staff are not available to administer medication intravenously. Timing of taking oral medication is difficult to predict and side effects which can include sedation may preclude the patient from driving home.
The strengths of our study include its prospective nature, and the variety of procedures assessed. A further strength is the incorporation of both quantitative and qualitative measures which can best inform clinical practice moving forward. Within the existing practice of pain relief, the HCPs should improve communication with patients to better prepare them for the possible pain they may experience. Further research by evaluating other drugs which are non-sedative, quick acting and self-administered is indicated as we have shown there is an opportunity to improve patient outcomes in the FRCL setting.
A limitation of this study is the small sample sizes for the individual procedures and the heterogeneity of procedures. There are different degrees of invasiveness and with small sample sizes, direct comparisons are impossible. Notwithstanding this, the purpose of the study is to evaluate “real world experience” based on common practice in the FRCL. The purpose of evaluating pain perceptions of patients and HCPs using current protocols was achieved. The FRCL is expected to have a heterogeneity of procedures and a survey of these with the variability in pain was studied.
Another limitation that does not allow direct comparison between procedures is that different HCPs perform different tasks. This on one hand is a potential bias, but on the other hand may be best practice as having the fracture clinic nurse routinely do suture/staple removal and the halo nurse do halo removal, develops expertise. The cast technician is best at cast removal and the doctor is best at subcutaneous removal of screws. The study is an evaluation of “real world experience” based on current practice patterns. Another limitation was the data for pain medication taken by patients was not complete. This potentially could have been mitigated had the patients been enrolled in the study before arriving at the FRCL. Rather than having patients recall the dose or frequency of medication use upon arrival in the clinic, earlier enrollment could have enabled a detailed list of pain medication to be obtained.
Conclusion
The FRCL has a crucial role as part of the continuum of care for patients recovering from orthopaedic trauma. Despite the focus on patient-centered care, the literature is scarce concerning the patient experience inside the FRCL. This study provided valuable qualitative and quantitative insight into the perception of pain by FRCL patients. We have further shown that there is concordance in the perception of pain by HCPs to the experience of pain by the patient. Different procedure types in the FRCL vary in the pain they induce. We have provided a survey of real world experience in the FRCL of pain perceptions and regardless of what procedure is performed, there is pain and there is opportunity to improve on this (some procedures more than others depending on invasiveness) and ultimately improve patient experience.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Feldberg Chair in Spinal Research at Sunnybrook Health Sciences Centre.