
Abstract
Introduction
Coronavirus disease 2019 (COVID-19) has killed more than six million people worldwide. 1 Not only it is affecting people who were infected but also it is affecting people who require medical service but cannot attain it because of a shift in public health policy. The COVID-19 pandemic has caused a huge disruption in the medical service. Resources for specialties that were deemed relatively unessential were reduced significantly, in order to provide service for the infected patients. Sports surgery has been hugely impacted as the elective orthopaedic service has been reduced during the COVID-19 pandemic, and sports activities of the population have been minimised due to social distancing strategies. Sports surgery was reported to be one of the most affected subspecialties in the orthopaedics department during the COVID-19 pandemic. 2 Study has reported that there was a 34.6% reduction in sports-related injuries requiring emergency department visits in the USA in the year 2020 during the era of the COVID-19 pandemic. 3 There were 28.7% and 41.5% reductions in sports-related shoulder and knee injuries, respectively. 3 In the first two months of the COVID-19 pandemic, a more than 80% reduction in anterior cruciate ligament (ACL) reconstruction operation was recorded in the public hospitals in Hong Kong due to the relocation of hospital resources to combat the infection. 4
In this study, we aimed to quantify the change in the number of sports medicine operations during the COVID-19 pandemic, which could be useful for healthcare providers and policymakers in terms of resource planning in case of another severe infection outbreak in the future. Numerous guidelines for adjusting clinical service during a pandemic have been published; however, many were produced empirically at the early stage of the pandemic. This study aims to contribute data and information on the need for elective sports and arthroscopic surgery during times of pandemic and lockdown periods. In addition, it might provide insight into the impact of the pandemic on the incidence of sports-related injuries and degenerative conditions. Many of the studies in the current literature investigated the impact of the COVID-19 pandemic on the medical service and were based on data from a short early period of the pandemic when the disruption of the service was most drastic.2–6 Retrospectively, using more than two years of data during the COVID-19 pandemic and data from a comparative period before the pandemic, the primary outcome of this study was to quantify the change in surgical volume. We hypothesised that the COVID-19 pandemic had led to a decrease in the number of sports medicine operations performed in our local hospitals. The secondary outcomes included describing the types of operations before and during the COVID-19 pandemic, thus, looking for the change in demand for various types of sports surgery during the pandemic. The difference between the demographics of the patients before and during the COVID-19 pandemic was explored. Regarding the secondary outcomes, we hypothesised that the pandemic had led to a change in the case mix of the sports operations and the demographic of the patients presenting for sports operations.
Methods
The data of all the elective operations performed by the Division of Sports and Arthroscopic Surgery in Hong Kong West Cluster from 1st September 2017 to 30th June 2022 was retrieved retrospectively. This included all the operations performed in the two hospitals under the Hong Kong West Cluster – the Queen Mary Hospital and the Duchess of Kent Children's Hospital. The list of operations was retrieved from the operation record listing on the Clinical Management System of the hospitals by specifying elective operations performed by the Division of Sports and Arthroscopic Surgery. No cases were excluded from the analysis. The 29-month period from February 2020 to June 2022 was classified as the COVID-19 era. This is because the World Health Organisation declared its highest level of warning – public health emergency of international concern, to the infection caused by the SARS-CoV-2 virus on the 30th January 2020. 7 In addition, the Hong Kong government declared the highest emergency response level for the COVID-19 pandemic on the 25th January 2020, when a series of social distancing measures and a reduction of elective hospital service were implemented. 8 Data of all the operations in the preceding 29 months, from 1st September 2017 to 31st January 2020, was collected and classified as the pre-COVID-19 period for comparison. A total of 58 months of data was collected. The age at the operation and gender of the patients and the types of operation were recorded. The types of operations were classified into shoulder and knee surgeries. Shoulder operations included rotator cuff tear surgeries, reverse shoulder arthroplasty (RSA), shoulder instability surgeries and other shoulder surgeries. Other shoulder surgeries included arthroscopic capsular release, pectoralis major repair and removal of loose body. Knee operations included ACL operations, meniscal surgeries (repair or meniscectomy), operations for patellar dislocation and other knee surgeries. Anterior cruciate ligament operations were either ACL reconstruction or ACL repair. Other knee surgeries included diagnostic arthroscopy, loose body removal, implant removal, quadricep tendon repair, chondroplasty, PCL reconstruction, patellar tendon repair and wound debridement.
The numbers of various sports operations and the patient demographics of the COVID-19 and those of pre-COVID-19 cohorts were compared. Mann–Whitney U tests were applied to compare the monthly number of all operations, shoulder operations and knee operations before and during the COVID-19 pandemic. Chi-square tests were applied to compare the proportion of knee and shoulder operations and the gender of the operated patients before and during the pandemic. Unpaired t-tests were used to compare the age of the patients at operation between the two periods. Statistical analyses were conducted using SPSS (version 27.0, IBM, Armonk, New York, USA).
Results
A total of 523 operations were performed by the Division of Sports and Arthroscopic Surgery in the two hospitals of HKWC in the study period of 58 months. There were 292 operations performed during the 29 months of the pre-COVID-19 period, while there were 231 operations during the 29 months of the COVID period. The number of operations performed per month was reviewed (Figure 1). There was a significant reduction in the number of sports surgeries performed per month. The mean number of sports surgeries performed after the beginning of the COVID-19 pandemic reduced by 20.9%, from 10.1 (SD = 4.0) to 8.0 (SD = 3.8) operations per month (p = 0.042) (Figure 2; Table 1).
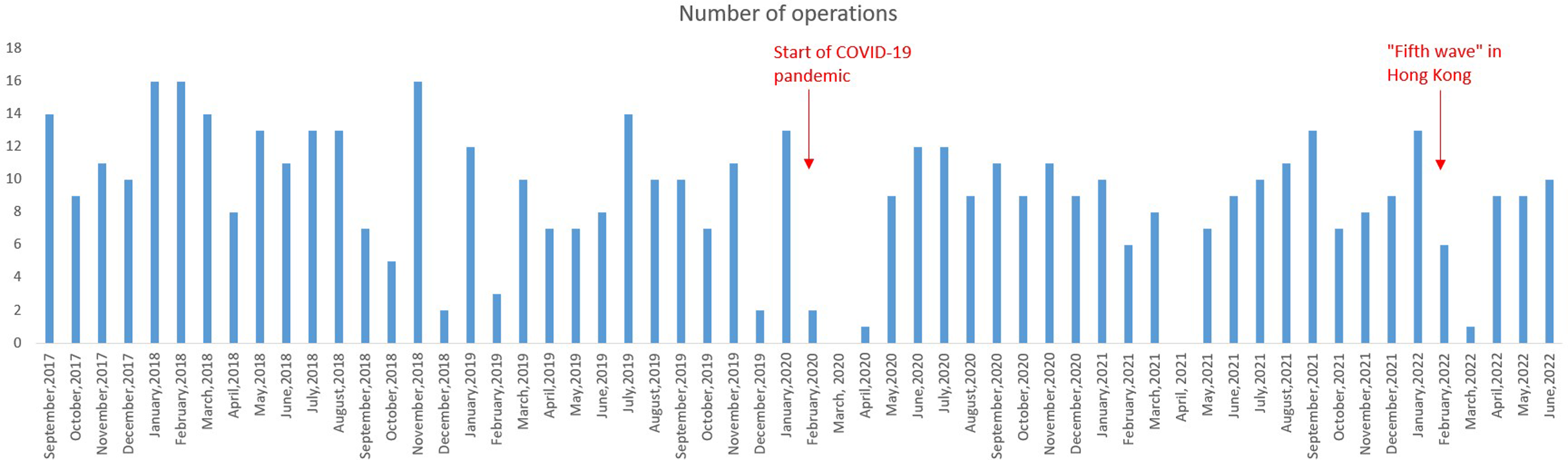
Bar chart demonstrating the number of operations performed in each month from September 2017 to June 2022.
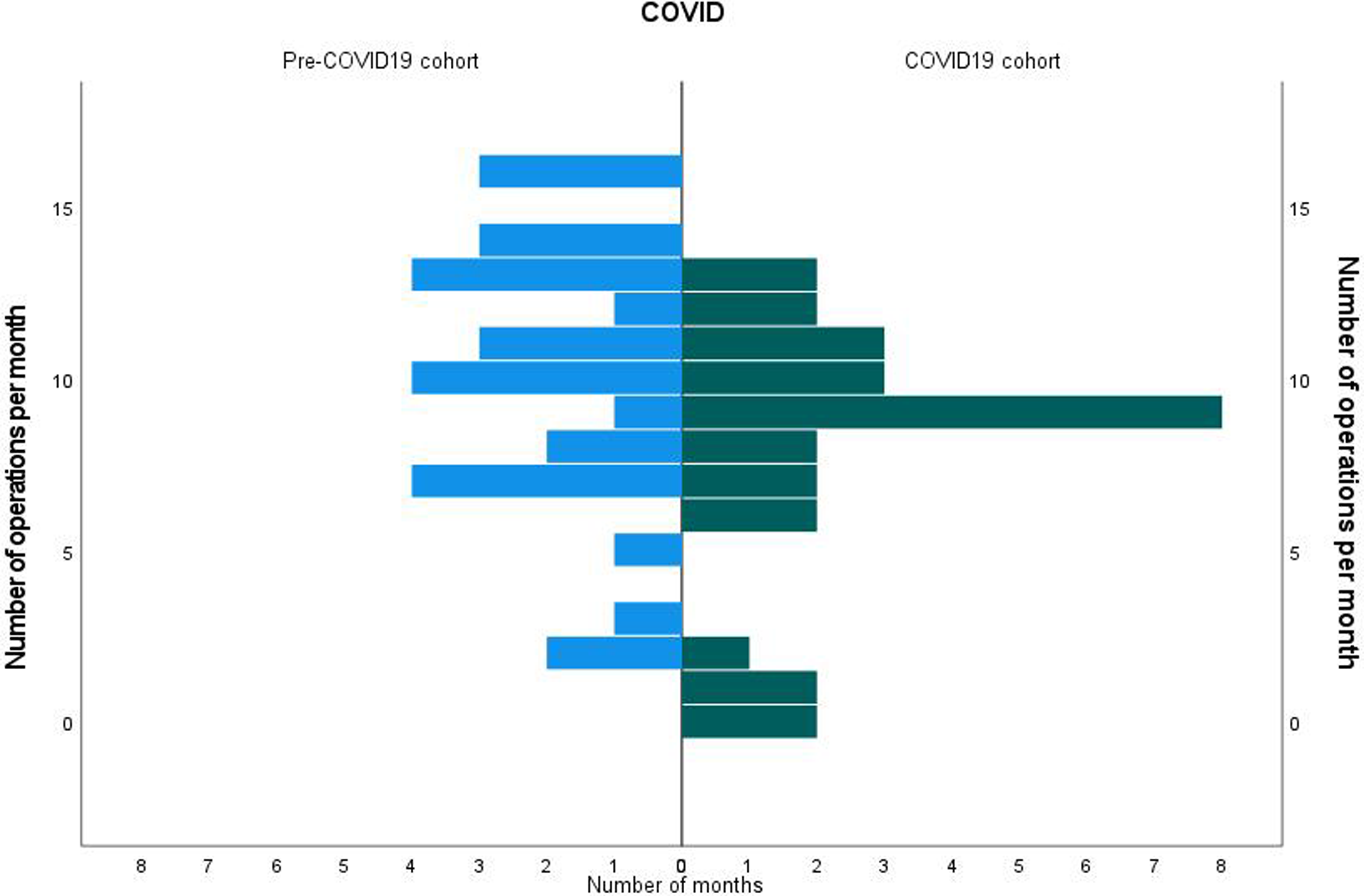
Histograms comparing the number of operations performed per month before and during COVID-19 pandemic.
Mean number of operations per month before and during the COVID-19 pandemic and their changes and the p values.
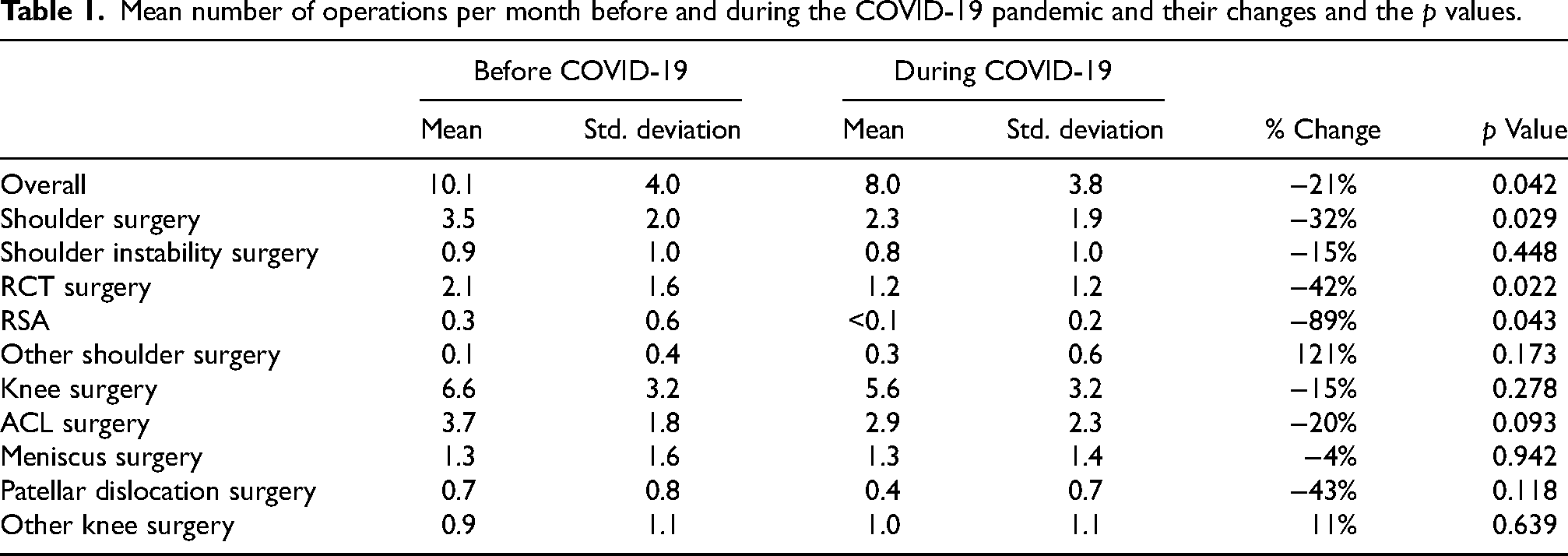
The mean number of shoulder operations per month was significantly reduced from 3.5 (SD = 2.0) before COVID-19 to 2.3 (SD = 1.9) during the COVID-19 pandemic (p = 0.029) (Table 1). When the numbers of each specific type of shoulder operation were investigated, the mean monthly number of rotator cuff tear surgery and RSA were reduced by 41.6% (p = 0.022) and 89.3% (p = 0.043), respectively. Although statistically insignificant, the number of shoulder instability surgery was reduced by 15%.
There was a reduction in the number of knee operations performed during the COVID-19 pandemic; however, the reduction was not statistically significant. The mean number of knee operations per month was reduced from 6.6 (SD = 3.2) before COVID-19 to 5.6 (SD = 3.2) during the COVID-19 pandemic (p = 0.278) (Table 1). The numbers of ACL surgery, meniscal surgery and patellar dislocation surgery were reduced by 20%, 4% and 43%, respectively, during the COVID-19 pandemic; however, none of the changes were statistically significant.
The relative proportion of knee and shoulder operations remained similar during the COVID-19 pandemic. Before the COVID-19 pandemic, 66% of all operations were knee surgery and 34% were shoulder surgery, while during the pandemic, 71% were knee surgery and 29% were shoulder surgery. No significant difference was identified between the relative proportion of knee and shoulder surgeries before and during the pandemic.
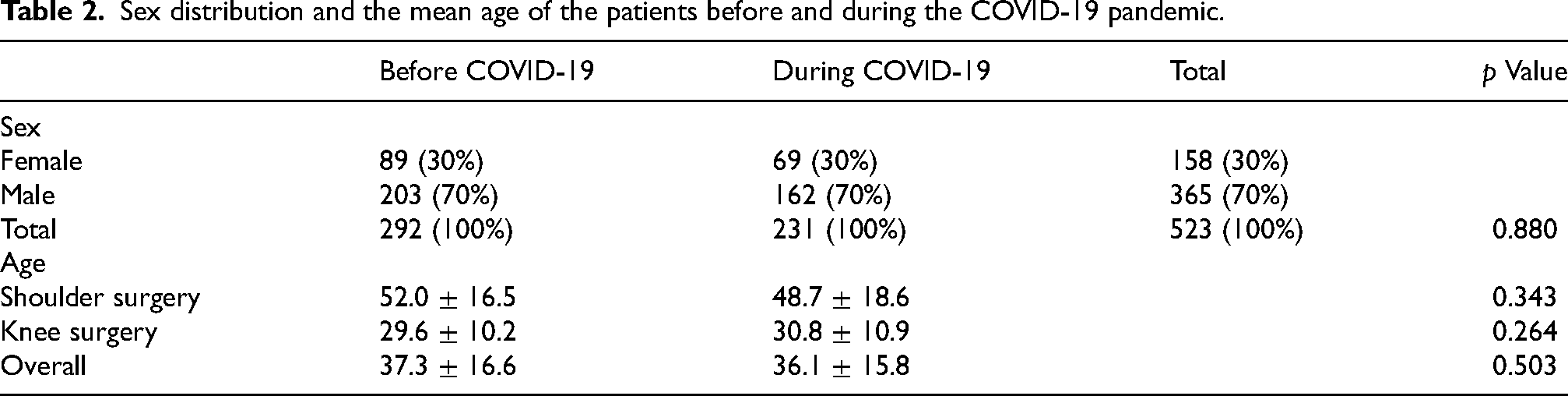
In terms of the demographic of the patients whom we have operated on, the gender distribution was the same before and during the pandemic, with a male-to-female ratio of 7:3 (Table 2). The majority of our patients were men both before and during the COVID-19 pandemic. There was no significant difference between the mean age of patients who underwent surgery before the pandemic and those during the pandemic. The mean ages of all operated patients before and during the pandemic were 37.3 (SD = 16.6) and 36.1 (SD = 15.8) years old, respectively (Table 2). The mean ages of shoulder patients were 52.0 (SD = 16.5) and 48.7 (SD = 18.6) before and during the pandemic, respectively. The mean ages of knee patients were 29.6 (SD = 10.2) and 30.8 (SD = 10.9) before and during the pandemic, respectively.
Sex distribution and the mean age of the patients before and during the COVID-19 pandemic.
Discussion
This study evaluated the impact of the COVID-19 pandemic and public health policy related to infection in Hong Kong on the surgical volume of sports and arthroscopy surgery in the local hospitals. There was a 21% reduction in the overall surgical volume in the two hospitals during the pandemic when compared to the pre-COVID-19 period. This finding supported our hypothesis of the primary outcome in which the pandemic had led to a decrease in the number of sports operations performed in our hospitals. A study that investigated the impact of the pandemic on a German level I trauma centre from March 2020 to May 2020 revealed a reduction of approximately 20% in the total operation number and an 85% reduction in elective operation during the lockdown period. 6 A UK study reviewing the situation in the first month of implementation of social distancing measures reported an 89% reduction in the referrals for sports injuries and about a one-third reduction in the acute operation number in a trauma centre in London. 5 They attributed the reduction in surgical volume to the decreased referral volume. 5 The relatively smaller reduction in the overall number of operations in this study might be explained by the longer study period that included periods when the local infection situation damped down and the resumption of some elective hospital services.
The lockdown during the pandemic did not only reduce sports-related injuries but also degenerative conditions such as rotator cuff tear. The number of shoulder operations in this study significantly reduced by 32% with rotator cuff surgery and RSA reduced by 42% and 89%, respectively. This finding was comparable to a study that involved surveying surgeons of the Turkish Society of Shoulder and Elbow Surgery in the early period of the pandemic, which reported that more than 90% of the participants discontinued elective surgery and more than 75% reduction in their clinic and surgical activity. 9 Majority of our shoulder patients composed of middle-aged to elderly patients with degenerative rotator cuff tear. As of the writing of this manuscript, no research articles have been published that investigate the incidence of rotator cuff tears during the COVID-19 pandemic or periods of social isolation. The reduction in the surgical volume for rotator cuff pathology in this study might be explained by the reduction in manual labour during the lockdown period as the Hong Kong government implemented a special work arrangement for citizens to work from home. 10 A recent study has demonstrated that high-intensity work level with heavy manual labour is associated with the progression of partial thickness rotator cuff tear. 11 Thus, the overall reduced manual labour activity in the community during the pandemic might have contributed to the reduction of the incidence of rotator cuff tear that required operative management. Another proposed possible reason was that middle-aged and elderly patients were reluctant to risk infection exposure by attending clinics and hospitals. A study reported that 61% of the general public participant expressed concern about getting a COVID-19 infection while hospitalised for a surgical procedure, particularly in the waiting and admission areas and also in situations where they require excessive interaction with the healthcare staff. 12 They also showed that women and non-native English speakers were more reluctant to undergo elective operations during the pandemic in the United States. 12 A proportion of the rotator cuff injury could be managed conservatively with home exercises; hence, patient might have preferred a trial of conservative management before considering admission for operation during the pandemic.
On the other hand, knee operation did not show a significant reduction in this study, with a 15% reduction in the total knee surgical volume. As anticipated, ACL surgery was reduced by 20% during the pandemic; however, it was not statistically significant. This could be explained by the reduction in the overall activity of organised team sports such as football and basketball during the lockdown period when team sports were banned and sports facilities were closed as ordered by the government. According to a study based on the local data in the first two months of the COVID-19 pandemic in Hong Kong, there was a significant reduction of approximately 60% in the number of sports-related injuries. 4 A study evaluating the effect of the pandemic on sports-related injuries presented to the emergency department in the three-month lockdown period in the USA reported that there was more than a 90% drop in emergency department visits due to organised team sports-related injuries. 3
Despite the reduction in ACL surgeries, the number of meniscal surgeries remained largely constant during the pandemic, with only a 4% drop in the number. Although there has not been any report of the incidence of meniscus injury during the pandemic in the literature, the finding aligned with that of a study investigating the surgical volume for sports medicine fellows during the early stages of the pandemic. 13 They reported that there was a significant reduction in procedures for multiligamentous knee injuries in the first year of the pandemic; however, it showed a rebound rise in the number of procedures for knee cartilage and meniscal conditions in the second year of the pandemic. 13 Risk factors for meniscal injuries include obesity, male sex, pivoting and contact sports and repetitive squatting or kneeling. 14 It had been documented that injuries related to deconditioning rebound after a period of suspension of sports activity. 3 Amateur and professional athletes were likely deconditioned during prolonged periods of inactivity and the misjudgement of readiness to return to play might have predisposed them to injuries. Congestion of games in between lockdown periods could also increase the risk of injury, as demonstrated by a study with 11 years of follow-up investigating the impact of fixture congestion on the injuries of professional competitive footballers. 15 Injury prevention and gradual resumption of training are recommended to avoid injury when athletes returned to play. 16 Another possible reason to explain the relatively high demand for meniscal surgery was that more individuals were participating in ‘COVID-19-safe’ individual sports such as hiking, running and cycling, as team sports were suspended. In addition, because of the closure of the gym and many entertainment venues in the community due to the social distancing measure, there was a trend for untrained individuals to take up these outdoor individual sports, hence a higher risk of injury. This was supported by a study that reported a surge of cycling-related injuries during the lockdown period. 17 However, based on the available data in this study, it is not possible to draw a conclusive explanation for why the need for meniscal surgeries remained constant during the pandemic.
The results of this study did not support our hypothesis regarding the secondary outcomes, in which we hypothesised that the pandemic had led to a change in the case mix of the operations and the demographic of our patients. There was no significant difference in the proportion of knee and shoulder operations between the pre-pandemic period and during the pandemic. In addition, there was no significant difference in terms of the mean age and the male-to-female ratio of the patients presenting for operation between the two comparing periods.
Although the findings of this study cannot conclude whether the reduction in surgical volume was due to resource limitations or a true reduction of the incidence of these injuries, the authors believe that it was likely due to a decreased incidence of such injuries. Despite the significant reduction in the surgical volume in our centre during the pandemic, we did not observe any accumulation of cases on the waiting list for these procedures. The threshold to offer operation in our division was unchanged during the pandemic and there was not much backlog of operations waiting at the end of the study period. Patients newly referred to our division could have operation arranged in one to two months, which was similar to that before the pandemic. Thus, the reduction in the surgical volume was likely attributed to a decrease in the incidence of injuries rather than solely a result of resource limitations. A study reported that there were around 30–50% reductions in the searches for ‘ACL’, ‘meniscus’ and ‘rotator cuff’ on Google by the general public, while the search for ‘ACL surgery’, ‘meniscus surgery’ and ‘rotator cuff surgery’ decreased by around 40–60%. 18 They suggested that the decline in public interest surrounding these topics could be due to a decreased incidence of these injuries. 18 For these reasons and given the relatively long follow-up for this study, the reductions in the number of procedures found in this study might provide an insight into the incidence of the injuries that necessitate operations during the pandemic.
By looking at the trend of the number of procedures per month from September 2017 to June 2022 (Figure 1), the two most significant disruptions of service occur in early 2020 and early 2022. January 2020 marked the beginning of the COVID-19 pandemic and the implementation of a social distancing policy in Hong Kong. There was a 50–100% reduction in the elective operation service from February to April 2020. The ‘Fifth wave’ of COVID-19 hits Hong Kong in January 2022 causing severe disruption of the public health system of the city with reported daily cases of infection more than fifty-thousand. 19 In April 2021, because of the manpower issue in our division, there was no operation performed in that month and it was not related to the pandemic situation.
Based on this study's results, it may be reasonable to limit elective operation sessions for sports and arthroscopic surgery during the COVID-19 pandemic when resources are scarce, as the need for these surgeries appears to be reduced during the lockdown period. A guideline published during the pandemic also recommended conservative management over early surgical intervention for patellar dislocation and knee ligament injuries to optimise the use of the limited medical resources. 20 In response to the decreased demand for elective orthopaedic procedures and the increased need for managing COVID-19 infections, a guideline suggested that surgeons should take on non-surgical roles to assist in the care of COVID-19 patients when the surgical workforce has been maintained. 21 Reducing the number of elective surgeries also helps to minimise the risk of COVID-19 transmission while ensuring that patients with urgent or emergent conditions can still receive the care they need. Moreover, alternative measures such as non-surgical interventions and home-based rehabilitation can be utilised to minimise the need for surgical interventions and reduce the number of patients in hospitals. By implementing these strategies, healthcare providers can maintain the quality of orthopaedic care for sports injury patients while also ensuring their safety during the pandemic.
The main limitation of this study is that the findings were based on data from only two public hospitals in Hong Kong. This might not truly reflect the local situation in other centres. The number of operations per month could be affected by multiple factors, apart from the pandemic situation. One of the reasons was the suspension of operating theatre due to the annual maintenance in December before the COVID-19 pandemic; hence, the relatively lower numbers of operations. Other limitations were that this study did not include the patients on the waiting list and did not investigate the onset or the time of the presenting injuries. Some of the patients who had operations performed during the pandemic period might sustain their injuries before the start of the pandemic, thus, a conclusion cannot be made regarding the incidence of injuries during the pandemic. Further analysis of the new attendance of sports-related injuries to the emergency department or our clinic would give more information on the true incidence of these injuries during the pandemic. This study could not address the cause of the change in surgical volume, which could be multifactorial. The reduction of the surgical volume during the pandemic might not only be due to the reduction of the incidence of sports medicine-related conditions but also the reduction of the public hospital service.
Conclusion
The total surgical volumes were significantly reduced by 21% when compared to the pre-COVID-19 period, while the case mix of the operation and the demographic of the patients who underwent operations remained similar during the pandemic. The number of ACL surgery and rotator cuff surgery were reduced by 20% and 42%, respectively, during the pandemic. These could be related to the reduced sports activity and manual labour activity during the lockdown periods of the pandemic. However, further studies with analysis of the presentation of new cases to the emergency department or clinic are warranted to draw conclusions regarding the incidence of these injuries during the pandemic. Despite these limitations, this study provides information and insight into the demand for sports medicine-related operations during periods of severe infection outbreaks. Considering these findings, it may be practical to limit elective operation sessions for sports and arthroscopic surgery during the pandemic, especially when resources are scarce. However, it is essential to strike a good balance between providing necessary care for patients who require these surgeries, while also taking appropriate measures to combat the pandemic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
IRB reference number: UW 23-125.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.