
Abstract
Purposes
This study aim to describe surgical outcome in treating postoperative radial neck nonunion and to perform a systematic review to evaluate the surgical outcome of symptomatic radial neck nonunion.
Methods
The study included ten patients with symptomatic postoperative radial neck nonunion from 2010 to 2016 which were treated surgically with either bone grafting (bone-grafting group) or radial head resection (resection group). The patient demographics, pre- and postoperative clinical scores were recorded. The PubMed, OVID/Medline, Cochrane, Google Scholar, and EMBASE databases were searched using the keywords “radial neck nonunion” according to the MeSH index. A systematic review was performed using PRISMA guidelines.
Results
Average time from primary surgery to nonunion was 10.7 months. Four and six patients received bone-grafting and radial head resection procedure. The mean age for resection group is older than bone grafting group (59 versus 28.75 years). The resection group patients presented with more significant pre-operative symptoms, associated injuries, loss of radial head articular congruity, and bone loss. All patients achieved favorable outcome. The systematic review included 12 publications with a total of 19 patients. The incidence of radial neck nonunion was 73.7% and 26.3% following conservative and operative treatment respectively. About 42.1% received operative treatment due to symptomatic progression.
Conclusions
Radial neck nonunion is rare and mostly appears asymptomatic. Operative treatment is advocated for symptomatic cases. Articular congruity and degree of bone loss are major determinant for surgical treatment of radial neck nonunion. Surgical treatment for symptomatic radial neck nonunion resulted in favorable outcome.
Introduction
Radial neck nonunion is uncommon in adults,1–6 due to their relative low incidence of the fractures. Nonunion is a result of both systemic (smoking, diabetes, non-steroid anti-inflammatory drugs abuse, alcohol abuse, and nutritional deficiency) and local factors (degree of fracture comminution, poor cortical apposition, interposed soft tissues, soft-tissue damage, bone loss, infection and quality of surgical treatment). 7 Minimally displaced fractures of the radial head and neck generally show favorable clinical outcomes, regardless of treatment method. 8 However, healing impairment may result from the insult of the time of injury to the precarious blood supply to the radial head and neck especially in those with associated injury.9,10 In the setting of radial head and neck fracture, surgeons will attempt their best effort to restore elbow biomechanics by performing internal fixation which generally follow by early mobilization to prevent stiffness.9,10 Still, those efforts may lead to inevitable loss of fracture reduction and fixation failure.9,11
Because of the small number of patients assessed, to date, the treatment of symptomatic radial neck nonunion remains unclear.1–6,11–14 Disturbed healing despite non-operative treatment has not been widely described.1,5 Radial neck nonunion following surgical intervention is even more infrequent.6,11 The aim of the current study is to describe patients which underwent surgical treatment following symptomatic post-operative radial neck nonunion. Systematic review following PRISMA guideline was performed to provide the current evidence of the clinical outcome of treating radial neck nonunion. To our knowledge, this is the largest case series of symptomatic post-operative radial neck nonunion reported.
Materials and methods
Case presentations
Ten patients (five women and five men) were diagnosed with symptomatic radial neck nonunion at an average of 10.7 months (range, 9–13 months) following surgery from the year of 2001 to 2016. All patients underwent primary surgical treatment within the average of 2.1 days (range, 1–4 days) after injury. The average age was 46.9 years (range, 17–76 years). Dominant extremity was involved in four patients. Causes of injury included falling onto an outstretched hand and motor vehicle accident. The type of fracture presented with Mason type III and IV. Five patients had associated injuries at the initial trauma.
Nonunion of the radial neck was diagnosed by plain radiography and computed tomography scan (CT). After symptomatic nonunion was confirmed, the surgical treatment was planned for all patients as shown in Figure 1. All secondary surgeries were performed by single senior elbow surgeon (I.H.J). Kocher approach was used in all patients for surgical approach. When nonunion was diagnosed, the articular congruity of the radial head and the degree of bone loss were measured as the primary dependent factor for surgical decision making. The pre-operative loss of range of motion (ROM) and the presence associated with injuries will be secondary dependent factor for surgical decision making. There were four patients without bone loss and preserved articular surface on the radial head. These patients underwent autologous iliac bone grafting (bone grafting group) (Figure 2). The other underwent radial head resection (resection group) due to bone loss and damage to the articular joint congruity. Pre- and postoperative Mayo Elbow Performance Index (MEPI) and ROM were assessed. All patients were followed up radiographically (Figures 3 and 4). Radiological union was documented for the bone grafting group. The final follow up time was 17.9 months after the secondary surgery.
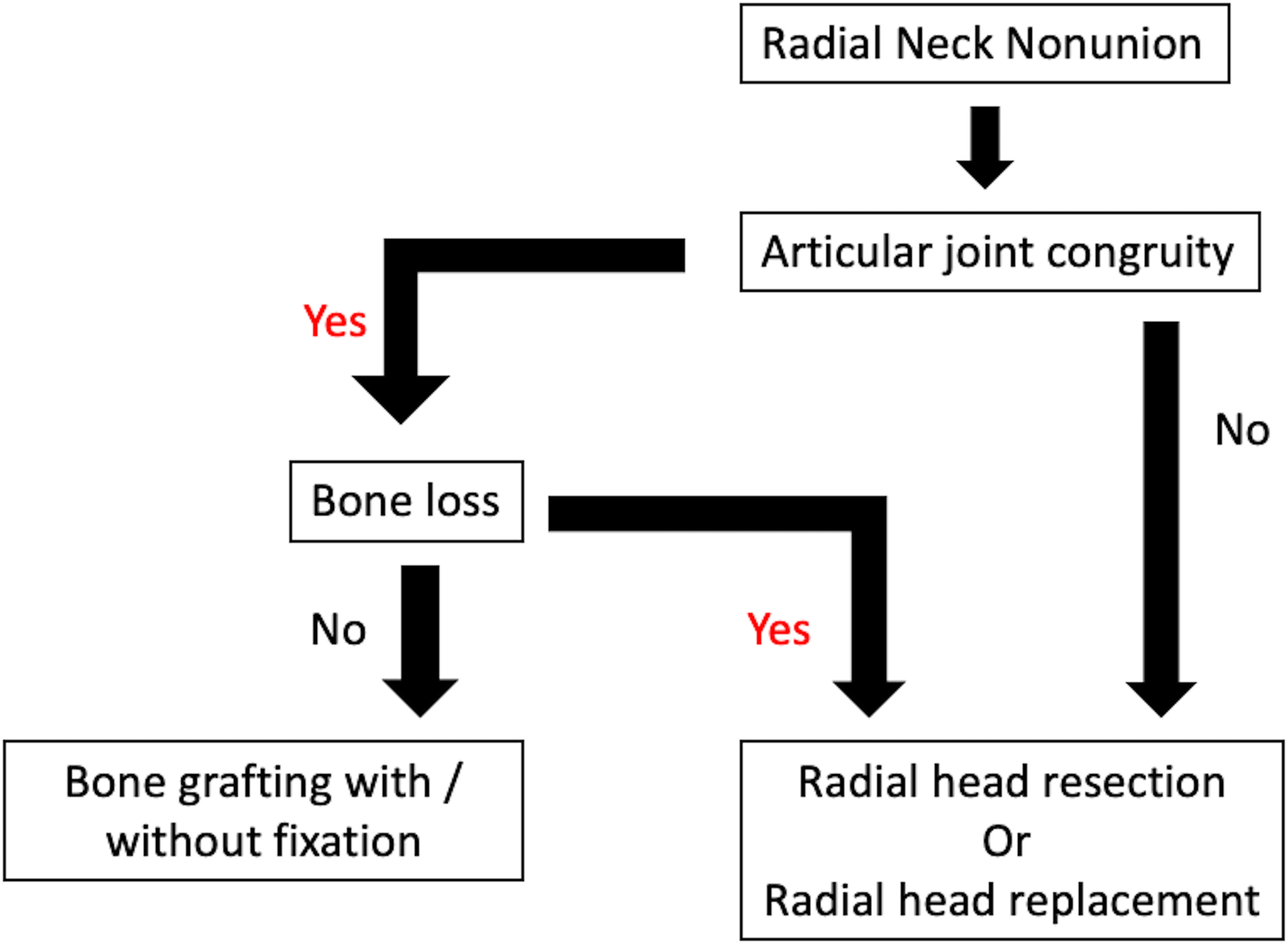
Treatment plan for radial neck nonunion.
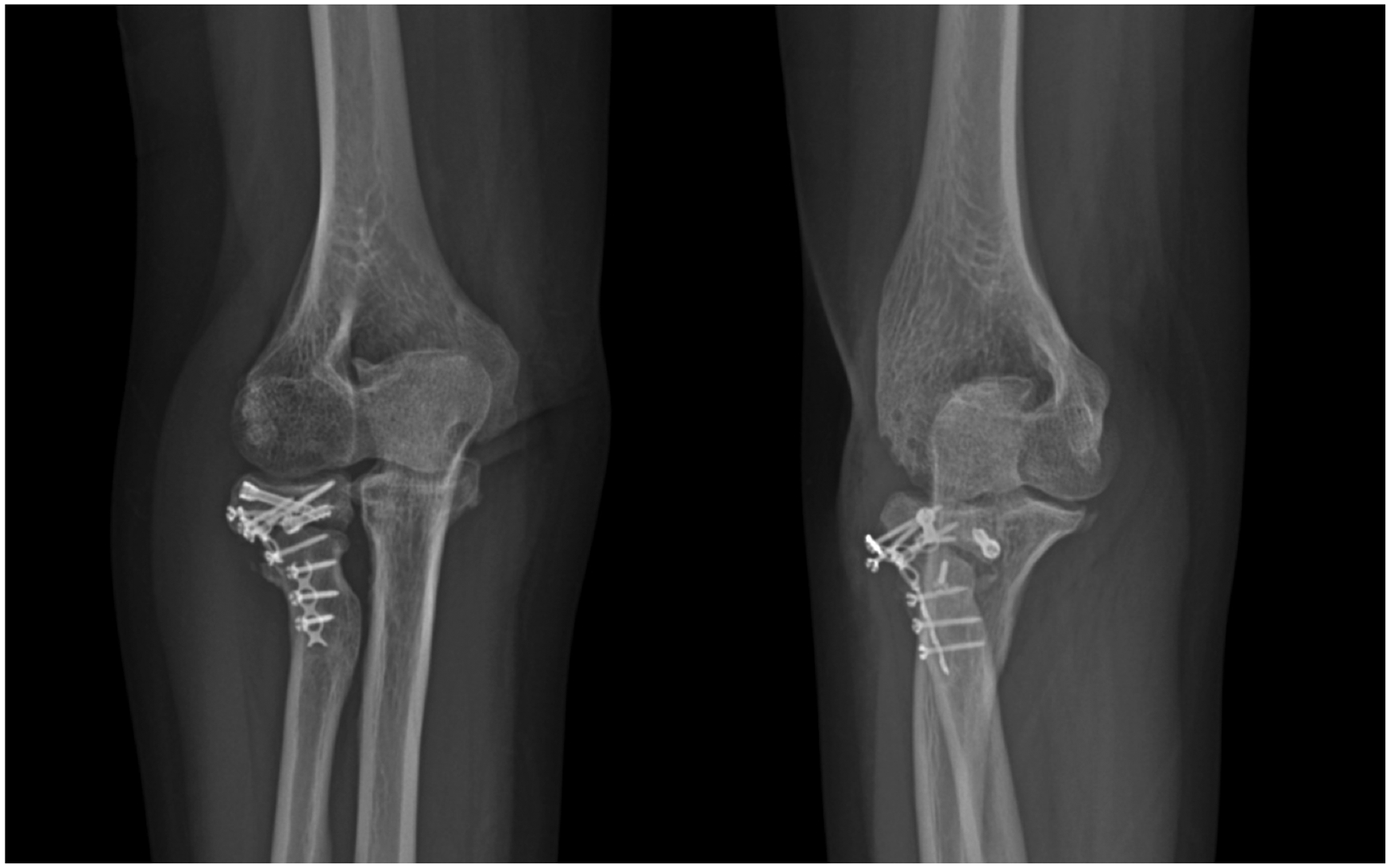
Radiographic figures of post-operative nonunion of the radial neck reveal a congruent radiocapitellar joint with no bone loss.

Radiographic figures immediately after bone grafting procedure.
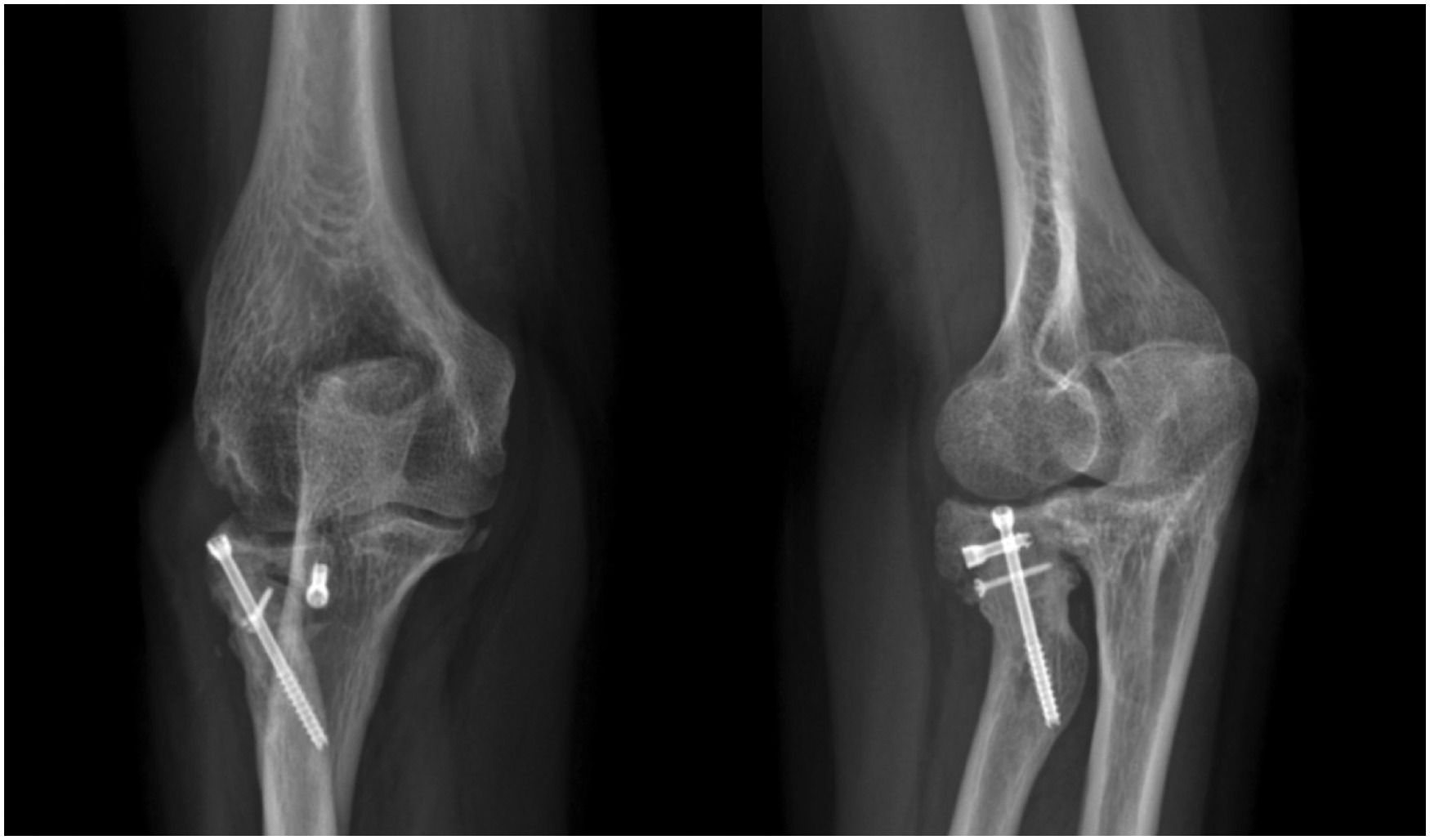
Radiographic figures showing union of the fracture site at 3 months follow-up.
Systematic review
The systematic review was performed according to Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 15 guidelines. The PubMed, OVID/Medline, Cochrane, Google Scholar, and EMBASE databases were searched using the keywords chosen according to the MeSH (Medical Subject Headings). The included the keywords “radial neck fracture nonunion”. Because the number of studies was limited, there were no restrictions in patient demographic characteristics, specific surgical procedure, publication status, and study period. The bibliographies of the retrieved studies were manually searched to identify other potentially relevant articles. The process of study selection was shown in Figure 5.
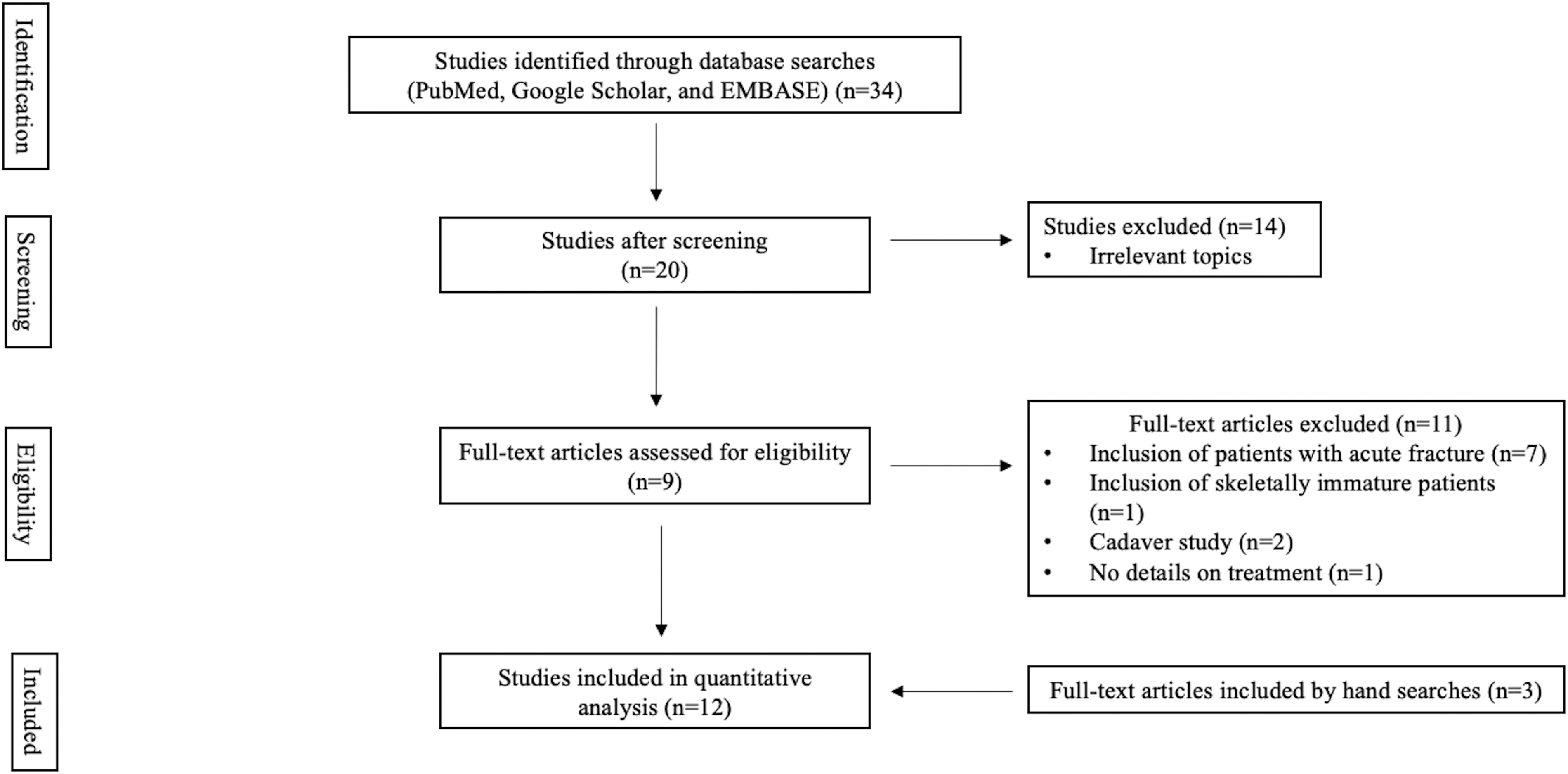
Flowchart of article selection according to PRISMA guidelines.
All abstracts were reviewed and individual articles on the diagnosis and management of the specific terms above were obtained. This review excluded textbook chapters, poster presentations, meeting abstracts and biomechanical studies. Only English written literatures were included in our review.
Two reviewers (E.K and H.J.L.) reviewed each full article independently, with the decision to include or exclude any study based on discussion and consensus. The level of evidence of each study was determined using the Oxford Centre for Evidence-Based Medicine criteria. 16 The decision to include or exclude studies was also discussed with expert orthopedic surgeons specializing in the upper extremities (I.H.J.). Data were extracted from the text, figures, tables, and supplementary material of each of the included studies. These data included demographic data, initial diagnosis and treatment, timing of nonunion presentation, functional status before and after the treatment, and the follow-up duration. These data were summarized in tables in Microsoft Office Excel (2013, Microsoft, Redmond, WA, USA).
Results
Case reports
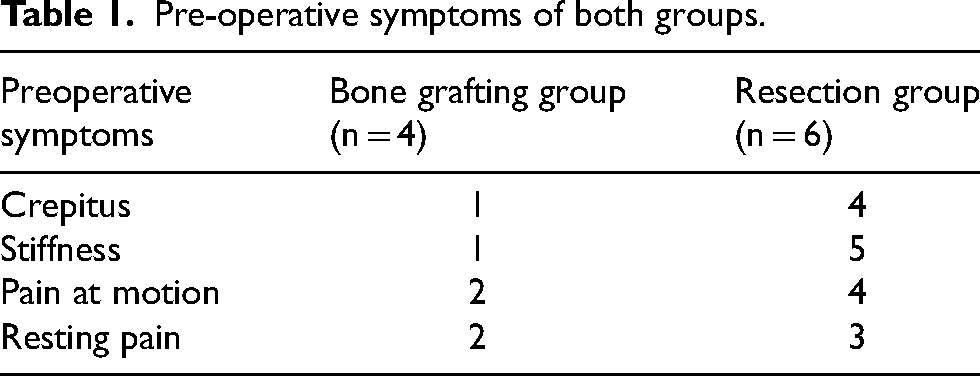
The mean age of the patients reported in this study is 46.9 years. The mean age for resection group (59 years) is older than bone grafting group (28.75 years). Resection group was observed to have more significant pre-operative symptoms including the presence of crepitus, stiffness, pain at motion and resting pain (Table 1). Table 2 shows the initial diagnosis for radial head fracture, associated injuries, pre- and postoperative ROM and MEPI score, articular surface congruency, degree of bone loss, and time to union in these patients. The mean of pre-operative extension-flexion and rotation arc for bone grafting group were 115° and 102.5°. The mean of pre-operative extension-flexion and rotation arc for resection group were 61.6° and 40°. The mean of post-operative extension-flexion and rotation arc for bone grafting group were 130° and 152.5°. The mean of post-operative extension–flexion and rotation arc for resection group was 109.1° and 82.5°. The mean pre-operative MEPI score for bone grafting and resection group were 75 and 57.5. The mean post-operative MEPI score for bone grafting and resection group were 93.75 and 82.5. The articular surface was congruent in all patients in the bone grafting group and incongruent in all patients in the resection group. None of the patients in the bone grafting group experienced bone loss, compared with five of the six patients in the resection group. Mean follow-up time was 17.9 months. All patients in the bone grafting group achieved union at an average follow-up time of 3 months. None of the patients in current series experienced neurovascular complications.
Pre-operative symptoms of both groups.
Cases demographic and presentations.
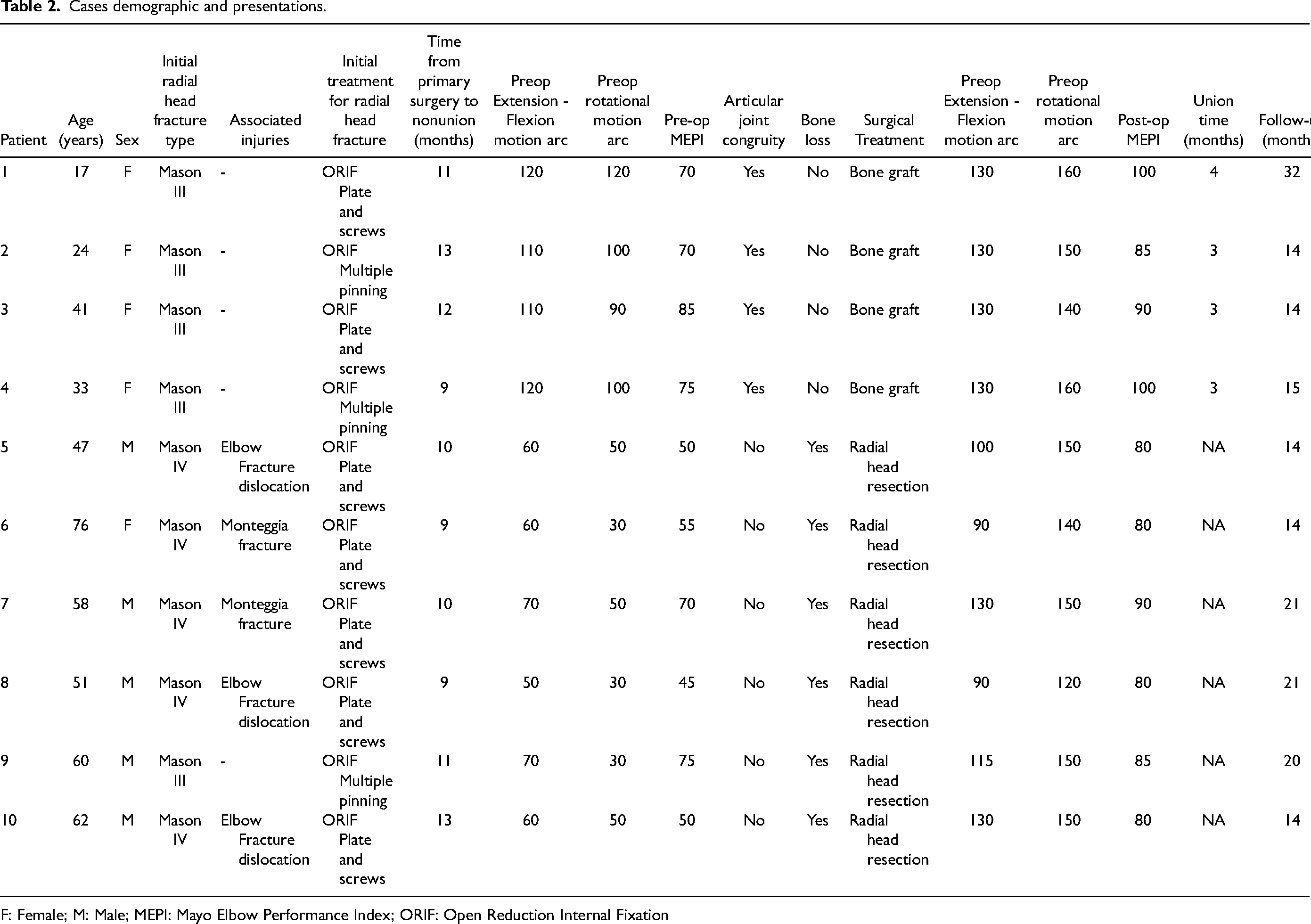
F: Female; M: Male; MEPI: Mayo Elbow Performance Index; ORIF: Open Reduction Internal Fixation
Systematic review
Our systematic review included a total of 12 publications of 19 patients with the mean age of 49 years (range 23–70 years). This review included 1 patient with bilateral radial neck nonunion following a conservative treatment and excluded one pediatric patients.5,11 (Table 3) Fracture of the radial neck was undetected initially undetected in one patient 1 and misdiagnosed for lateral epicondylitis in another. 2 The initial diagnosis ranged from isolated radial neck or head fracture or associated with other injuries. The incidence of radial neck nonunion was 73.7% and 26.3% following conservative and operative treatment, respectively. The average time of nonunion was 9.3 months with loss of ROM and discomfort while lifting objects as initial symptoms.
Demographic characteristics of the patients in each included study.
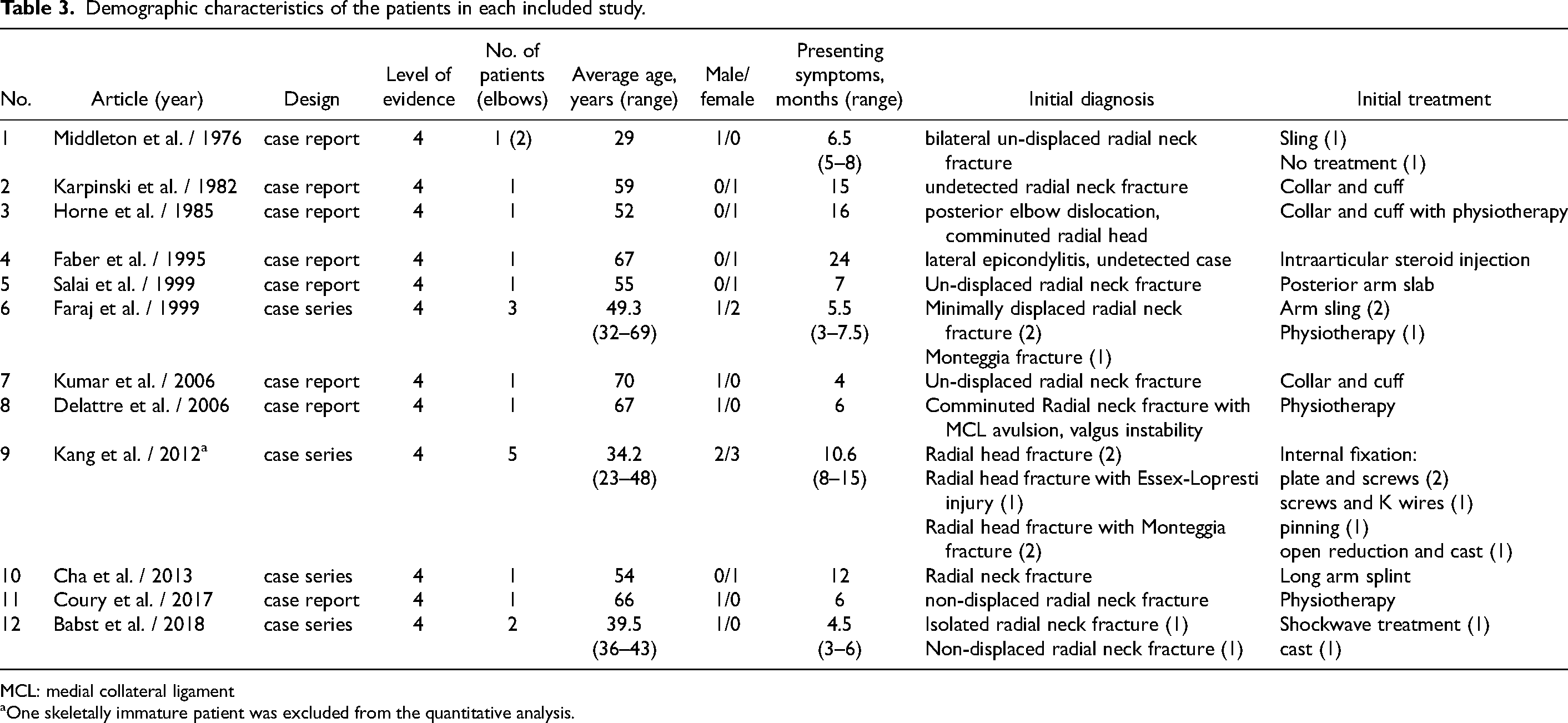
MCL: medial collateral ligament
One skeletally immature patient was excluded from the quantitative analysis.
Fourteen patients presented with nonunion of the radial neck fracture after conservative treatment with the mean age of 53.2 years and five patients presented with post-operative radial neck nonunion with the mean age of 34.2 years. Eight of total 19 patients (42.1%) received surgical treatment for radial neck nonunion which varied from bone grafting with or without internal fixation (three patients), radial head replacement (two patients) and radial head excision (two patients). No treatment were described for two patients.4,13 Two patients refused surgical treatment despite symptomatic progression.2,3 The details of nonunion treatment and summary of clinical outcomes were described in Table 4.
Type of nonunion treatment and summary of clinical outcomes.
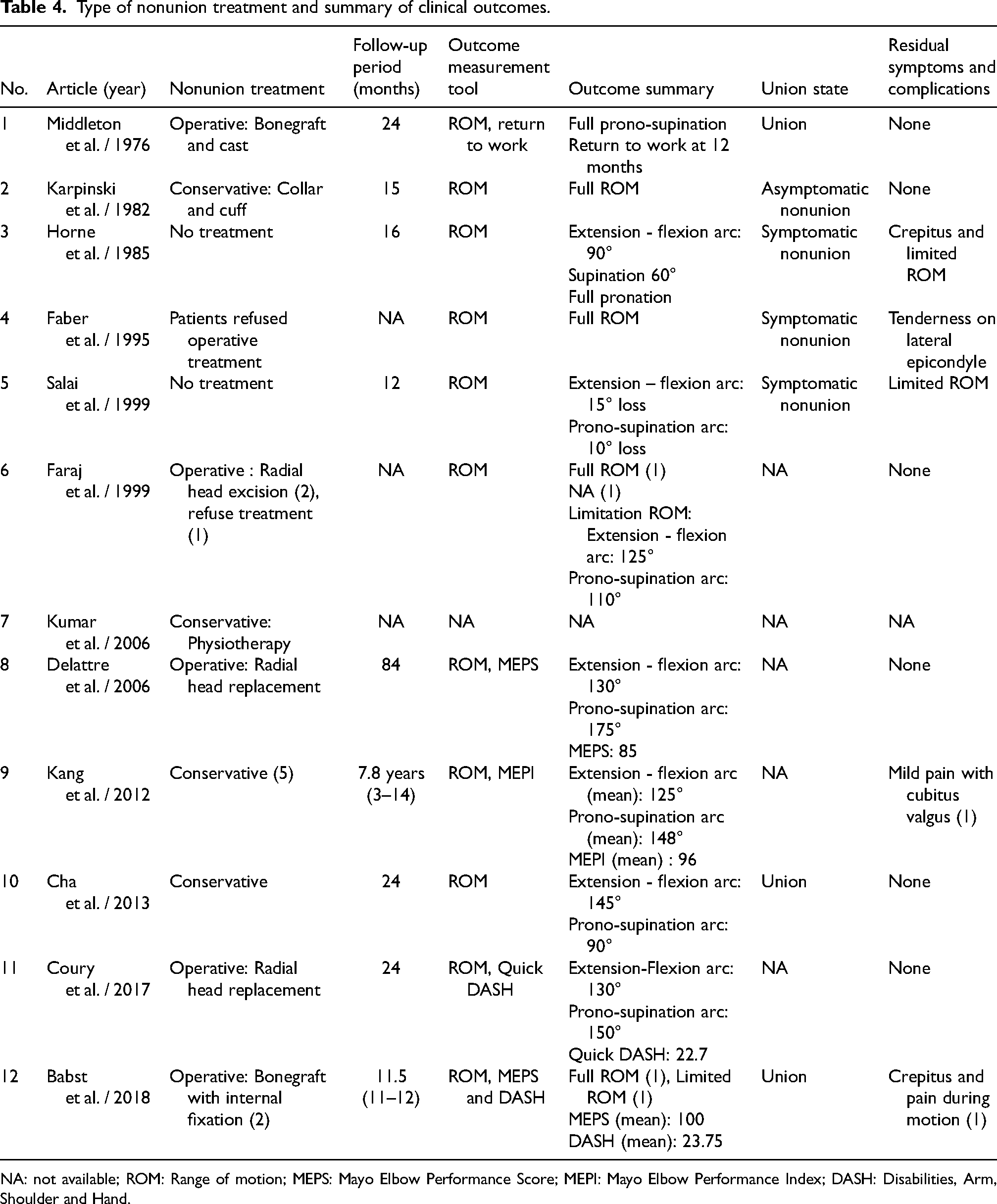
NA: not available; ROM: Range of motion; MEPS: Mayo Elbow Performance Score; MEPI: Mayo Elbow Performance Index; DASH: Disabilities, Arm, Shoulder and Hand.
At the final follow up of 51.2 months. There were 14 patients remained asymptomatic and five patients (26.3%) still complained of having symptoms. 17 Three literatures were unable to describe the follow up time for the total of five patients.2,3,18 ROM was the most common outcome measurement tool to be used, nevertheless only five studies described specific ROM with the mean of 131° for extension-flexion arc and 134.6° for prono-supination arc.3,11,19–21 Objective measurement tools were only used in four studies which were MEPS, MEPI, DASH and Quick DASH which resulted in four patients being rated to have good to excellent outcome.11,17,20,21 The final outcome were failed to be described for two patients with one was due to refusal of treatment.3,18
Discussion
The cause of radial neck nonunion is multifactorial.11,22 The causes of nonunion at this site remain unclear, although the intra-articular position is thought to contribute to the susceptibility of the intraosseous blood supply to the neck. An insult from high energy injury to the vasculature complex in the radial head–neck region at the time of injury is likely to be the major cause of radial neck nonunion as described in six patients in our case series.11,23
Both inadequate internal fixation and early rehabilitation may contribute to nonunion leading to an iatrogenic soft tissue injury that “feeds” the radial neck. Five of 10 patients (50%) in the current series were presented with associated injury which depicted a high-energy injury. The attempt of open reduction and internal fixation to fix radial head fracture add deleterious effects on the precarious vasculature of the radial neck. The systemic inducing factors to nonunion (smoking, diabetes, non-steroid anti-inflammatory drugs abuse, alcohol abuse, and nutritional deficiency) were ruled out in all cases. Most of the local factors had been found in our cases as major cause of the nonunion. The mean age of our patients is relatively young and comparable with those presented with post-operative radial neck nonunion in the systematic review. Despite the young age, the incidence of nonunion is high hence, we postulate that age is not a major cause of having nonunion. The nonunion is rather associated with the associated lesions and the degree of bone loss. We also presume that the background of having a post-operative nonunion is related to tenuous blood supply of the radial neck later worsen by surgical insult.
The current systematic review revealed that treatment for the initial injury was mostly conservative. This might be caused by the lesser associated injury compared to our reported patients who underwent surgical procedure as initial treatment.
Our systematic review revealed that despite conservative treatment, the incidence of radial neck nonunion is still as high as 73.7%. Various treatment methods, including conservative and surgical methods3,5,6,11 with high variability due to the small numbers of patients were described with lack of consensus guidelines. Patients with asymptomatic nonunion of the radial neck, despite any previous treatment, require no further treatment, as conservative treatments have demonstrated satisfactory clinical outcomes.1,2,4,6,11,13 However, conservative treatments were described multifariously lead to no conclusion for preferred method.
Surgical approach is recommended for symptomatic nonunion presented more than 6 months. 17 Most of these patients will experience deterioration of elbow function which disturb the daily activities and precipitate arthritic changes in the joint. According to the current systematic review, the outcome of surgical treatment for radial neck nonunion was reported to be favorable.3,5,17,20,21 Treatment options consist of prosthetic (radial head replacement) 20 and non-prosthetic reconstruction (ORIF and radial head excision).3,5,17,19,21
Bone grafting had been recommended for young and high-demand patients which resulted in satisfactory outcomes.3,22 The aim of the procedure is to improve radio-capitellar alignment and ROM, reduce pain and lessen the risk of future degenerative changes in the joint. In the present study, the decision to perform bone grafting was dependent on preoperative evaluation which includes the initial diagnosis, the involvement of associated injuries, and preoperative ROM. Bone grafting is recommended for patients with a less severe initial radial head injuries, less associated injury, congruent articular surface with the absence of bone loss.
In cases of severe bone loss, radial head replacement is considered a good treatment option to restore a painless and stable elbow. Nevertheless, in the current series, radial head replacement was not performed after indepth discussion regarding risks and benefits of the procedure with our patients. The radial head resection was favored by the patients for its single operation manner with the least chance of failure from prosthetic-related complications. Resection of the radial head has been considered appropriate for older and low-demand patients which resulted in satisfactory outcomes.3,6 In the present study, patients underwent radial head resection if they had a poorer initial diagnosis with more significant complains, higher energy injuries, and evident initial fracture displacement. The most important factors indicating radial head resection include non-congruent articular surfaces and significant bone loss. Other factors include the initial presence of associated injuries and more limited preoperative ROM.
Limitations
Our study has several limitations including the small number of patients due to the scarcity of this condition. This also limits us to perform comparative analysis between two groups which explains the lack of statistical analysis in the current study. Other limitation include the different types of fracture and primary surgical treatment which may influence the nonunion course, the absence of radial head replacement procedure as an alternative to radial head resection procedure, retrospective design of the study, and the short-terms follow-up. Nonetheless, this study provides largest number for postoperative symptomatic radial neck nonunion along with the treatment plan and systematic review.
Conclusions
Symptomatic radial neck nonunion following surgical intervention is rare. Operative treatment is advocated for symptomatic cases. This study highlights the surgical decision making in these patients’ cases in which articular congruity and bone loss status plays major role. Surgical treatment for symptomatic radial neck nonunion resulted in favorable outcome.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.