
Abstract
Introduction
Cubital tunnel syndrome (CuTS) is the second commonest compressive neuropathy in the upper limb, after carpal tunnel syndrome. The prevalence ranged between 1.8% and 5.9%. 1 Common sites of compression of the ulnar nerve are between the two heads of flexor carpi ulnaris/ aponeurosis, Osborne's ligament, within the arcade of Struthers and medial epicondyle. Diagnosis of CuTS is commonly made by physical signs (McGowan grade 1-3) and symptoms. Nerve conduction test (NCT) confirms the diagnosis and quantifies the severity. 2 In our locality, the practice is similar. However, they have their limitations. For example, NCT may cause electromagnetic interference in patients with implantable cardiac devices. 3 And in case of absent electric signal due to severe CuTS, electromyography (EMG) may be needed as an adjunct to NCT. Classical EMG finding of lower motor neuron denervation would be the presence of fibrillation potentials, positive sharp waves, and increased insertional activity. 4 Sometimes, a spectrum of clinical findings can make the diagnosis unclear, and symptoms and signs of C8 radiculopathy may overlap with CuTS (Figure 1).
Ultrasonography is able to visualize peripheral nerves in selected areas of extremities and facilitate the diagnosis of pathological conditions. Ultrasound (USG) of the median nerve at the carpal tunnel is widely employed. Ulnar nerve enlargement is often observed in USG in patients with CuTS, especially just above and below the site of maximal compression i.e., hourglass deformity. So far, no USG data for CuTS was available for use in the Hong Kong Chinese population. Our study aims to compare the USG size of the ulnar nerve between CuTS patients and control subjects, to find the cut off size for diagnosis in our locality, and to validate the use of USG as an adjunct in CuTS diagnosis.
Materials and methods
Cases were recruited between April 2021 and October 2022. We recruited 18 patients with clinical and NCT confirmed CuTS in the orthopedic outpatient clinic of United Christian Hospital. Among them, five patients had bilateral disease. So there were a total of 23 CuTS elbows in the patient group (CuTS + ve). In the control group (CuTS-ve), there are 42 normal elbows: eight are from the asymptomatic, NCT-ve contralateral elbows of the CuTS + ve group, while 34 normal elbows from 17 subjects are recruited from the same orthopedic clinic who presented with other upper limb complaints with a normal NCT. Cases with elbow deformities, old ulnar nerve injuries, ulnar nerve subluxation and postoperative cases for cubital tunnel syndrome were excluded (Figure 1).
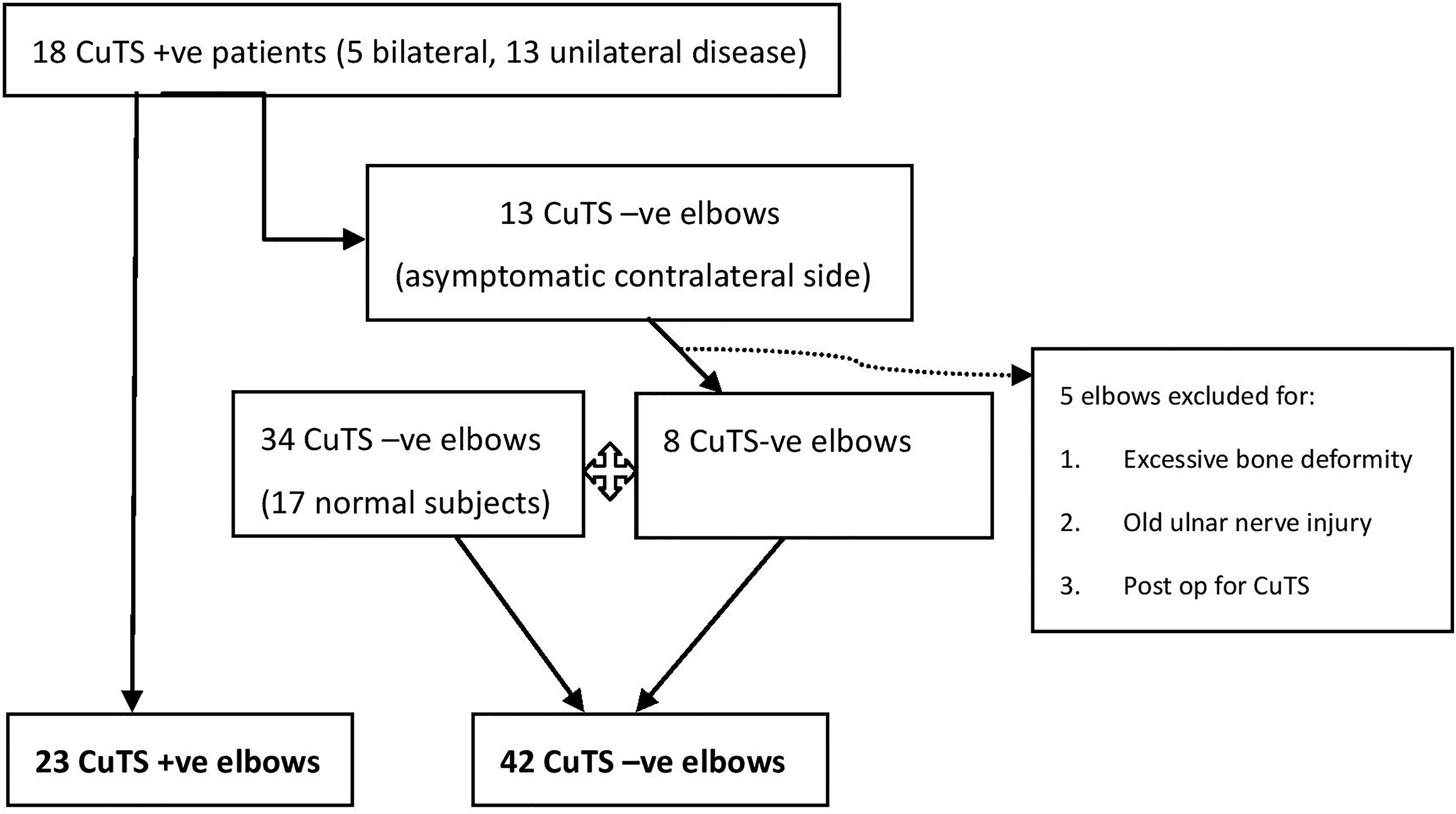
Diagram showing the process of recruiting CuTS+ve and CuTS-ve elbows.
Clinical symptoms of CuTS consisted of weakness or clumsiness of the ulnar nerve innervated muscles, numbness and paresthesia of the fourth and fifth digits of the hand, and medial elbow pain. Patients were assessed by orthopedic surgeons at the outpatient clinic for pinprick sensation in the territory innervated by the ulnar nerve, muscle strength of the first dorsal interosseous and abductor digiti minimi using the Medical Research Council grading, presence of Tinel sign and ulnar nerve thickening.
The NCTs in the same hospital were performed with standard surface/ring electrodes, stimulation techniques, recording techniques, and filter settings as described by Kimura. 5 Based on the American Association of Electrodiagnostic Medicine Criteria, ulnar neuropathy at the cubital tunnel was diagnosed in the presence of one of the following abnormalities: absolute nerve conduction velocity slowing above the elbow, decrease of nerve conduction velocity of more than 10 m/s across the elbow, decrease in amplitude of more than 20%, absent ulnar sensory responses, or signs of denervation in muscles innervated by the ulnar nerve on electromyography.
Demographics (gender and age) between the two groups would be compared.
General Electric Logiq P9 ultrasound machine with linear array transducer (L8-18i-RS Probe) was used to trace the ulnar nerve around the elbow (Figures 2 and 3). USG is performed or supervised by an orthopedic surgeon specialized in hand surgery to minimize interobserver variability. The subject is seated upright, with shoulder flexed to 90 degrees and his/her elbow rested on a table placed in front (Figures 4 and 5). The ulnar nerve cross-sectional area (CSA) was measured at six different levels and positions: over the medial epicondyle (ME) in 90 degree elbow flexion and full extension, 2cm and 5 cm distal to the ME in 90 degree elbow flexion, 2 cm and 5 cm proximal to the ME in 90 degree elbow flexion (Figure 6). The mean CSA values at these positions between the two groups would be compared, with p < 0.05 being statistically significant. A cut off CSA value for CuTS diagnosis was derived with receiver operating characteristic (ROC) curve. Correlation between ulnar nerve CSAs and NCT was obtained with Pearson correlation coefficient.
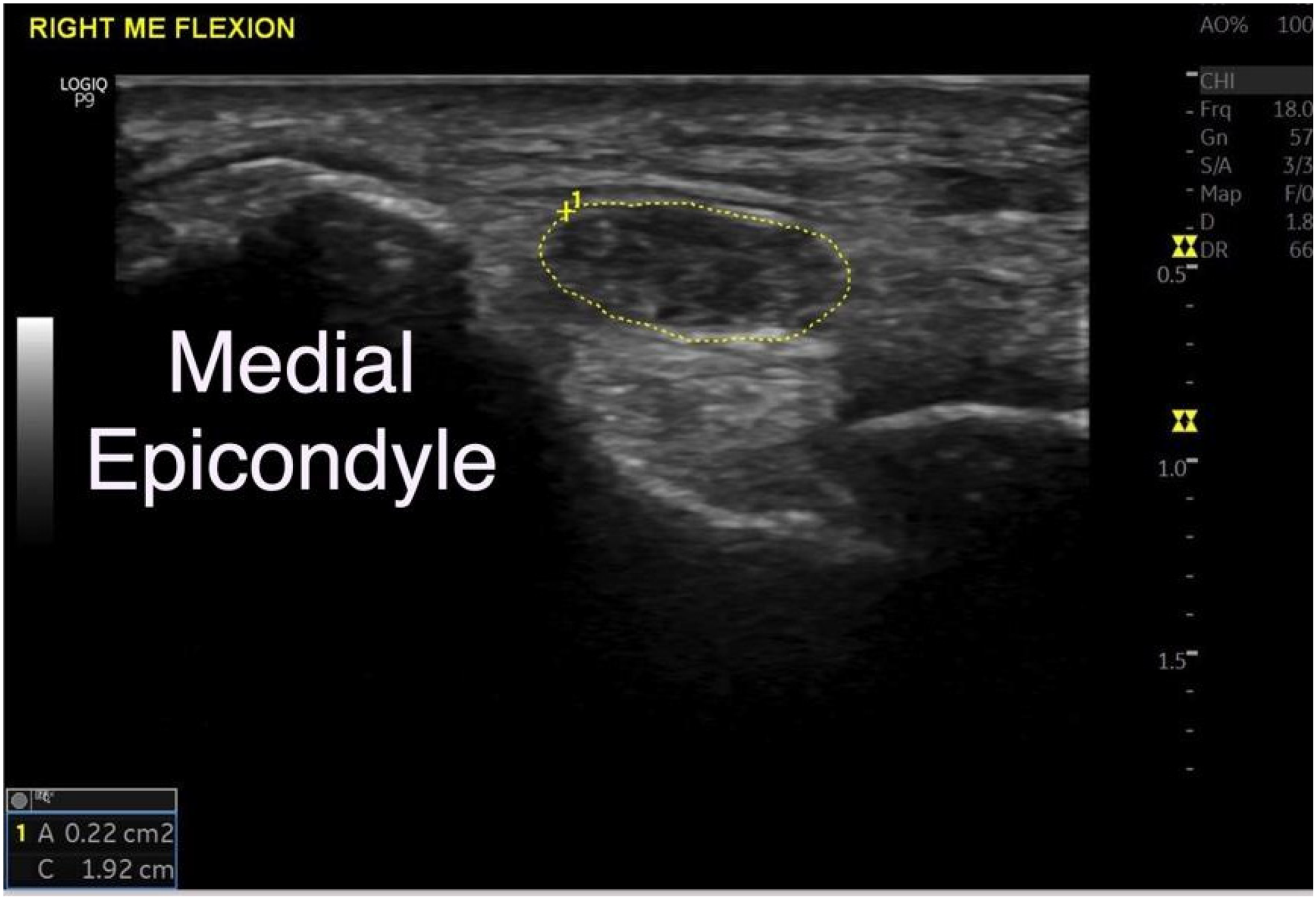
Ulnar nerve tracing (in yellow) at the medial epicondyle in a patient with CuTS. It shows a grossly swollen nerve.
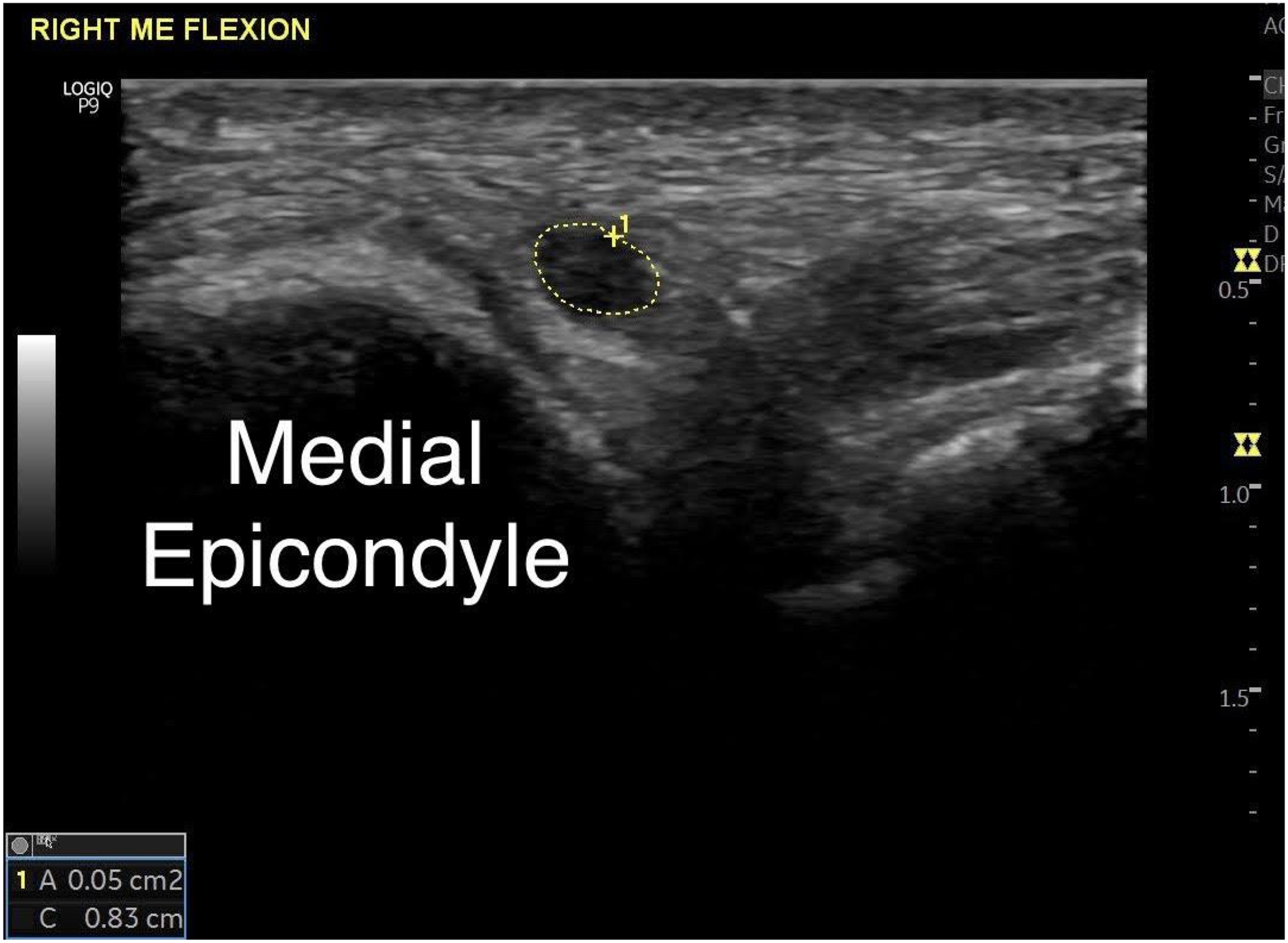
Ulnar nerve tracing (in white) at the medial epicondyle in a normal subject. The nerve has a normal caliber.
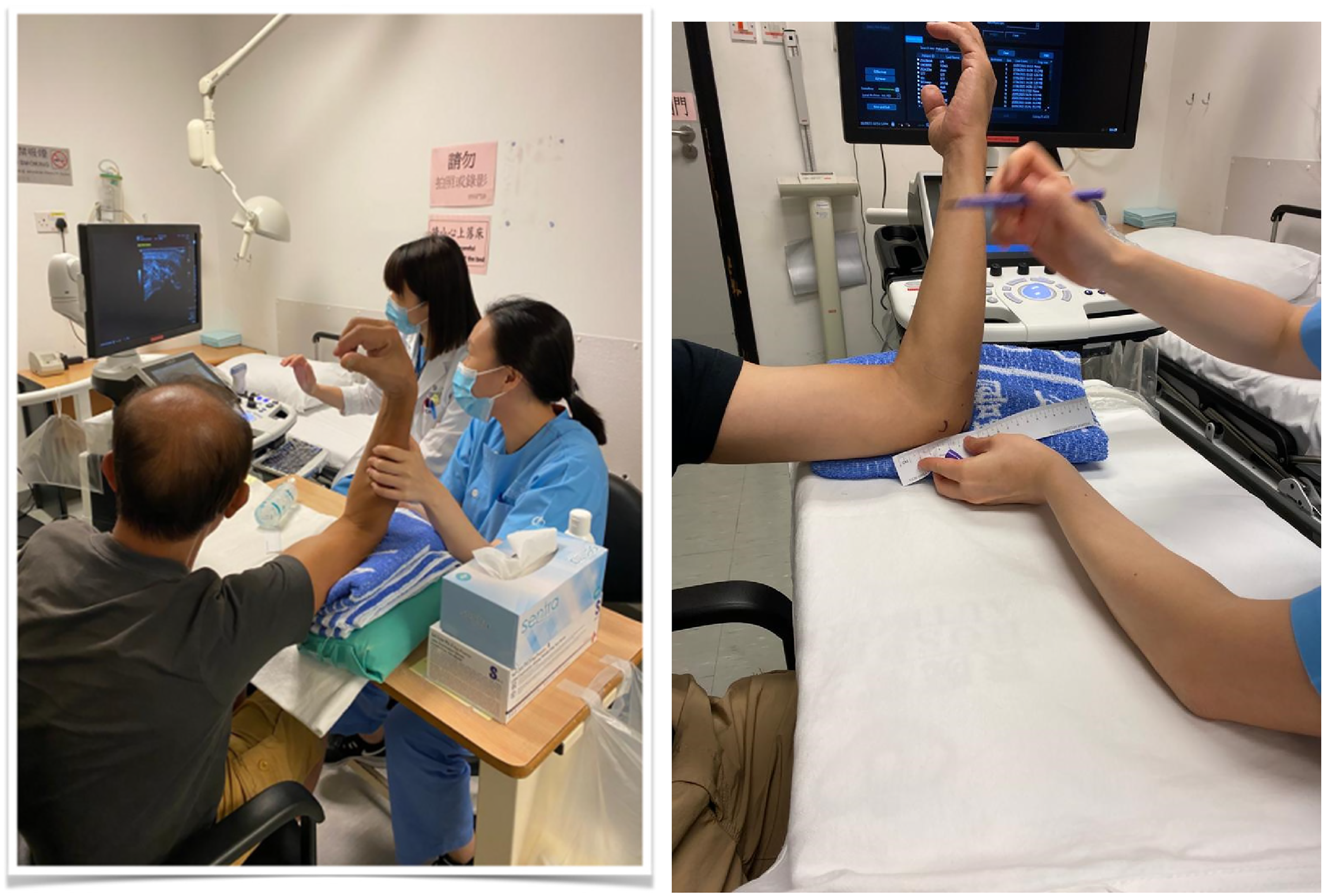
Subject positioning during USG: Shoulder flexed to 90 degrees and elbow rested on a table in front.
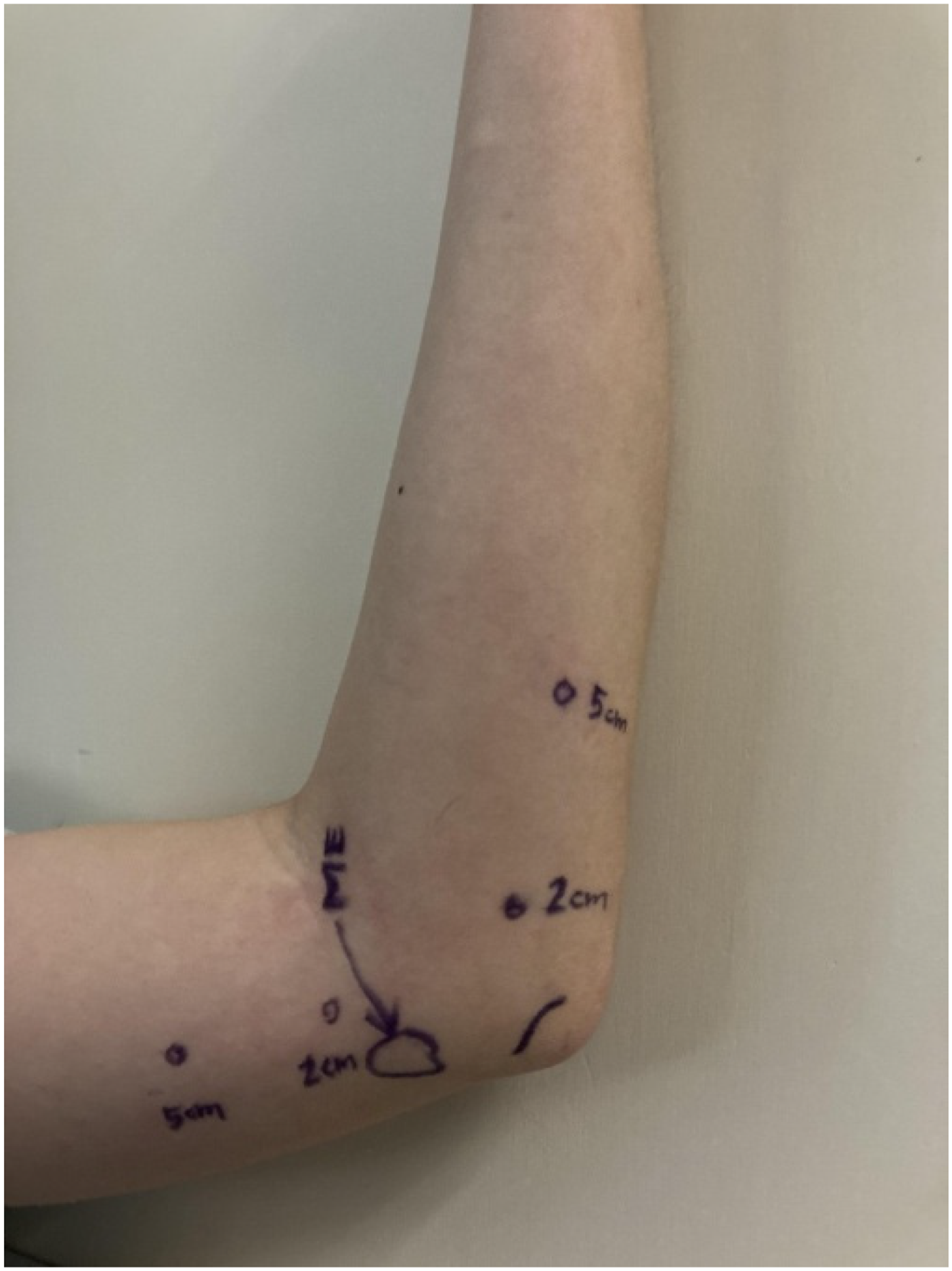
Landmarks used for ulnar nerve USG tracing.
Results and discussion
There are 20 males and three females in the patient group; 27 males and 15 females in the control group (p > 0.05). The mean age of the patient group is 61.2, while the mean age of the control group is 56.6 (p > 0.05).
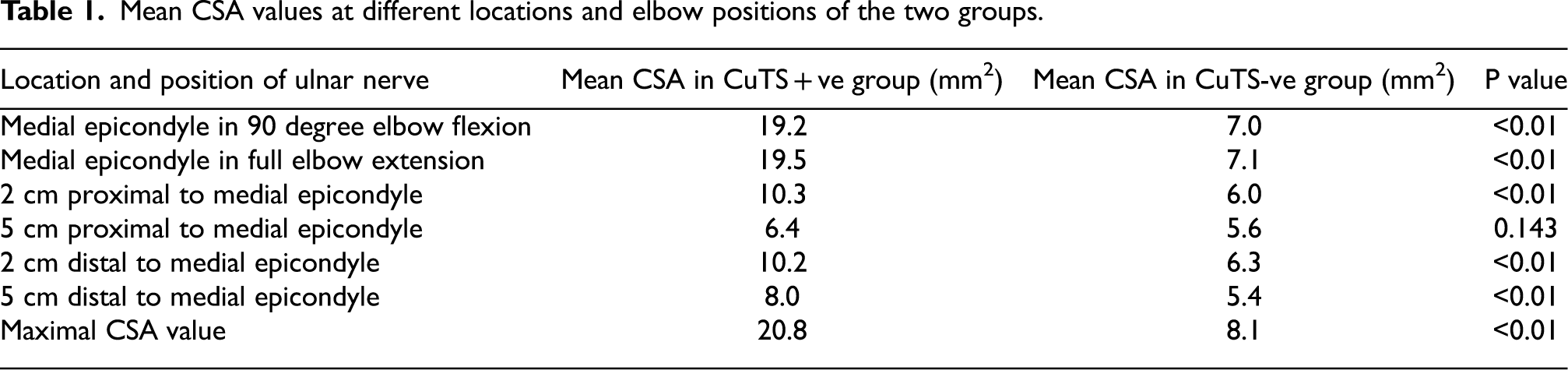
The ulnar nerve cross-sectional area is larger at all recorded locations and positions around the elbow for the CuTS + ve group. Most differences between the two groups are at the medial epicondyle in 90 degree elbow flexion and full elbow extension. Apart from 5cm proximal to medial epicondyle, differences in cross-sectional area in other points between the two groups are statistically significant (Table 1). A possible explanation would be: ulnar nerve is most swollen at the medial epicondyle in the CuTS + ve group, hence there will be gradual tapering of the swelling away from the pathological site. And 5cm away from the medial epicondyle is the farthest point from the compression site recorded from our study.
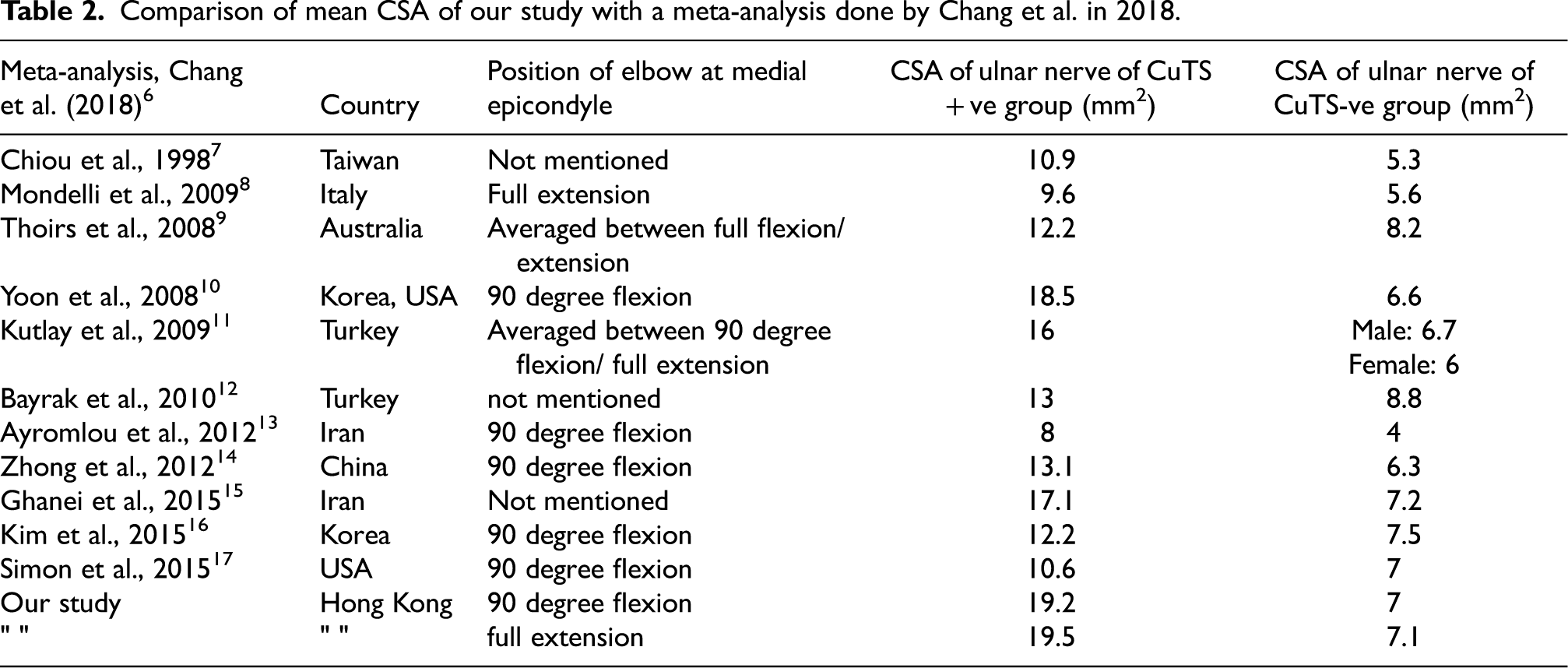
Comparing our study result to other similar overseas studies, our mean ulnar nerve CSA at the medial epicondyle in the CuTS + ve group, regardless of elbow position, is larger (Table 2). This can be possibly due to a delayed initial presentation to the clinic by patients in our locality. Most CuTS cases in our clinic are at McGowan grade 3.
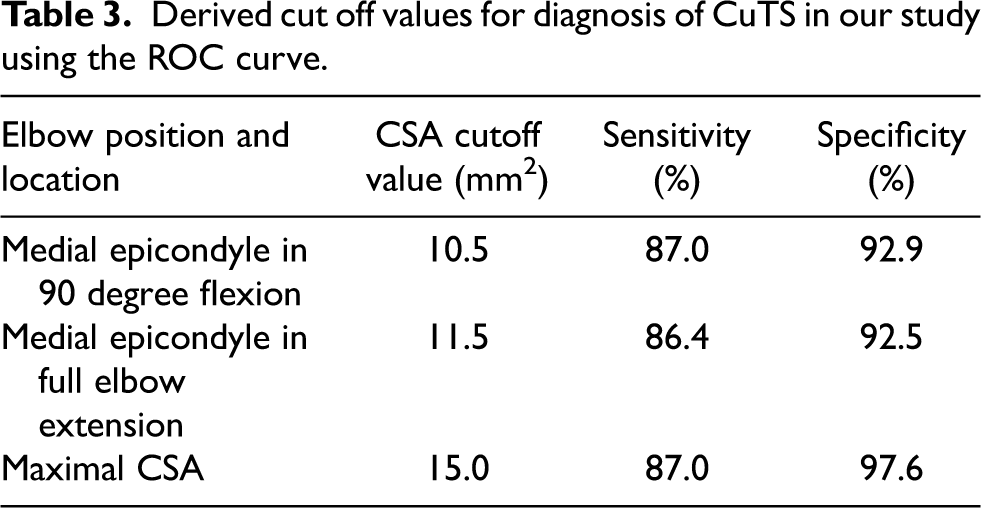
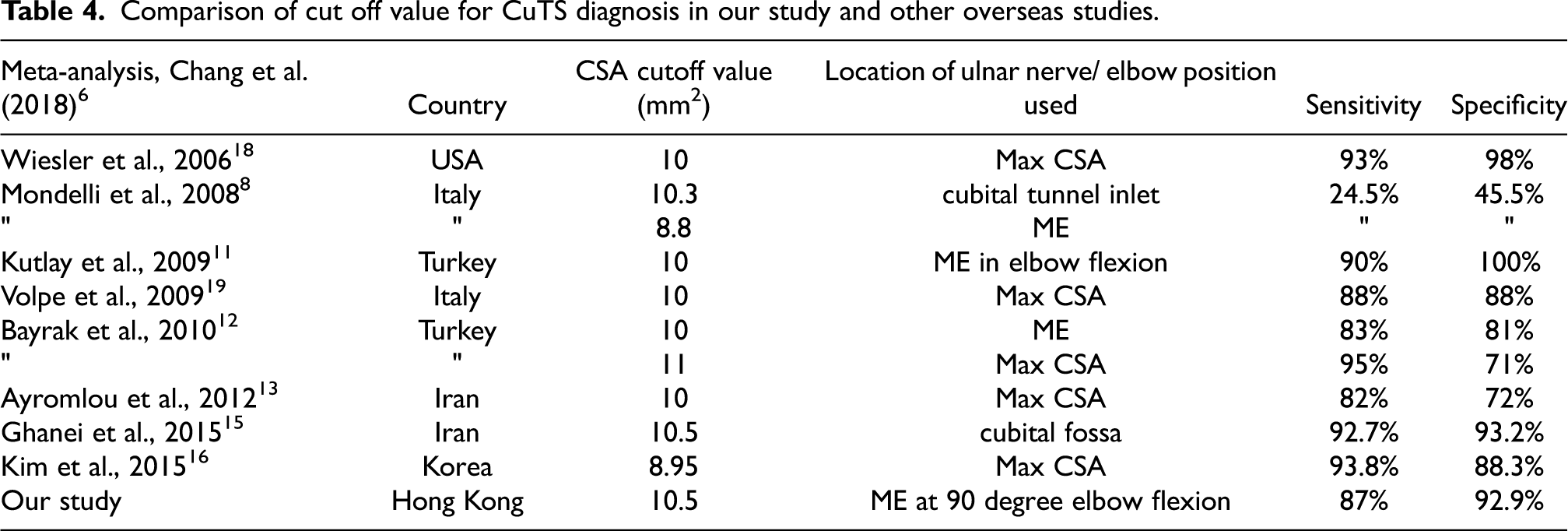
Our cutoff value for CuTS diagnosis is 10.5 mm2 at medial epicondyle at 90 degree elbow flexion (Table 3). It is similar to other studies (Table 4).
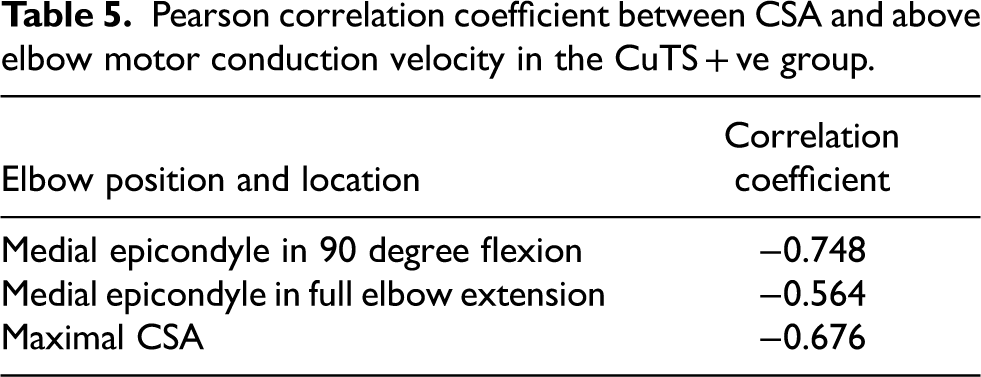
Results showed a strong negative correlation between CSA value and the above elbow motor conduction velocity, meaning the lower the velocity above elbow i.e., the more severe the CuTS, the larger the CSA of the ulnar nerve is in ultrasound (Figure 7 and Table 5). This result further shows that CSA value in USG correlates well with the severity of CuTS. We could also utilize this scatter diagram to roughly estimate the above elbow motor conduction velocity based on the ultrasonic ulnar nerve measurement at the elbow, or vice versa, during daily practice.
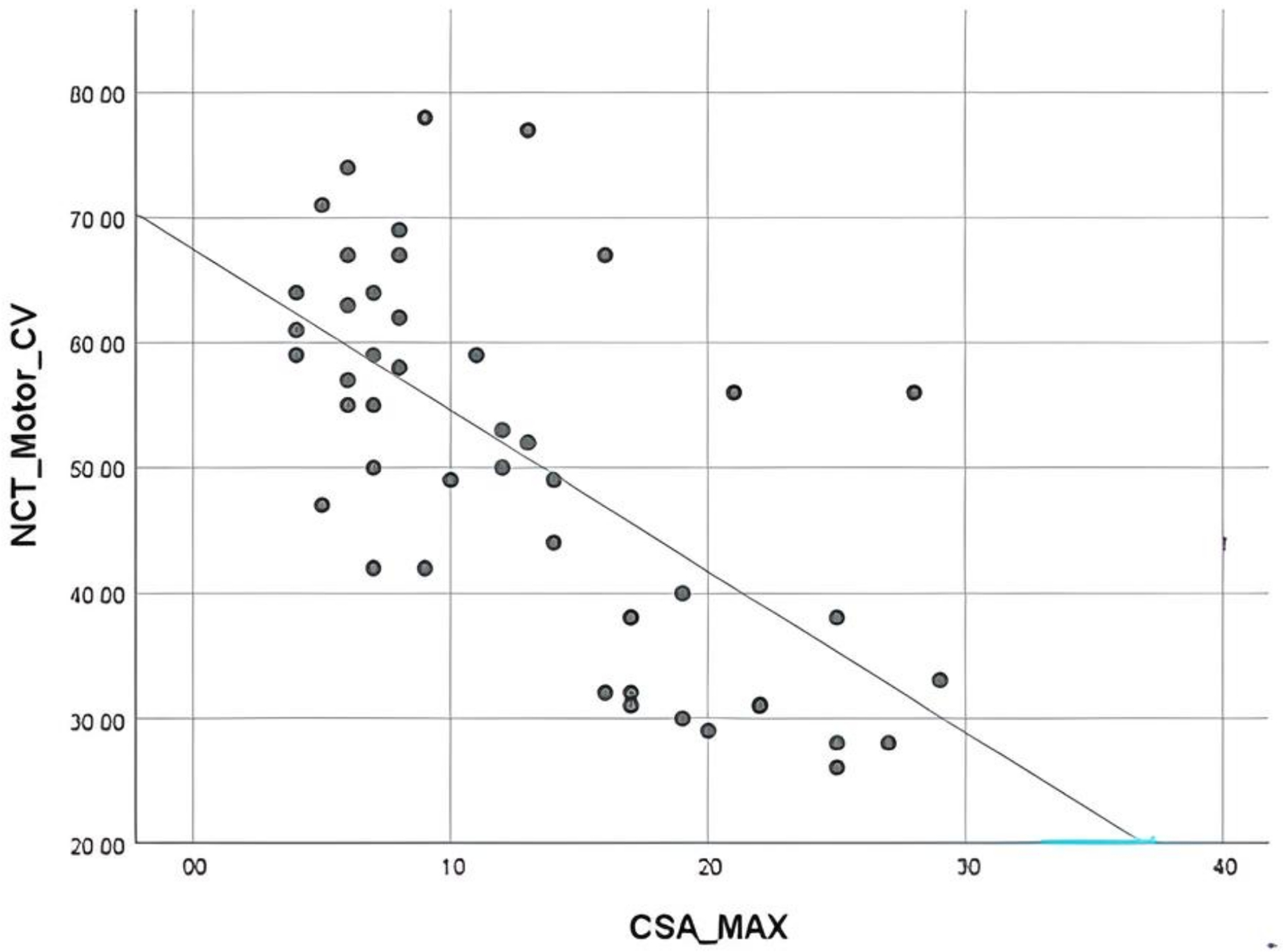
Scatter diagram for correlating above elbow motor conduction velocity and maximal CSA in both groups.
There are several limitations in our study. The status of subjects undergoing USG (patients vs control) is not blinded to the examiner. Furthermore, we did not evaluate the USG findings in patients who only present with clinical symptoms of cubital tunnel syndrome but with a normal NCT.
Conclusion
Ultrasound of the ulnar nerve can be used as diagnosis, or adjunct to diagnosis of cubital tunnel syndrome with high accuracy and safety. In cases where NCT shows no response, or those with double crush syndrome (both cervical radiculopathy and compression at the cubital tunnel), USG would be particularly useful. It can also be used to delineate possible anatomical etiologies at the cubital tunnel such as anconeus epitrochlearis muscle, occult ganglion, ulnar nerve dislocation, etc. In future, with more similar studies performed, more standardized USG techniques and diagnostic criteria for cubital tunnel syndrome could be established.
Mean CSA values at different locations and elbow positions of the two groups.
Comparison of mean CSA of our study with a meta-analysis done by Chang et al. in 2018.
Derived cut off values for diagnosis of CuTS in our study using the ROC curve.
Comparison of cut off value for CuTS diagnosis in our study and other overseas studies.
Pearson correlation coefficient between CSA and above elbow motor conduction velocity in the CuTS + ve group.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.