
Abstract
Pelvic and acetabular fractures are challenging injuries to treat. This review evaluates three-dimensional intraoperative imaging and navigation-guided percutaneous SI, trans-iliac, trans-sacral, and acetabular screw placement versus conventional methods performed with C-arm imaging. A systematic search of MEDLINE, Embase, and Cochrane was performed. Two reviewers independently extracted data into a collaborative data form designed a priori and piloted prior to its use. Descriptive statistics are presented where applicable. Summary statistics analysis was presented based on the fracture type. Continuous data such as fluoroscopic and operative time were compared with unpaired Student t-test and pooled data of revision rate and complications were compared with chi-square analysis with an alpha set at 0.05. The rate of complications using conventional fluoroscopy was 11.3% (26/230) compared to three-dimensional navigation (6.7% (40/597), X2 (DF: 1, N = 827) = 4.79, p = .028.) which translated to a higher rate of revision surgeries in the conventional fluoroscopy group (10.9% vs. 0.8%) X2 (DF: 1, N = 827) = 47.8, p ≤.001. Average fluoroscopic time was lower for studies using three-dimensional navigation (28.8 ± 14.3 s, n = 71) compared to conventional fluoroscopy (57.8 ± 4.2 s, n = 38, p ≤.001). Three-dimensional navigation during minimally invasive pelvis and acetabular fracture fixation may have some benefits. Level of evidence: IV.
Introduction
Pelvic and acetabular fractures are serious injuries with high morbidity and mortality rates (between 9% and 30%).1,2 Many patients who survive do not return to baseline activity levels due to long-term issues including chronic pain (30%–85%).3,4
Management of pelvic and acetabular fractures includes temporization using skeletal traction or external fixation; definitive management includes open reduction and internal fixation (ORIF) or image-guided percutaneous fixation.5,6 Internal fixation with plates and screws requires extensive surgical exposure and risks damage to neurovascular structures.6,7 Image-guided fixation techniques may minimize the need for soft tissue dissection, decreasing pain and infection risk.7,8 Due to the complex anatomy of the pelvis and acetabulum, there are risks of screw malposition and neurovascular injuries.9,10 During percutaneous posterior pelvic ring fixation, screw malposition occurs in 12% of patients with normal sacral anatomy and 28% in those with a dysmorphic sacrum. 11
Computer-assisted navigation has been introduced as a potential way to improve accuracy and outcomes following percutaneous pelvic and acetabular fixation. Iso-C three-dimensional (3D) and ARCADIS Orbic 3D are intraoperative image-based navigation devices used in trauma and elective cases. The 190° arc C-arm provides 3D reconstruction based on multiple fluoroscopic images. 12 Several studies found Iso-C 3D exhibits greater sensitivity and specificity for evaluating hardware position and reduction in acetabular fractures.6,10,13,14 O-arm is a 2D fluoroscopic and 3D multi-planar volumetric imaging system used to provide intraoperative CT imaging. 15 These tools may support optimal hardware position, reducing the risk of neurovascular injury. 16 It has been used in spinal surgeries to guide decompression and in trauma surgery for ORIF.17–20 Studies show promising results for intraoperative 3D navigation with good accuracy (97%).9,16 Coste et al. 20 evaluated the use of O-arm in osteosynthesis of pelvic fractures, concluding that O-arm offers safe, precise margins during the surgery and is not associated with any malpositioning or secondary screw displacement.
Intraoperative image-based navigation also has drawbacks related to implementation and radiation exposure. Theologis et al. 19 performed a study on 10 cadavers, comparing the use of C- versus O-arm for left-sided S1 screw fixation. The set-up time for O-arm was longer and radiation exposure was higher compared to cases done with standard C-arms alone, carrying health implications for operating room personnel and patients.
To better understand how 3D imaging systems compare to their 2D counterparts during percutaneous pelvic and acetabular SI screw fixation, we performed a systematic review to assess 3D intraoperative imaging and navigation-guided percutaneous SI, trans-iliac, trans-sacral, and acetabular screw placement to conventional methods alongside conventional C-arm imaging. Specifically, we aimed to evaluate the accuracy of placement, quality of reduction, duration of radiation exposure, and operative time. We also analyzed complication types and rates.
Methods
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for conducting and reporting systematic reviews. 21 The study protocol was registered prospectively on The International Prospective Register of Systematic Reviews (PROSPERO) (ID: CRD42020222285). No data was derived from experimental or clinical observations in human or animal subjects.
Source of funding
No funding was received for this study.
Search strategy
A systematic search of MEDLINE, Embase, and Cochrane was performed on 21 November 2020, including all studies from inception to the search date. Search terms included “pelvi$,” “acetabul,*” “percutaneous screw,” “3D imaging,” and “Navigation” (see the Appendix for a list of MESH terms).
Eligibility criteria
The research question and study eligibility criteria were established a priori. All studies evaluating acetabular, sacral, and pelvic ring fractures treated with S1 or S2 percutaneous screws in skeletally mature patients were included. Exclusion criteria were as follows: surgical procedures such as open reduction or adjunct fixation, sawbones or cadaveric studies, non-human studies, studies lacking adequate clinical information, conference proceedings or abstracts without an available full-text, review papers, and case reports describing five cases or less.
Study screening
Two independent reviewers (LN and KL) assessed the titles and abstracts and applied the eligibility criteria using the online software Rayyan (2010, Qatar Computing Research Institute, Doha, Qatar). Any discrepancies at this stage were automatically included in the full-text review. Full texts were then screened for duplicates; discrepancies were discussed between the reviewers and resolved by consensus. References of included studies were reviewed manually to identify any additional relevant studies for inclusion.
Data extraction
Two reviewers (LN, KL) independently extracted data from the included studies into a collaborative data extraction form (Google Sheets, Google, CA, USA) which was designed a priori and piloted prior to its use. Relevant collected data included study characteristics, injury and patient demographics, operative outcomes, accuracy of screw placement, and complications.
Risk of bias of included studies
The Methodological Index for Non-Randomized Studies (MINORS) was used to assess the quality of included non-randomized studies. Each paper was assigned a score from 0 to 2 against 12 validated criteria for non-randomized studies. The maximum score was 16 for non-comparative studies and 24 for comparative studies. 22 We categorized the quality of evidence a priori based on a previous systematic review: < 5 indicated very low-quality evidence, 6–9 low quality, 10–14 fair quality, and > 14 good quality. 23 Randomized controlled studies were evaluated with the revised Cochrane risk-of-bias tool (RoB2). 24 RoB2 assesses numerous study domains as either low risk, some concerns, or high risk of bias based on set criteria.
Statistical analysis
The Cohen kappa statistic (κ) was calculated at each screening stage to evaluate the level of inter-reviewer agreement and categorized as follows: substantial agreement: κ > 0.60; moderate agreement: 0.21 < κ < 0.60; and slight agreement: κ < 0.21. 25 Inter-class correlation (ICC) was calculated to determine agreement between reviewers’ risk of bias assessments. Descriptive statistics including means, standard deviations, and ranges are presented where applicable. A separate summary statistics analysis was presented based on fracture type (pelvic ring vs. acetabular), as was defined a priori. Due to the literature's heterogeneity and inconsistency in reported outcomes, we were unable to perform a formal meta-analysis. Finally, continuous data such as fluoroscopic and operative time were compared with unpaired Student t-test, and pooled data of revision rate and complications were compared with chi-square analysis with an alpha set at 0.05.
Results
Study characteristics
The initial search identified 195 unique studies; 20 met the inclusion criteria (Figure 1). There were two randomized controlled trials, two prospective comparative studies, two retrospective comparative studies, and 14 case series that met eligibility criteria.11,26–44 The included studies were published between 1992 and 2017. Sixteen studies investigated the use of 3D imaging on percutaneous pelvic ring screws; four studies focused on acetabular screws. A total of 789 patients were included across the 20 studies and 322 of which were female.
PRISMA flowchart for the systematic search strategy utilized.
Study quality
The included studies were mostly of level IV evidence. There were two studies of each level I, II, and III evidence. There was substantial agreement between reviewers at the title and abstract screening (κ = 0.72) and excellent agreement at full-text screening (κ =0.82). Similarly, there was substantial agreement between assessors for quality assessment scores using the MINORS criteria (ICC = 0.643). Included non-randomized studies had an average MINORS score of 13 ± 4 which indicates an overall fair quality of evidence. The randomized study was assessed using the RoB tool. Matityahu et al. 11 generally had a low risk of bias as the process of the randomization and selection of reported results were well done with minimal loss of data. It is important to mention that this study was multi-centered with a good sample size. Some concerns regarding the measurement of the outcome were noted as a pre-determined and strict definition for screw misplacement was used and they lacked information regarding blinding.
Results for pelvic ring fractures
Of the 16 studies which included pelvic ring fractures, there were 713 included patients.11,27–36,40–44 The mean age of 44.6 ± 15.6 years (range: 13–94). A total of 38% (n = 271) were female. The mean length of time between injury and surgery was 9 days (range: 1–217). Table 1 summarizes these studies.
Demographic data of included studies.
Of the four comparative studies which investigated the use of 3D navigation on percutaneous pelvic fixation, three compared the Iso-C 3D C-arm to conventional 2D fluoroscopy.11,29,33 The additional comparative study compared a robotic system (TiRobot) performed autonomously to robotic-assisted screw fixation and conventional 2D fluoroscopy. 35 Most of the case series described CT scan-guided percutaneous pelvic fixation.27,28,30–32,34,40–42,44 Mu et al. 43 were the only ones to describe the results of Iso-C 3D C-arm guided fixation.
Screw misplacement
Complications rates were higher in procedures that used conventional fluoroscopy (11.3% (26/230)) compared to 3D navigation (6.7% (40/597), X2 (DF: 1, N = 827) = 4.79, p = .028) (Table 2). Higher complication rate also translated into a higher revision rate in the conventional group (10.9% vs. 0.8%) X2 (DF: 1, N = 827) = 47.8, p ≤ .001).
Comparison of complication and revision rates between conventional fluoroscopy and 3D navigation.
Matityahu et al. 11 performed a subgroup analysis of previously randomized patients. They included 130 patients that were either treated with conventional fluoroscopy (n = 58), 2D navigation-based imaging (n = 18), or 3D navigation (n = 54). After a blind review of the 109 patients with the non-dysmorphic sacrum, they found nine misplaced screws in the conventional group (total of 73 screws, 12%), six in the 2D navigation (total of 22 screws, 27%), and 0/66 (0%) in the 3D navigation group. The observed difference was even higher among dysmorphic sacrums with 7/22 (32%) misplaced screws for the conventional group and 0/12 (0%) in the 3D group.
In a comparative cohort study, Zwingman et al. 33 reported the results of consecutive patients treated before (n = 87, 131 screws) and after (n = 54, 63 screws) the implementation of 3D navigation. As mentioned by the authors, there was high variability among surgeons which makes direct comparison between the conventional and navigation groups difficult. Fourteen different surgeons had individual revision rates varying from 0% (0/40) to 29% (7/24); most were low-volume surgeons (< 15 SI screws over an 8-year period). 3D navigation technology lowered the incidence of screw malpositioning (19% with navigation vs. 58% conventional). They also saw a reduction in revision for screw perforation (1/63, 1.6% vs. 13/131, 9.9%). Screw perforations were seen on post-operative CT scans. The authors did not report cases of neurologic deficit/symptoms (Table 3).
Screw perforation and complications for the percutaneous placement of pelvic screws.
Operative time and radiation exposure
In 122 cases, the average operative time for percutaneous pelvic fixation using 3D navigation was 134.6 ± 31.3 min. Average fluoroscopic time was lower for studies using 3D navigation (28.8 ± 14.3 s, n = 71) compared to conventional fluoroscopy (57.8 ± 4.2 s, n = 38, p ≤.001).
Wang et al. 35 compared 22 cases of SI screws placed freehand using fluoroscopy and 23 robot-assisted cases. While they showed no difference in complications or revisions, they reported longer mean operative time with the robot (150.0 min (range: 75–230 min) vs. 104.0 min (60–154 min), p = .158). However, both the number of guide-wire insertion attempts (average 1.0 vs. 7.0, p < .001) and the radiation exposure were significantly lower with the use of the robot (mean = 6 s vs. 36 s, p < .001).
Using Iso-C 3D, Li et al. 29 also reported lower fluoroscopy time in their navigation group (46.4 s ± 2.5 vs. 75.4 s ± 6.9, p < 0.001) and SI screw placement time (19.5 min ± 2.2 vs. 30.9 min ± 5.7, p < .001) compared to conventional fluoroscopy.
Acetabular percutaneous screws
Although less common, advanced imaging is also used for acetabular percutaneous fixation. This includes a combination of anterior column, posterior column, anterograde, and retrograde screws. Swartman et al. 39 performed a retrospective study of 24 cases of CT navigated acetabular screw placement and 13 conventional cases using 7.3 mm cannulated screws. There was no significant difference between the two methods in terms of the quality of the fracture reduction (pre- and postoperatively) and the position of the screws relative to the hip joint and in the bone corridor. He et al. 26 compared a small cohort of patients receiving percutaneous fixation with 6.5 mm cannulated screws through Iso-C 3D (n = 10) and C-arm fluoroscopy (n = 12). They reported similar operative time and post-operative outcomes; radiation exposure was significantly less in the navigation group (26.9 s ± 2.1 vs. 80.7 s ± 3.0, p < .001). Schwabe et al. 37 described a case series of 22 cases using the ARCADIS Orbic (3D C-arm). They reported good clinical and radiologic results but lacked comparison to a conventional method.
Bleeding and infection rates
Overall, infection rates appeared to be higher with 3D versus conventional navigation (6/597 patients and 0/230 patients, respectively). Likewise, the incidence of bleeding was also higher with 3D navigation (1/597 vs. 0/230).
Timing of post-operative CT
The timing of post-operative CT was variable and not consistently reported.
Discussion
This study identified a trend towards improved precision and lower rates of perforation with the use of 3D navigation. This is based on the limited evidence from six higher-quality studies that compared outcomes from Iso-C 3D C-arm or robotics with conventional fluoroscopy. Included navigation-assisted case series showed rates of screw misplacement that ranged from 0% to 8%, which are lower than reported misplacement rates ranging from 12% to 23% using conventional techniques.45–47 Although these ranges cannot be directly compared due to variations in the methodology in referenced studies, they suggest that 3D navigation may reduce misplacement rates. Differences suggested in comparative studies were greater in cases that presented a greater technical challenge for the surgeons, including patients with dysmorphic sacrum. This suggests that there may be a benefit for those surgeons who are less comfortable with the procedure.
Ionizing radiation is a classified carcinogen by the WHO, with a likelihood for long-term sequelae. 48 One potential benefit of 3D navigation is decreased fluoroscopic time and radiation exposure for patients. The trend towards lower fluoroscopic time using 3D navigation compared to 2D fluoroscopy in the pooled analysis is seen in the comparative trials, suggesting a potential reduction in radiation exposure for patients and operating room staff using 3D navigation. Operative time stands as an indication of resource utilization and surgeon proficiency and is useful in determining the value of new techniques. The average operative time for pooled cases using 3D navigation (134 min) was slightly higher than the average operative time seen in cases using conventional fluoroscopy in the randomized control trial (RCT) performed by Wang et al. (104 min, p ≤ .001). 35 While it is difficult to directly compare these figures due to the small sample size of conventional cases, variability in anatomy, number of screws implanted, and surgeon experience, these findings suggest that operative time is relatively similar between the two methodologies. Maintenance of operative time in addition to the increased technological costs associated with using navigation suggests a significant financial burden associated with the implementation of navigation in minimally invasive pelvic fixation.
Of additional importance is a complication. No included studies demonstrated fewer complications or reoperations with navigation. Only Wang et al. 35 directly compared rates of complications and revisions between fluoroscopy and navigation, showing no difference. However, pooled analysis of included studies showed the rate of revision surgeries in the 3D navigation group was 0.8% (5/597) compared to 11% (25/230) in the fluoroscopy group. All conventional fluoroscopy cases in which a revision was required were from a single study. 33 While the trends towards lower cut-out rates and radiation exposure are promising, there lacks evidence that 3D navigation reduces rates of reoperation and additional high-powered comparative studies are needed to better elucidate this relationship.
As only four studies investigated the use of 3D navigation in acetabular fracture fixation, two of which were comparative studies, it is difficult to draw any meaningful conclusions. The only significant difference seen in these studies was a trend toward a lower dose of radiation exposure in the navigation group. Included case studies reported good clinical and radiologic outcomes. More research is needed to identify the meaningful benefits of using 3D navigation in percutaneous fixation of acetabular fractures.
There is often a learning curve associated with the implementation of new technology, involving a period of skill acquisition associated with increased operative time and complication rates. 49 In Zwingman et al.'s 33 retrospective comparative study, all fluoroscopy cases were performed prior to incorporating navigation technology. This introduces a potential for bias within the results, as the surgeons may have been in the skill-acquisition phase during early fluoroscopic cases. When 3D navigation was implemented, the surgeons may already have developed proficiency, inflating the results of the navigation-assisted procedures. This bias has the potential to influence additional included studies, depending on the surgeon's comfort and experience using 3D navigation. Future studies may account for this learning curve by excluding the first set of navigation-assisted cases.
While the current literature on the use of O-arm in orthopedics focuses on spine surgery, the clinically significant outcomes are promising. Wang and colleagues demonstrated operative time for posterior lumbar interbody fusion in elderly patients was significantly shorter when O-arm was used compared to fluoroscopy. 50 It has been well established that prolonged operative time is associated with higher rates of infection in orthopedic surgeries, so this significant decrease in operative time may also represent decreased rates of infection. 51 Furthermore, a recent retrospective review showed that patients who underwent a transforaminal lumbar interbody fusion with O-arm navigation had significantly lower visual analogue scale leg and Oswestry disability index scores at 6 months post-operatively compared to patients who underwent the procedure using fluoroscopy. 52 It is suggested that these improved clinical outcomes are due to improved surgical accuracy, so would likely translate to pelvic and acetabular trauma in which outcomes are similarly reliant on accurate screw placement.
This systematic review was strengthened by its rigorous methodology, involving a comprehensive search of major databases. Reviewer bias was minimized by blindly completing the screening; conflicts were resolved via consensus with assistance from senior authors. This resulted in the inclusion of 713 patients. The range of demographic factors makes the results broadly applicable to the general population. To the authors’ knowledge, this study is the first of its kind to compare 3D navigation and conventional fluoroscopy in percutaneous fixation of pelvic and acetabular fractures.
The findings are limited by the low-quality evidence of included studies. As most of the included studies were level 4 evidence, with only one RCT, there is a risk of bias within the results. Since only four studies directly compare 3D navigation with conventional fluoroscopy, it is difficult to determine the true differences that exist between the two. There was significant heterogeneity in the methodology of included studies, involving varying fracture patterns and screw placements. This prevented the authors from performing a formal meta-analysis.
The paucity of high-quality evidence emphasizes the need for rigorous RCTs to elucidate the benefits of 3D navigated minimally invasive pelvic and acetabular fixation compared to conventional fluoroscopy. While 3D navigation has the potential to improve screw accuracy and reduce radiation exposure, large studies that are sufficiently powered to detect differences in rates of complications and revision surgeries are imperative to guide practice. 3D navigation is costly, with the O-arm capital costs estimated to be $700,000 CAD (∼ $575,000 USD) plus annual operating and maintenance costs. 53 Based on this study's equivocal results, it seems unlikely that O-arm's high up-front costs are worthwhile for pelvis and acetabular surgery alone but may be more acceptable if used for additional patient populations and injury patterns. Additionally, once the benefits of navigation on screw cut-out and revision rates are better understood, a cost-effectiveness analysis should be performed to evaluate the financial feasibility of implementing this technology.
Conclusion
This review demonstrates there may be limited evidence to support using 3D navigation during minimally invasive pelvic fracture fixation. Based on current evidence, there is no clinical impact of navigation on cortical perforations or neurovascular complications. The paucity of high-quality trials limits the applicability of these findings clinically. Research is needed to characterize the implications of navigation on complication and revision rates, radiation exposure, and cost-effectiveness before implementing this technology into routine practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix. MESH Search Terms
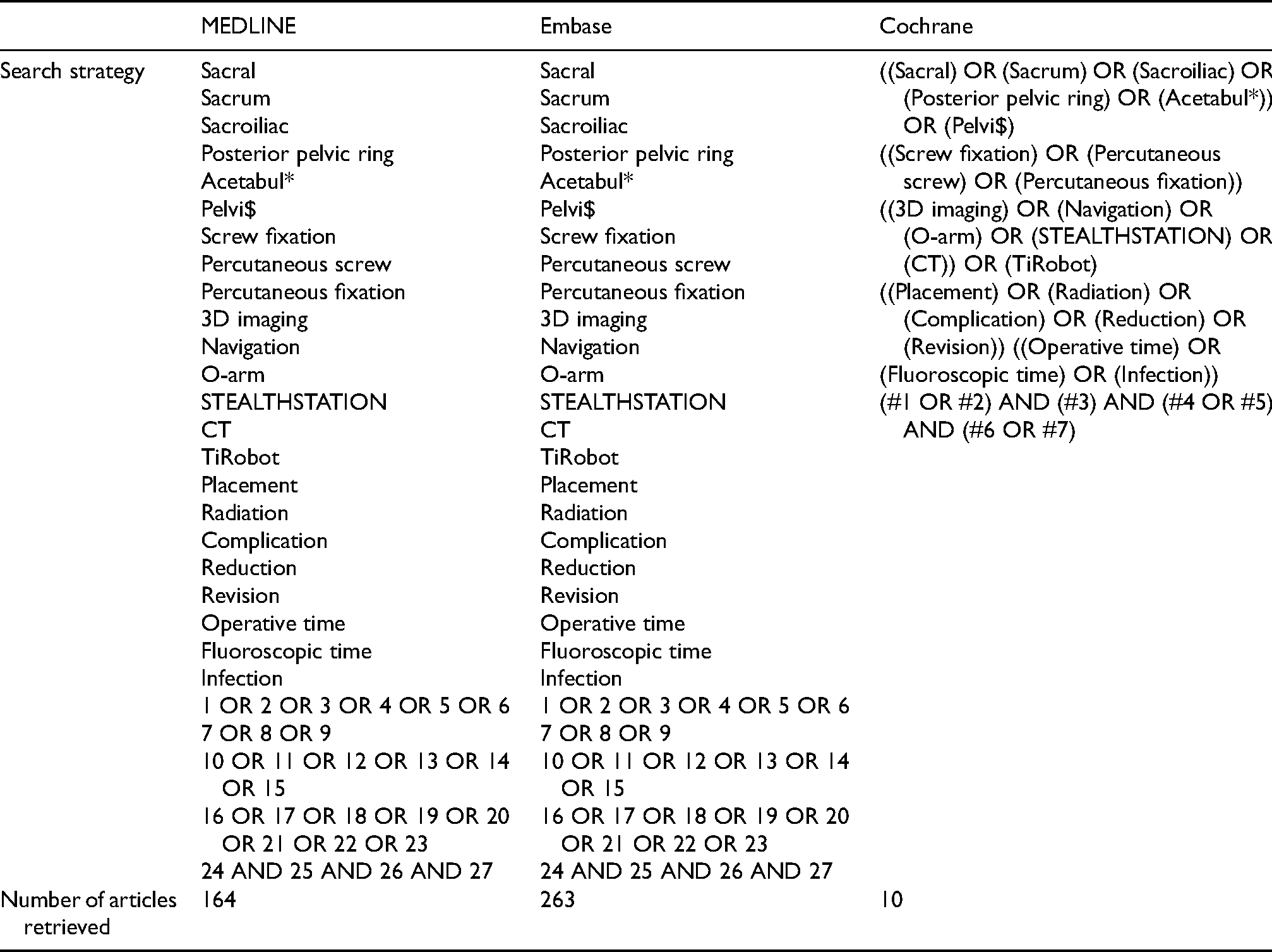
| MEDLINE | Embase | Cochrane | |
|---|---|---|---|
| Search strategy | Sacral Sacrum Sacroiliac Posterior pelvic ring Acetabul* Pelvi$ Screw fixation Percutaneous screw Percutaneous fixation 3D imaging Navigation O-arm STEALTHSTATION CT TiRobot Placement Radiation Complication Reduction Revision Operative time Fluoroscopic time Infection 1 OR 2 OR 3 OR 4 OR 5 OR 6 7 OR 8 OR 9 10 OR 11 OR 12 OR 13 OR 14 OR 15 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 24 AND 25 AND 26 AND 27 |
Sacral Sacrum Sacroiliac Posterior pelvic ring Acetabul* Pelvi$ Screw fixation Percutaneous screw Percutaneous fixation 3D imaging Navigation O-arm STEALTHSTATION CT TiRobot Placement Radiation Complication Reduction Revision Operative time Fluoroscopic time Infection 1 OR 2 OR 3 OR 4 OR 5 OR 6 7 OR 8 OR 9 10 OR 11 OR 12 OR 13 OR 14 OR 15 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22 OR 23 24 AND 25 AND 26 AND 27 |
((Sacral) OR (Sacrum) OR (Sacroiliac) OR
(Posterior pelvic ring) OR (Acetabul*)) OR (Pelvi$) ((Screw fixation) OR (Percutaneous screw) OR (Percutaneous fixation)) ((3D imaging) OR (Navigation) OR (O-arm) OR (STEALTHSTATION) OR (CT)) OR (TiRobot) ((Placement) OR (Radiation) OR (Complication) OR (Reduction) OR (Revision)) ((Operative time) OR (Fluoroscopic time) OR (Infection)) (#1 OR #2) AND (#3) AND (#4 OR #5) AND (#6 OR #7) |
| Number of articles retrieved | 164 | 263 | 10 |