
Abstract
Background
Total knee arthroplasty (TKA) is a successful procedure in treatment of degenerative disease of the knee, and optimal component placement is essential for long-term implant survival. The purpose of this study was to compare the accuracy of the accelerometer-based KneeAlign 2 (KA2) navigation system against conventional methods for accurate positioning of the femoral and tibial components in TKA in a Chinese population.
Methods
A total of 123 (37 conventional and 86 KA2) cases of elective primary TKA were reviewed. Hip-knee-ankle (HKA) angle, mechanical lateral distal femoral angle (mLDFA), and anatomical lateral distal femoral angle (aLDFA) were measured from hip-to-ankle EOS radiographs. Accuracy of conventional alignment and KA2 navigation system was assessed by measuring the difference between intraoperative goal and postoperative radiographic measurements of the components for each respective case.
Results
There was no significant difference between conventional alignment methods and KA2 navigation in achieving a neutral mechanical alignment of the lower limb. KA2 navigation was significantly more accurate than conventional alignment methods for optimal positioning of the tibial component in both the coronal and sagittal plane, while no significant difference between the two groups was appreciated in the positioning of the femoral component in the coronal plane.
Conclusions
TKA using the accelerometer-based KA2 system was found to offer a high degree of accuracy in component alignment, and in particular, significantly improved tibial component alignment in comparison with conventional alignment methods in a Chinese population. However, no significant improvements were observed in neutral mechanical axis of the lower limb alignment and femoral component placement in the coronal plane.
Background
Total knee arthroplasty (TKA) is one of the most commonly performed orthopaedic procedures; it had been demonstrated to be a highly successful treatment for end-stage degenerative knee disease, with functional and quality of life improvements.1,2
It is well established that optimal alignment is crucial for TKA implant survivorship and functional outcomes.3–7 For instance, Berend et al. (2004) demonstrated tibial component alignment of >3.0° varus was associated with a 17-time increased odds of implant failure and medial bone collapse. 8 May it be the traditional and most commonly adopted mechanical alignment technique that we are using in this study, or the kinematic alignment technique that has recently gained popularity, the ability to achieve an accurate bone resection and therefore implant placement remains crucial for the success of TKA.
Conventionally, the tibial and femoral component alignment in TKA is achieved by extramedullary (EM) and intramedullary (IM) alignment for bony resection.
In this study, hand-held accelerometer-based navigation (ABN) system KneeAlign 2 (KA2) (OrthAlign, Inc.; Aliso Viejo, CA) was used. It was designed to combine the accuracy of computer-assisted surgery (CAS) with the familiarity of conventional EM alignment systems, without the need of a large console for the registration and alignment feedback, as is required with most CAS systems. KA2 consists of a display console, reference sensor, and attachments to tibial and femoral jigs. The console communicates with the reference sensor wirelessly to guide femoral and tibial bone resection in the coronal and sagittal plane. Although long-term data are still pending, reports suggest that ABN is highly accurate in restoration of the neutral mechanical alignment of the lower limb, and in positioning of the femoral and tibial, components in TKA.9–12
The purpose of this study was to compare the accuracy of the ABN system against the conventional method for accurate positioning of the femoral and tibial components in TKA, and the ability to restore the neutral mechanical axis of the lower limb in a Chinese population.
Methods
Patient selection
This study was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (ethics approval number: 2017.458).
Between June 2017 and September 2020, 37 and 91 consecutive cases of elective primary TKA were performed with respectively conventional and ABN KneeAlign 2 (KA2) navigation system (OrthAlign, Inc.; Aliso Viejo, CA) in the Prince of Wales Hospital, Hong Kong; all surgeries were performed by senior surgeons experienced in knee arthroplasty. Patients were selected into each group at the operating surgeons’ discretion. Two patients from the conventional group and 19 patients in the KA2 group underwent bilateral TKA in the same surgical session.
Amongst the 91 cases of elective primary TKA performed with KA2, 5 cases were excluded due to incomplete data; the rest of the 86 cases were analysed.
Surgical techniques and procedures
The surgical techniques were standardised apart from the use of instruments for femoral and tibial osteotomies, with the aim to achieve distal femoral and proximal tibial cuts that are 90° relative to their respective mechanical axes in the coronal plane, and a tibial posterior slope of 3° in the sagittal plane. All TKAs were performed via a standard medial para-patellar approach with measured resection technique; with tibial and femoral osteotomies, soft tissue balancing, and then implantation of components with antibiotics-loaded cement. Implants used were either Legion or Journey II BCS total knee system (Smith & Nephew, plc.; Watford, UK).
For the conventional alignment group, the proximal tibia cut with EM alignment guide, and distal femur was cut with an IM alignment guide.
In the KA2 navigation group, the accelerometer-based alignment system was used for both proximal tibial and distal femoral osteotomy (Figure 1). The KA2 system was used as per the manufacturer's protocol, with the tibial and femoral jig, attached with a display console and reference sensor.

Intraoperative photos: use of KneeAlign 2 (KA2) navigation system (OrthAlign, Inc.; Aliso Viejo, CA) in proximal tibial and distal femoral osteotomy.
Radiological evaluation
The definitions of the radiographic alignment measurements were summarised in Appendix 1. The radiographic measurements were performed by an orthopaedic trainee and a postgraduate student; methods and surgical techniques were taught by a senior orthopaedic surgeon.
Preoperatively, weight-bearing anteroposterior (AP) full length hip-to-ankle radiographs were obtained with low-radiation-dose EOSTM imaging systems, from which the hip-knee-ankle (HKA) angle, mechanical lateral distal femoral angle (mLDFA), and anatomical lateral distal femoral angle (aLDFA) were taken (Figure 2). 13 For convention, all positive values represent a varus alignment, whereas negative values represent valgus alignment. The HKA angle is defined as the medial angle formed between the mechanical axis of the femur and the mechanical axis of the tibia. The mLDFA is defined as the lateral angle between the femoral mechanical axis, and a line tangent to the most distal aspects of the medial and lateral femoral condyles. The aLDFA is defined as the lateral angle between the femoral anatomical axis, and a line tangent of the most distal aspect of the medial and lateral femoral condyles. The preoperative difference between the mLDFA and aLDFA was calculated for each patient.
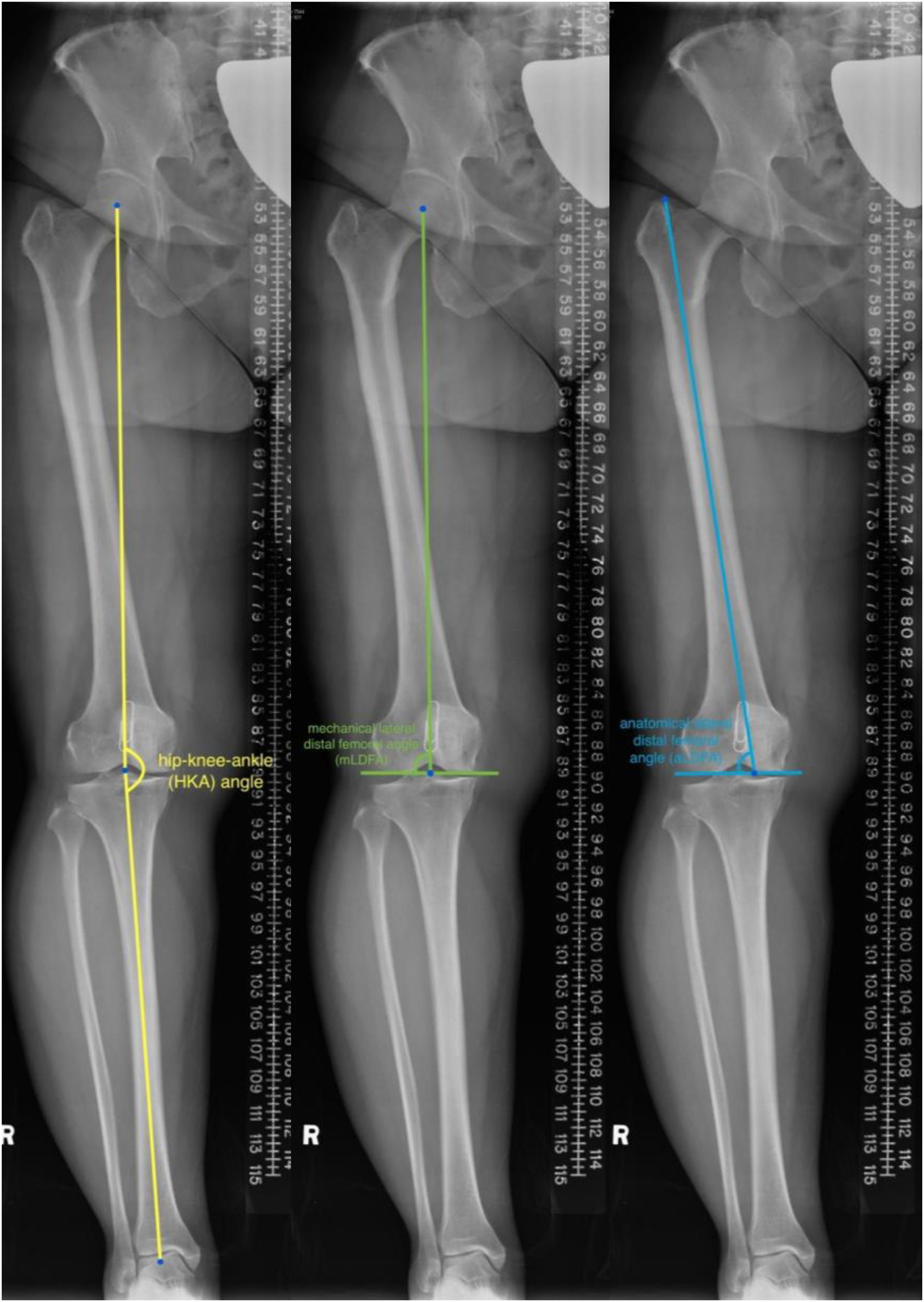
Definition of radiological measurements – preoperative alignments of the lower limb.
At the patient's first postoperative clinic visit, weight-bearing radiographs were obtained, including long-film hip-to-knee EOSTM, AP and lateral knee radiographs. The postoperative HKA angle, femoral component varus/valgus angle, tibial component varus/valgus angle, and tibial component posterior slope were measured. 14
The accuracy of the conventional alignment and KA2 navigation system was assessed by measuring the difference between the intraoperative goal and the postoperative radiographic measurements of the components for each respective case. A satisfactory result was taken as postoperative HKA angle of 180 ± 3°, femoral component coronal alignment of 90 ± 3°, tibial component coronal alignment of 90 ± 3°, and tibial component sagittal alignment (posterior slope) of 3 ± 2° (Figures 3 and 4).
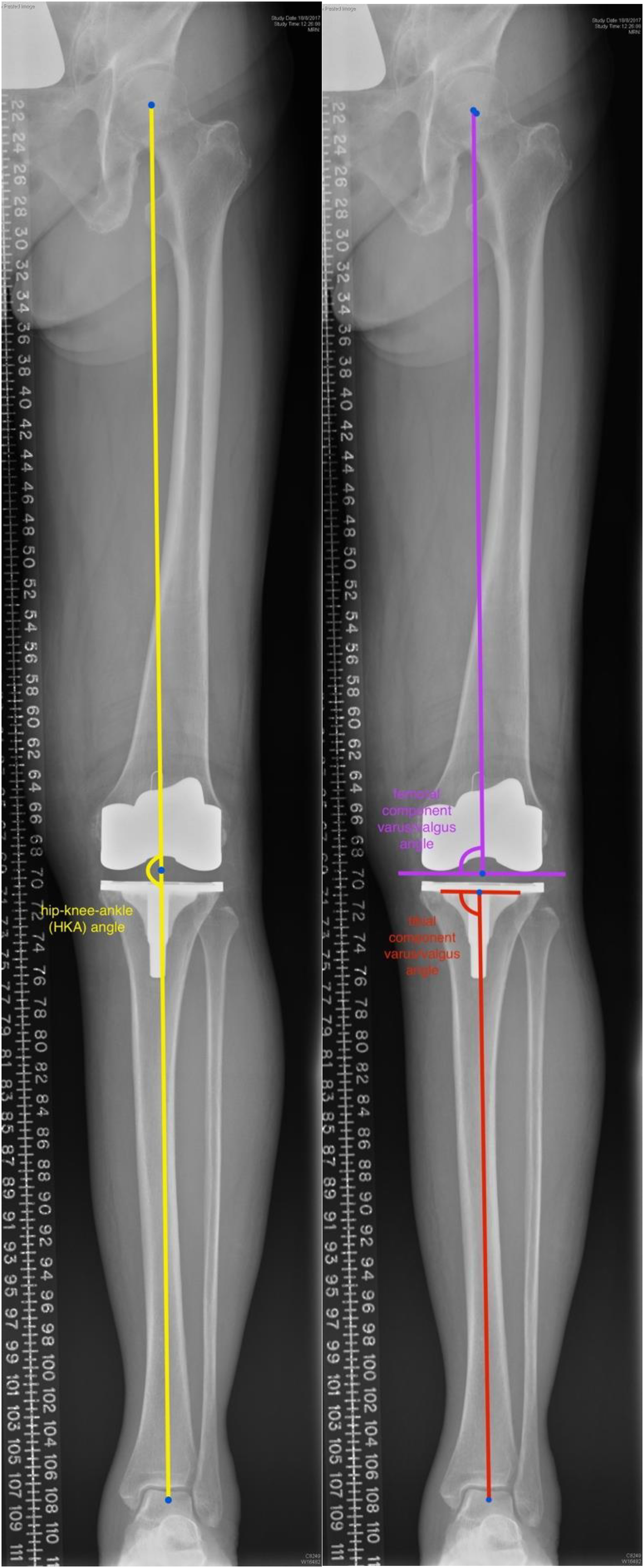
Definitions of radiological measurements – postoperative alignment in coronal plane.

Definitions of radiological measurements – postoperative alignment in sagittal plane.
Sample size calculation
From the results of our pilot study (unpublished), the allowable difference per single measurement is 0.4 with population variance is 1.9. Given β equals 0.8 and α equals 0.05, the calculated sample size is 30 (sample size estimation website, Centre for Clinical Research Biostatistics, Chinese University of Hong Kong).
Statistical analysis
Statistical analysis was performed to compare the accuracy of positioning of femoral and tibial components in TKA in the conventional alignment and accelerometer-based KA2 navigation groups. Continuous data, such as differences in the coronal and sagittal alignments of the components, were expressed in terms of mean and standard deviation of the mean and compared using two-tailed independent t-tests. Categorical data such as the number of outliers was analysed using Pearson's Chi-squared test or Fisher's exact tests. Further statistical analyses were carried out following the accuracies of different measurements. The HKA, femoral component coronal alignment, and tibial component coronal alignment with accuracy limit of ±3° within the target of 90°, percentage distribution of measurements within ±3°, <-3°, and >3°. Similar analysis was performed for posterior slope of tibial component with the measurement accuracy limit of ±2°. The above results were also graphically presented by the corresponding histograms and trendlines. Apart from calculating the percentages below and above the accuracy limits, tables showing the distributions on either a ±3° or ±2° intervals were provided to show the range of the mean differences. Inter-rater reliability was carried out to compare radiological measurements between two independent orthopaedic surgeons through intra-class correlation (ICC) and Cronbach α values. All p-values of <0.05 were deemed statistically significant. All statistical analysis was performed using IBM SPSS version 24 (Armonk, NY).
Results
Patient demographics
The age of the conventional alignment and KA2 navigation groups were comparable, at the mean age (± 1 standard deviation) of respectively 67.7 ± 8.0 and 69.5 ± 7.7 years (p = 0.256), whereas percentage of females are respectively 81% and 59%. All patients had severe osteoarthritis of the knee, with the exception of respectively 1 and 2 patients who had rheumatoid arthritis in the conventional and KA2 groups.
Mean number of months between preoperative and postoperative radiographs were 4.65 ± 6.70 (Median = 4.65; Range = 1.22 to 40.54 months) in KA2 navigation group and 3.09 ± 2.27 (Median = 2.10; Range = 1.22 to 10.51 months) in conventional group.
Preoperative mechanical alignment of the lower limb
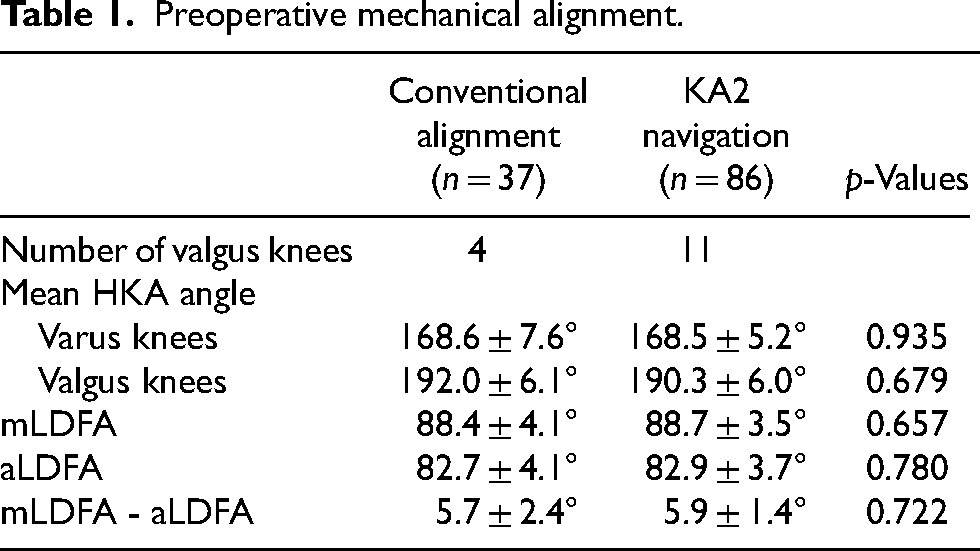
The preoperative mechanical alignments of the lower limb were comparable between the conventional alignment and KA2 navigation groups (Table 1). In the conventional alignment group of 37 cases, 4 were valgus knees; preoperatively, the mean HKA angle was 168.6 ± 7.6° for those with a varus alignment, and 192.0 ± 6.1° for those with a valgus alignment. In the KA2 navigation group of 86 cases, 11 were valgus knees; preoperatively, the mean HKA angle was 168.5 ± 5.2° for those with a varus alignment, and 190.3 ± 6.0° for those with a valgus alignment. There was no statistically significant difference of the preoperative mechanical alignments of the lower limb between the 2 groups (Table 2).
Preoperative mechanical alignment.
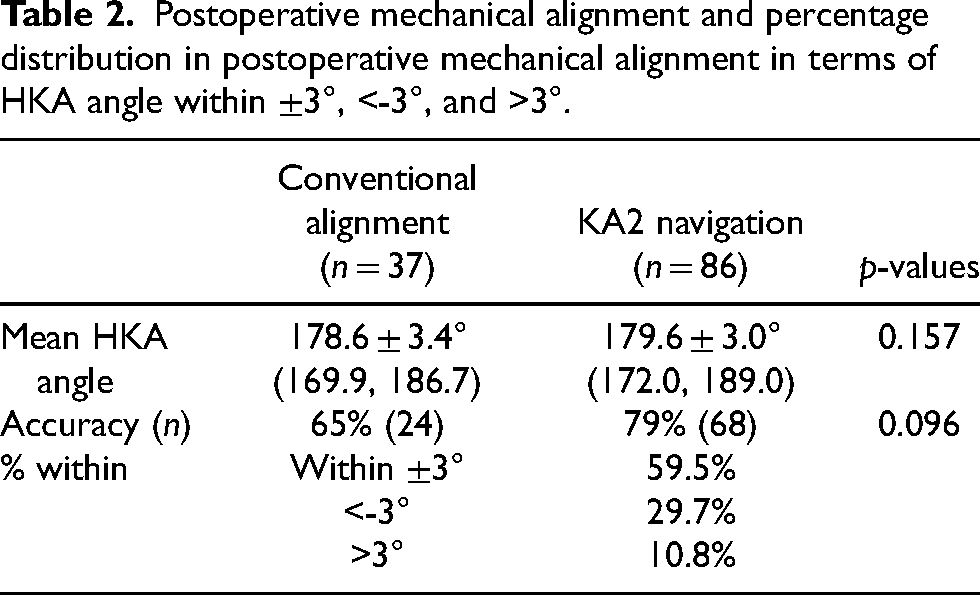
Postoperative mechanical alignment and percentage distribution in postoperative mechanical alignment in terms of HKA angle within ±3°, <-3°, and >3°.
Postoperative mechanical alignment of lower limb
The postoperative mechanical alignments of the lower limb were comparable between the conventional alignment and KA2 navigation groups (Table 3). Both the conventional alignment and KA2 navigation groups were able to achieve a neutral postoperative mechanical axis of the lower limb; the mean HKA angles of the 2 groups were respectively 178.6 ± 3.4° and 179.6 ± 3.0° (p = 0.157). Satisfactory lower limb mechanical alignment, defined as HKA angle of 180 ± 3°, was achieve in 65% (24 of 37 cases) in the conventional group, and 79% (68 of 86 cases) in the KA2 navigation group (p = 0.096). The percentage distribution of mean differences in postoperative HKA angles within ±3°, <-3°, and >3° of the two groups are shown in Figure 4.
Femoral and tibial component alignment.
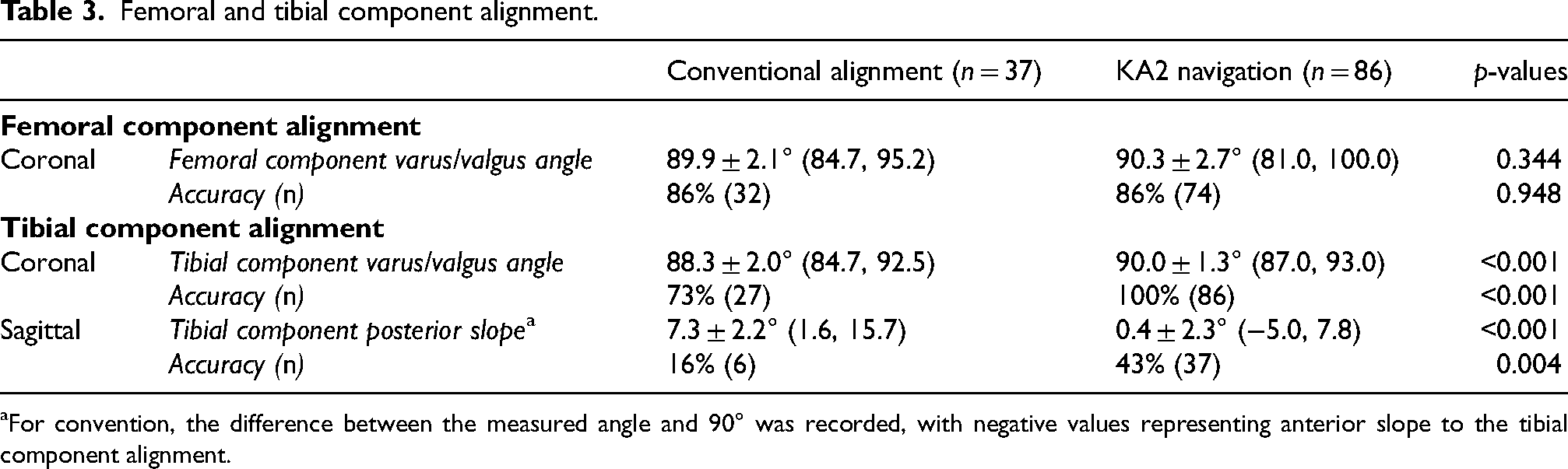
For convention, the difference between the measured angle and 90° was recorded, with negative values representing anterior slope to the tibial component alignment.
Component alignment
The KA2 navigation group's tibial component alignment in both the coronal and the sagittal planes were significantly more accurate comparing to the conventional alignment group, while there was no significant difference between the 2 groups in the femoral component alignment in the coronal plane (Table 4).
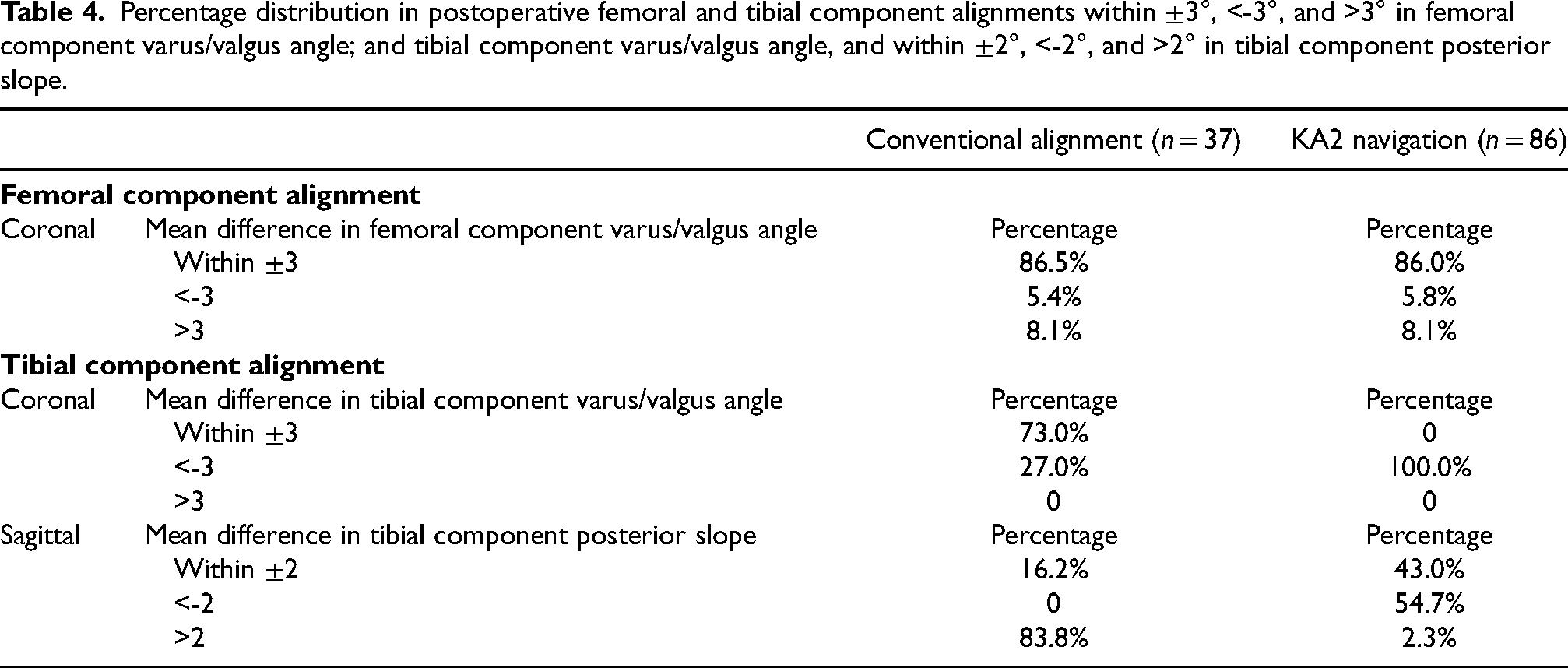
Percentage distribution in postoperative femoral and tibial component alignments within ±3°, <-3°, and >3° in femoral component varus/valgus angle; and tibial component varus/valgus angle, and within ±2°, <-2°, and >2° in tibial component posterior slope.
Coronal alignment of femoral component
The femoral component varus/valgus angle was 89.9 ± 2.1° for the conventional alignment group and 90.3 ± 2.7° for the KA2 navigation group (p = 0.344), and both means were within the accepted range used in this study for satisfactory alignment (Table 4). Satisfactory component alignment, defined as femoral component varus/valgus angle of 90 ± 3°, was achieve in 86% (32 of 37 cases) in the conventional group, and 86% (74 of 86 cases) in the KA2 navigation group; there was no significant difference between the 2 groups (p = 0.948). The percentage distribution of mean differences in postoperative femoral component varus/valgus angle within ±3 °, < -3°, and >3° of the two groups are shown in Tables 5 and 6 and Figure 5.
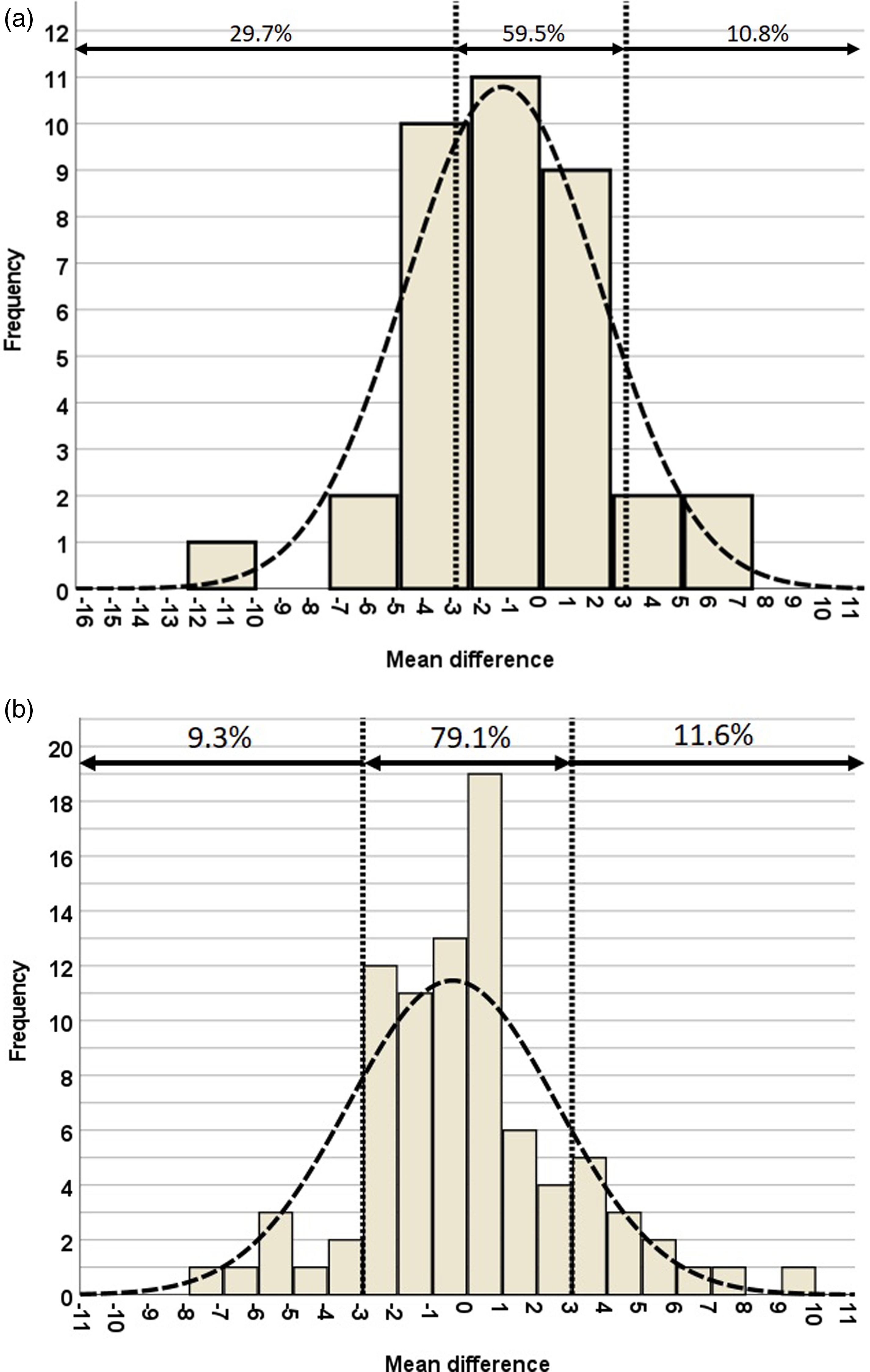
Percentage distribution of mean differences in postoperative HKA angles within ±3°, <-3°, and >3° of (a) conventional navigation and (b) KA2 navigation.
Distribution of mean differences in the three kinds of angles.
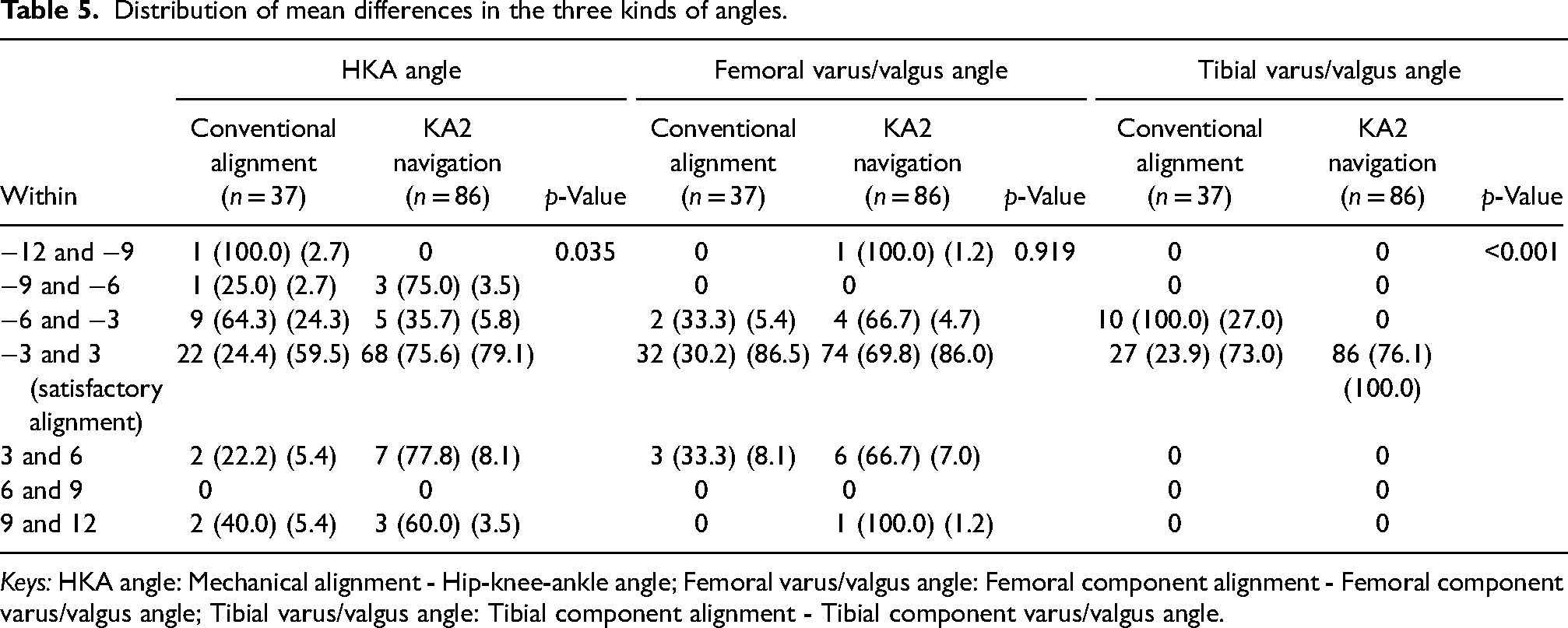
Keys: HKA angle: Mechanical alignment - Hip-knee-ankle angle; Femoral varus/valgus angle: Femoral component alignment - Femoral component varus/valgus angle; Tibial varus/valgus angle: Tibial component alignment - Tibial component varus/valgus angle.
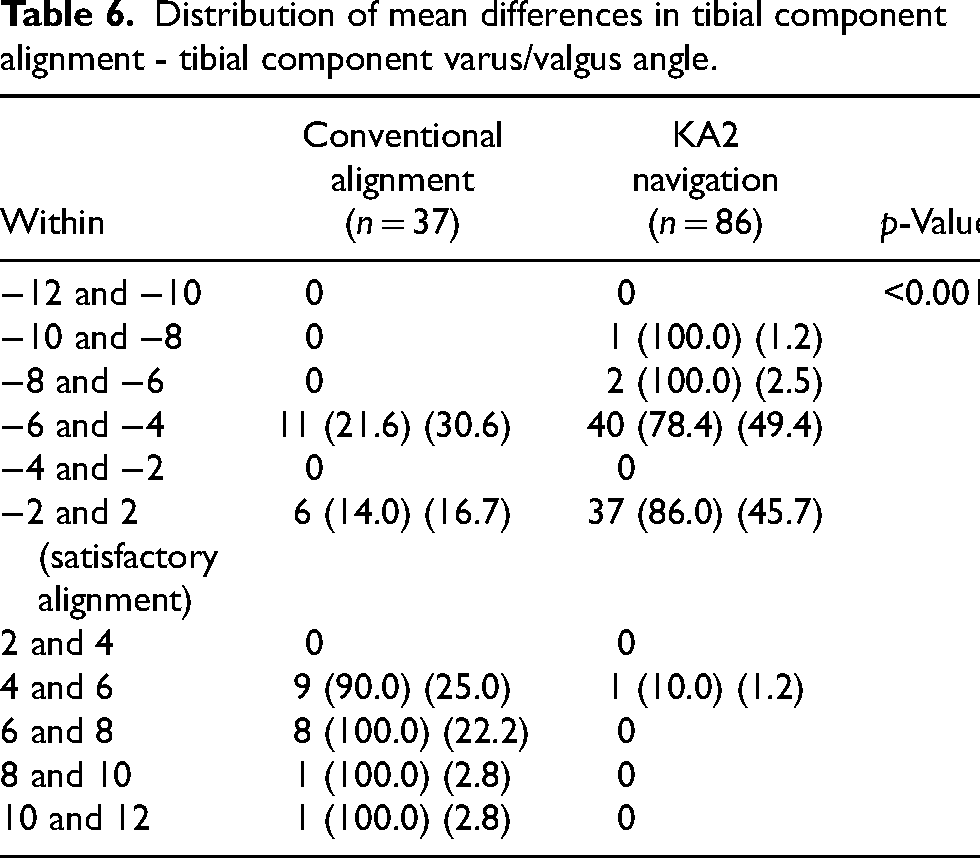
Distribution of mean differences in tibial component alignment - tibial component varus/valgus angle.
Coronal alignment of tibial component
The tibial component varus/valgus angle was 88.3 ± 2.0° for the conventional alignment group and 90.0 ± 1.3° for the KA2 navigation group; which was significantly different (p < 0.001); both means were within the accepted range used in this study for satisfactory alignment (Table 4). Satisfactory component alignment, defined as a tibial component varus/valgus angle of 90 ± 3°, was achieve in 73% (27 of 37 cases) in the conventional group, and 100% (86 of 86 cases) in the KA2 navigation group; which was significantly different (p < 0.001). The percentage distribution of mean differences in postoperative tibial component varus/valgus angle within ±3 °, < -3°, and >3° of the two groups are shown in Tables 5 and 6 and Figure 6.
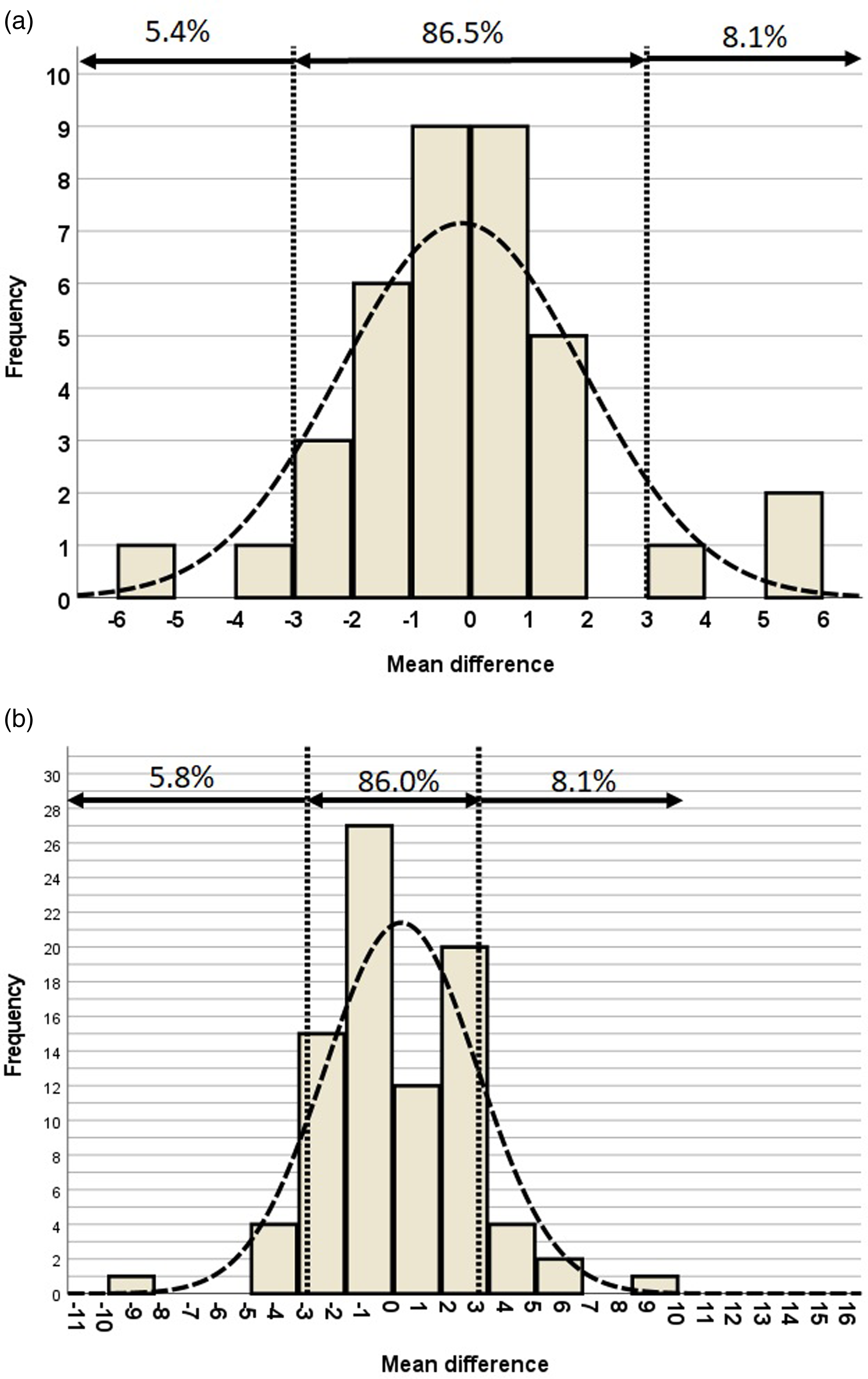
Percentage distribution of mean differences in postoperative femoral component varus/valgus angle within ±3°, <-3°, and >3° of (a) conventional navigation and (b) KA2 navigation.
Sagittal alignment (posterior slope) of tibial component
The tibial component posterior slope was 7.3 ± 2.2° for the conventional alignment group and 0.4 ± 2.3° for the KA2 navigation group, which was significantly different (p < 0.001); only the KA2 navigation group was able to achieve a mean posterior slope value within the accepted range used in this study for satisfactory alignment (Table 4). Satisfactory component alignment, defined as tibial component posterior slope of 3 ± 2°, was achieve in 16% (6 of 37 cases) in the conventional group, and 43% (37 of 86 cases) in the KA2 navigation group; there was significant difference between the 2 groups (p = 0.004). The percentage distribution of mean differences in the tibial component posterior slope within ±3°, < -3 °, and >3° and ±2°, < -2 °, and >2° of the two groups are shown in Tables 5 and 6 and Figures 7 and 8.
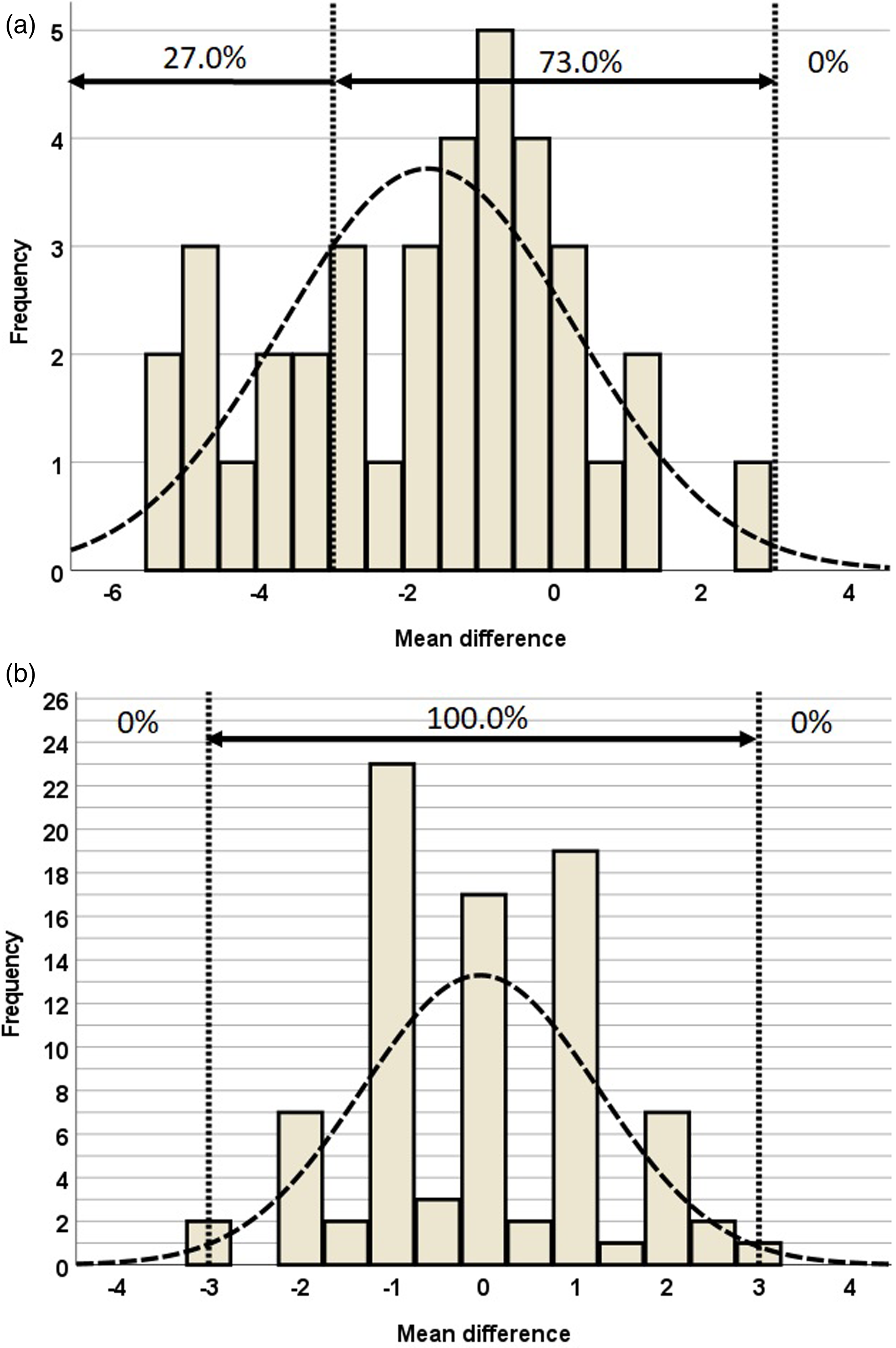
Percentage distribution of mean differences in postoperative tibial component varus/valgus angle within ±3°, <-3°, and >3° of (a) conventional navigation and (b) KA2 navigation.
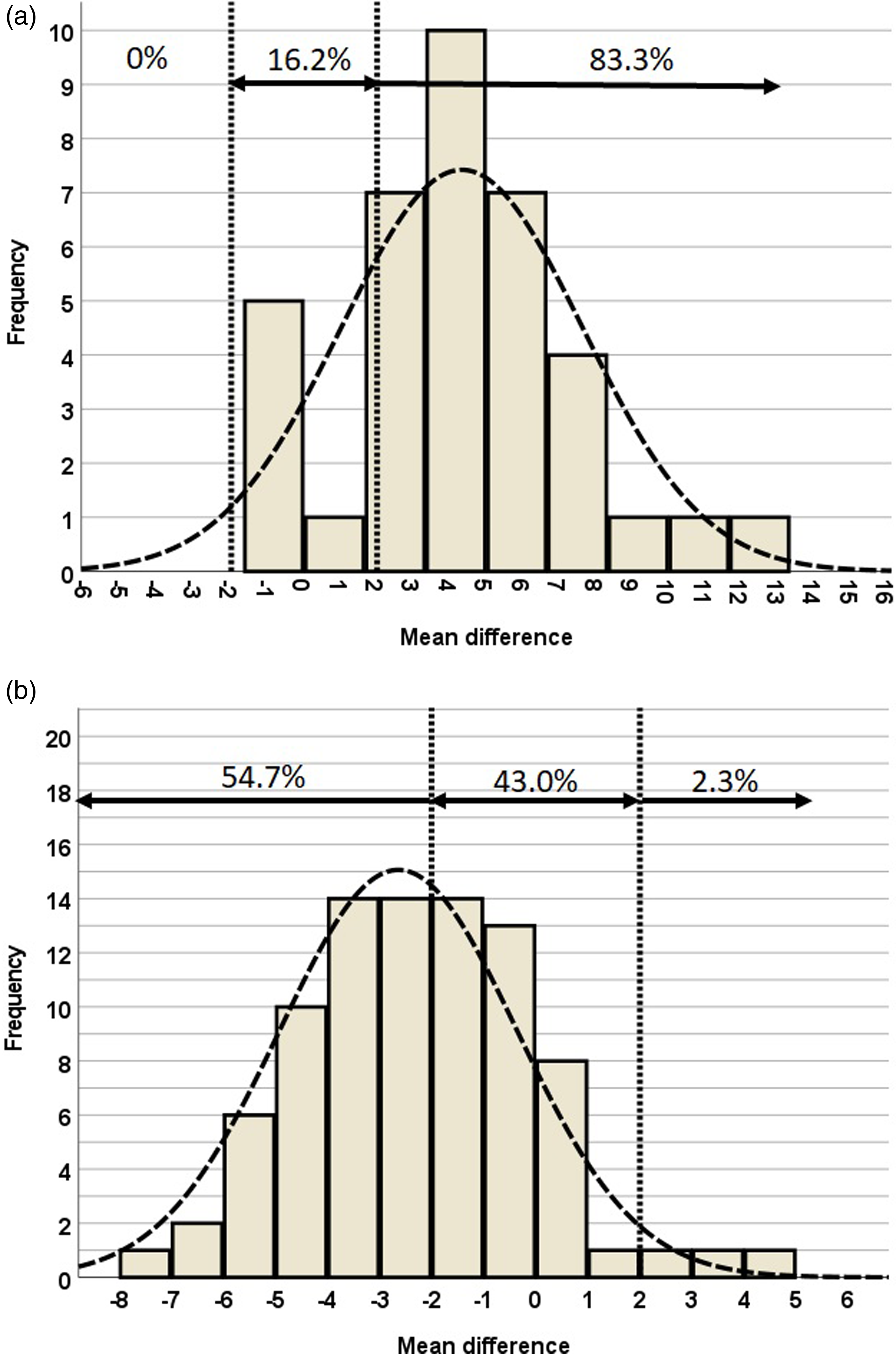
Percentage distribution of mean differences in tibial component posterior slope angle within ±2°, < -2°, and >2° of (a) conventional navigation and (b) KA2 navigation.
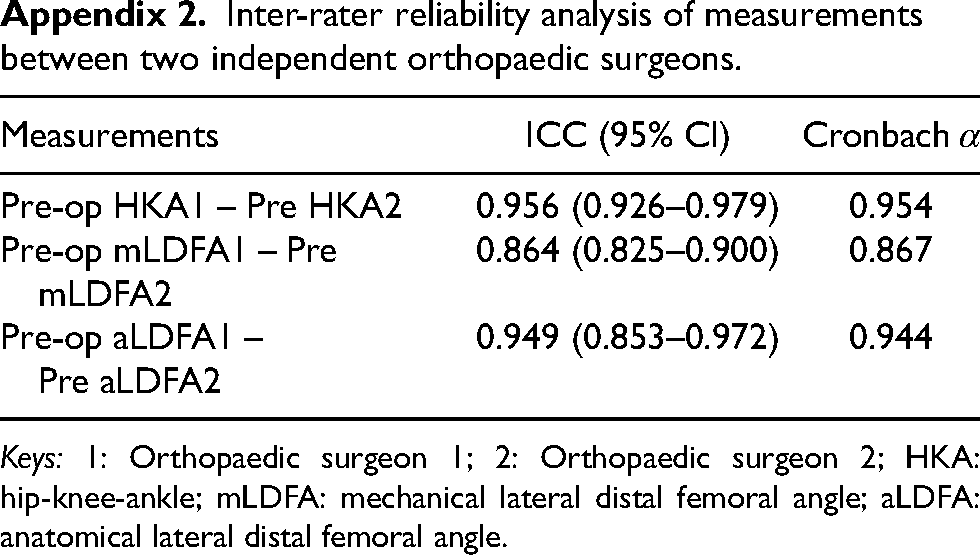
Intra-class correlation values in all measurement showed excellent reliability lowest ICC in preoperative mLDFA (ICC and 95% confidence interval [CI] = 0.875 [0.826–0.911]); highest ICC in Preoperative HKA (ICC and 95% CI = 0.979 [0.971–0.985]). The same observations were also reflected by Cronbach α values (Appendix 2).
Discussion
TKA has been a successful procedure in treatment of degenerative disease of the knee, and the optimal component placement is essential for long term implant survival. This study evaluated the radiological accuracy of ABN against conventional alignment methods, for its ability to achieve accurate component positioning in TKA in a Chinese population.
Regarding the radiological outcome evaluation of this study, while it is widely accepted that optimal coronal alignment of the femoral and tibial components should be 90 ± 3° when utilising the mechanical alignment technique, there is more controversy on the optimal posterior slope of the tibial component. We are aware that differences exist in posterior tibial slope of the native knee between different ethnic groups; Asians have increased posterior slope compared to Caucasians, 15 with Chinese having an average of 5.1° to 5.6°. 16 There are also considerable inter-individual variations,17,18 leading to the emerging concept of restoring the individual slope in TKA. Nevertheless, the purpose of this study was to determine the accuracy of ABN, and 3° of posterior slope was chosen as a reference in this study because it was the value used in the first ABN papers published, 13 and since only posterior stabilised TKR (Legion and Journey II BCS) were used in this study, excess posterior slope is not suitable.
The KA2 navigation group's tibial component alignment in both the coronal and the sagittal planes were significantly more accurate comparing to the conventional alignment group, while there was no significant difference between the two groups in the overall mechanical axis of the lower limb, or the femoral component alignment in the coronal plane.
The KA2 navigation's superiority in achieving accurate tibial component posterior slope placement may be explained by technical difficulty with the conventional EM alignment method; the fibular shaft axis is an external anatomical landmark – palpation of the fibular head and lateral malleoli can be affected by the overlying soft tissue,19,20 thereby reducing the accuracy in the subsequent proximal tibial osteotomy
ABN was introduced for clinical use in the past decade, with the first comparative studies published in 2016; it had been compared against conventional alignment methods, CAS, and PSI. Since then, numerous retrospective studies, prospective matched studies, and randomised controlled trials had been published. The two major ABN devices on the market are KA2 that were used in this study, and iASSIST (Zimmer CAS, Montreal, Canada), which uses multiple smaller accelerometer-based microelectronic pods to analyse limb position and cutting guides for alignment. 21 The latest meta-analysis by Shihab et al. (2020) 12 analysed 13 publications involving 1566 patients that compared ABN against conventional alignment method, and included of both KA2 and iASSIST. They found that the pooled odds ratios for percent outliers (taken as >3° from target) for the HKA angle (RR = 0.58) and coronal femoral angle (RR = 0.42) was significantly lower for ABN compared to conventional methods, while the coronal tibial angle, sagittal femoral angle and sagittal tibial angle were not significantly different. In addition, they found no difference in operative times, blood loss, postoperative complications, and functional outcomes in terms of Knee Society Score (KSS), Oxford Knee Score (OKS), and Short Form-36 (SF-36) scores.
The long-term benefit of ABN use in TKA, however, has yet to be demonstrated, as it had only been in clinically use since early 2010s, data concerning its long-term outcomes such as implant survivorship and functional outcomes are still pending.
It also remains uncertain if the radiological improvements conferred by ABN translate into improved clinical outcomes. Although ABN system may improve accuracy of component alignment, EM and IM alignment methods were also able to achieve satisfactory results; it is unknown if this difference would translate into improved clinical outcomes and ultimately improved implant survival in the long term – as with the experience with the CAS navigation systems,9,22–24 it may not always be the case. Further research with long term follow-up would be required to establish clinical benefit of the KA2 system.
Despite such uncertainties, navigation TKA has been demonstrated to be a valuable tool in conditions which the accuracy of conventional intra- or extra-medullary guides may be compromised, or impossible to use. Several case-series25–27 and a case-report 28 have reported success in achieving satisfactory TKA component alignments with ABN in complex cases with extra-articular deformities (e.g. post-traumatic, developmental in multiple hereditary exostoses), retained hardware (e.g. IM nail in femur, previous high tibial osteotomy), or the presence of ipsilateral total hip replacement.
The results of our current study demonstrated that KA2 confers improved accuracy in some aspects but not others; our findings suggest that the accelerometer-based KA2 navigation system is significantly more accurate than conventional methods in tibial component positioning in both the coronal and sagittal plane, however, failed to demonstrate that KA2 navigation confers any significant improvement in accuracy in achieving a neutral mechanical axis of the lower limb and femoral component placement in the coronal plane.
Limitations of this study
This study had several limitations. Only one AVN system (KneeAlign 2, OrthoAlign Inc.) was used in this study, when there are other systems available for clinical use, such as the iASSIST (Zimmer Inc.); our findings may not be able to be generalised to other ABN systems. Secondly, this was a cohort study, and randomisation was not performed; despite so, confounding variables were minimised as the demographical characteristics and preoperative mechanical alignment of the lower limb of the two groups were comparable.
Conclusions
TKA using the accelerometer-based KA2 system was found to offer a high degree of accuracy in component alignment, and in particular, significantly improved tibial component alignment in comparison with conventional alignment methods in a Chinese population. However, no significant improvements were observed in neutral mechanical axis of the lower limb alignment and femoral component placement in the coronal plane.
Footnotes
List of Abbreviations
Authors’ contributions
SLCM, MTYO, and KKWH designed the research. SLCM and XZ collected the data. WWC assembled the data. SLCM and WWC analysed, interpreted the data and wrote the paper. All authors took part in the writing and final editing of the manuscript. All authors have been given a copy of the manuscript, all have approved the final version of the manuscript, and all are prepared to take public responsibility for the work and share responsibility and accountability for the results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Inter-rater reliability analysis of measurements between two independent orthopaedic surgeons.
| Measurements | ICC (95% CI) | Cronbach α |
|---|---|---|
| Pre-op HKA1 – Pre HKA2 | 0.956 (0.926–0.979) | 0.954 |
| Pre-op mLDFA1 – Pre mLDFA2 | 0.864 (0.825–0.900) | 0.867 |
| Pre-op aLDFA1 – Pre aLDFA2 | 0.949 (0.853–0.972) | 0.944 |
Keys: 1: Orthopaedic surgeon 1; 2: Orthopaedic surgeon 2; HKA: hip-knee-ankle; mLDFA: mechanical lateral distal femoral angle; aLDFA: anatomical lateral distal femoral angle.