
Abstract
Objective
This study aims at determining the prevalence of little finger brachymesophalangia (BMP-V) in the Chinese ethnic population.
Methods
A retrospective study reviewing hand radiographs taken in United Christian Hospital from January 2011 to July 2016. Exclusion criteria included previous hand trauma, background history of genetic syndromes and non-Chinese ethnic origin. The radiographs were assessed with objective measurement using computer software and were defined BMP-V with the following criteria: (1) 5th MP length: 4th MP length <0.65 and (2) 5th MP length: 5th PP length <0.50. The radiographs would be included as BMP-V cases if they fulfil both criteria.
Results
A total of 563 hand radiographs in 394 patients (290 left hands and 273 right hands; 169 bilateral hands) were reviewed. The mean age (± standard deviation) was 51.3 ± 11.7 years (ranging from 25 to 69 years). Forty-four patients were identified to have BMP-V. The prevalence of BMP-V was found to be 11.2%. Clinodactyly with trapezoidal shape middle phalanx was found in 6.82% of the BMP-V cases. All subjects with bilateral hand radiographs showed symmetrical findings concerning the presence of BMP-V.
Conclusion
This is the first study to report the prevalence of brachymesophalangia-V in the Chinese adult population. The prevalence of BMP-V in the Chinese adult population was found to be 11.2%. It is lower than Japanese group but higher than other ethnic groups documented in other studies.
Introduction
‘Brachydactyly’ is a term derived from the ancient Greek. It refers to disproportionately short digits, which could be due to abnormally developed phalanges, metacarpals or both. Brachydactyly is one of the ten categories of hand malformations classified by Temtamy and McKusick. 1
Brachymesophalangia-V (BMP-V) is a known isolated abnormality, which is Brachydactyly type A3 according to Temtamy and McKusick classification. 1 It is the most common hereditary anomaly of the middle phalanges. It refers to the shortening of middle phalanx of the little finger. BMP-V could also present with clinodactyly, which is radial deflection of distal phalanx due to slanting of the distal articular surface of middle phalanx.
The frequency of BMP-V varied in different populations between 3.4% and 21%. 2 A study found a frequency of 21% among Japanese school children. 3 However, there is no study reporting the frequency in adult population of our locality. This study aims to report the prevalence of BMP-V in the Chinese population.
Methods
A retrospective review was performed on hand radiographs taken in United Christian Hospital from January 2011 to July 2016. Posteroanterior view of left hand, right hand or both hands is mandatory for assessment. The data were retrieved from Clinical Data and Reporting System and Clinical Management System. The exclusion criteria included previous hand trauma, background history of genetic syndromes and non-Chinese ethnic origin. The study was approved by the Research Ethics Committee of the Hospital Authority, Hong Kong.
The radiographs were assessed by an orthopaedic resident trainee and a hand specialist separately. Any discrepancy was reassessed and discussed to achieve consensus prior to analyzing the results. The radiographs were assessed with objective measurement using computer software in clinical management system radiograph viewer. The measurements were all taken along with the median axis of the shaft including both diaphysis and epiphysis. The definition of BMP-V in this study is according to the following criteria: (1) 5th MP length: 4th MP length <0.654,5 and (2) 5th MP length: 5th PP length <0.50.4–6 Both criteria have to be fulfilled for the radiographs to be included as BMP-V cases. As shown in Figure 1 is an example of radiograph, showing BMP-V.
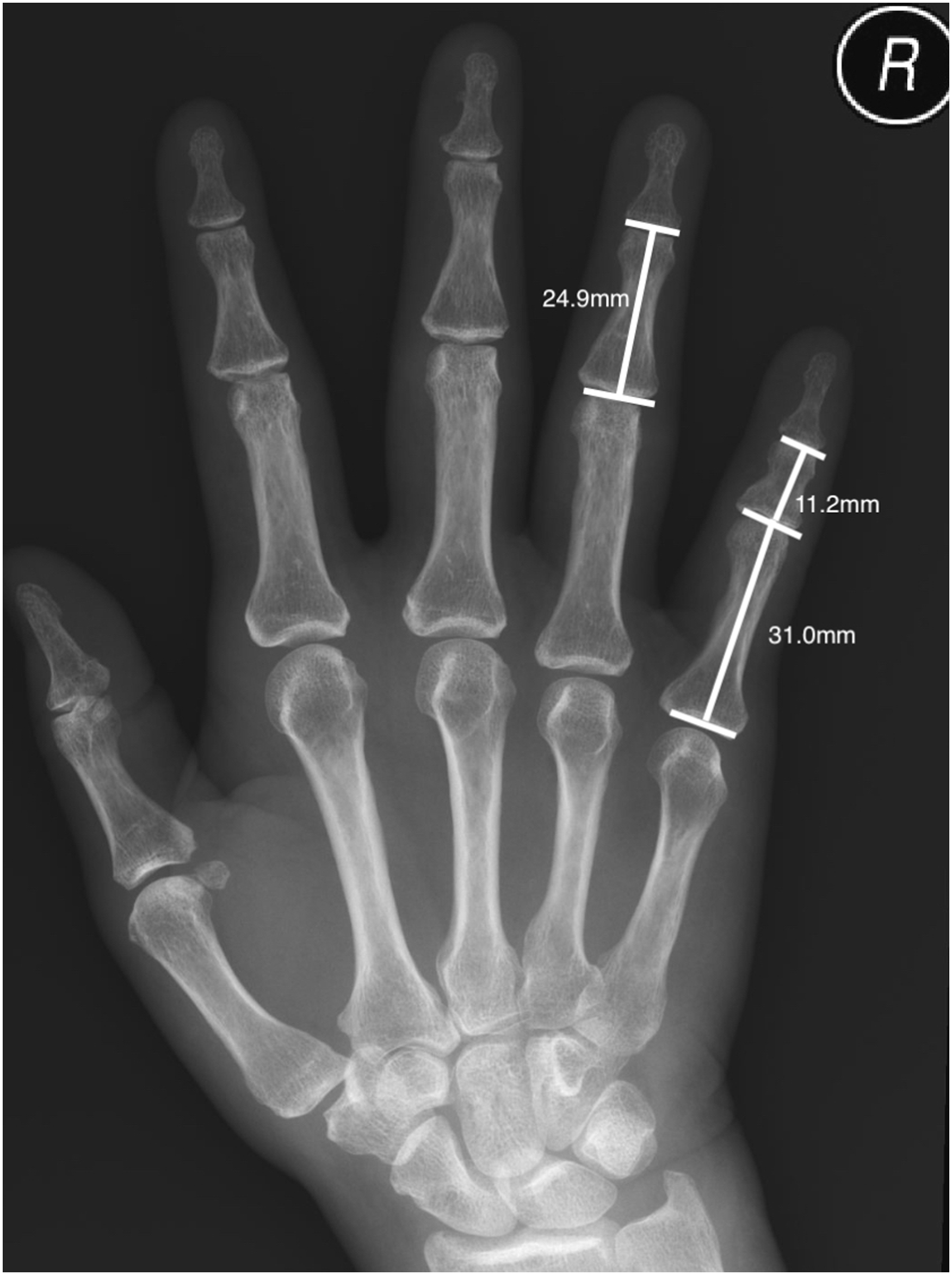
Case example of brachymesophalangia-V.
Results
A total of 563 hand radiographs in 394 patients were reviewed. There were 325 radiographs of male subjects and 238 radiographs of female subjects. There were 290 left-hand radiographs, 273 right-hand radiographs and 169 bilateral hand radiographs. The mean age (±SD) was 51.3 ± 11.7 years old (ranging from 25 to 69).
After our assessment with the computer software in clinical management system radiograph viewer, 68 radiographs of 44 patients were identified to have BMP-V, including bilateral hands (n = 24), left hands (n = 10) and right hands (n = 10). The prevalence of BMP-V was found to be 11.2% (44 out of 394 patients). The prevalence was 7.08% in male subjects’ radiographs (23 out of 325 radiographs) and 18.9% in female subjects’ radiographs (45 out of 238 radiographs).
Clinodactyly with trapezoidal shape middle phalanx was also found in 6.82% cases of BMP-V (Figure 2). In this study, clinodactyly is determined if angle of axis between distal phalanx and proximal phalanx is more than 10°.7,8 All subjects with bilateral hand radiographs showed symmetrical findings concerning the presence of BMP-V (Figure 3).
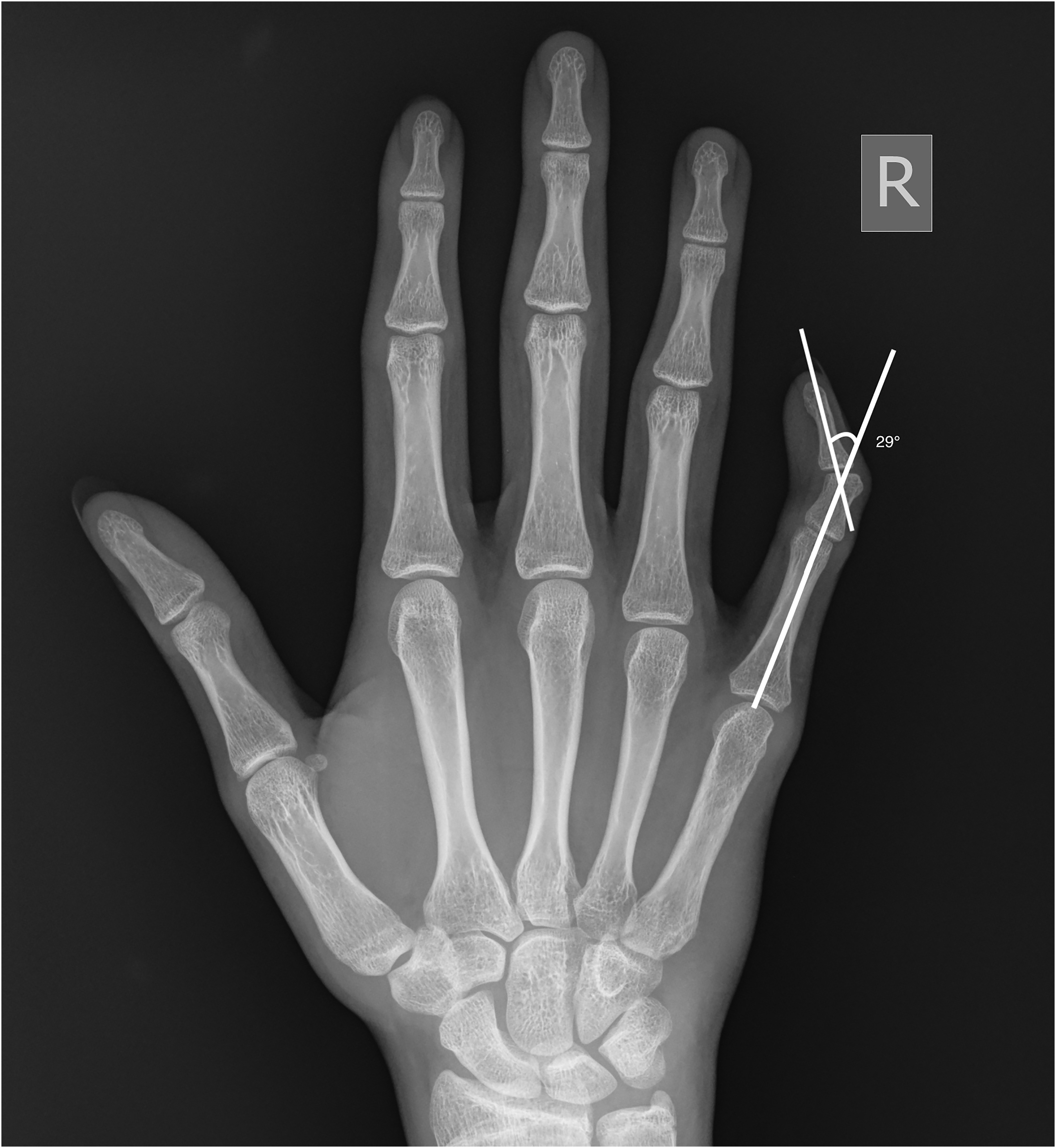
Example of clinodactyly.

Bilateral hands involvement of brachymesophalangia-V.
Discussion
This is the first study to report the prevalence of BMP-V in the Chinese adult population. The prevalence of BMP-V in our locality was found to be 11.2%. It is lower than the Japanese group, which is 21%. 3 It is higher than other ethnic groups documented1,5,9,10 (Table 1). The previous studies had different subject inclusion criteria. Japanese study by Sugiura et al. 3 included school children from 6 to 12 years old. Australian study by Brown et at. 5 and Nepalese study by Williams et al. 10 included children and young adults. Central American study by Blanco et al. 9 included malnourished children from 0 to 7 years old. These studies also had different criteria for defining BMP-V. Blanco et al. 9 took 5th MP length: 4th MP length <0.5 as defining criteria. Williams et al. 10 took into account length, width and shape of phalanges. The different subject inclusion criteria and variety of definitions hinder direct cross-study comparisons. The possible causes of such differences in prevalence could be attributed to genetics, skeletal maturity, sample size and study methodology.
Frequency of BMP-V in our study and other ethnic groups.
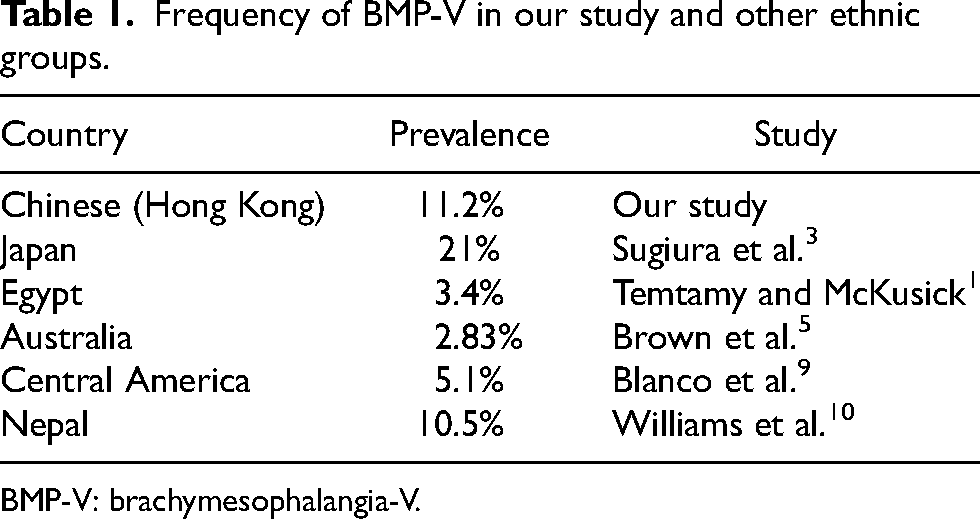
BMP-V: brachymesophalangia-V.
About 6.82% of BMP-V cases in this study also presented with clinodactyly. Clinodactyly is the slanting of distal articular surface of middle phalanx leading to radial deflection of the distal phalanx (Figure 4). Clinodactyly has different morphology, including delta and trapezoidal shape. In our study, all clinodactyly cases were trapezoidal in shape. Regarding the association of brachymesophalangia-V and clinodactyly, previous study by Roche et al. 11 reported that 90% of their cases of brachymesophalangia-V were associated with clinodactyly. However, they also reported that cases of clinodactyly could be associated with normal length of the fifth middle phalanx. This finding was verified by Temtamy et al. that clinodactyly was not always associated with a short middle phalanx and vice-versa. 12

Clinical example of clinodactyly.
The inheritance of BMP-V is autosomal dominant with reduced penetrance. 12 No gene or locus has yet been identified. Future study could aim at identifying the gene for BMP-V.
This study has strengths and limitations. Previous studies on brachymesophalangia in the Chinese population included mainly children as subjects.13,14 This was the first study reporting the prevalence of BMP-V in the Chinese adult population. Bilateral hand radiographs were utilized for analysis to observe for symmetry of BMP-V. There were two orthopaedic surgeons involved in analyzing the radiographs as independent viewers. It reduced the possibility of observation error. All radiographs were reviewed in digital data form, which could allow adjustment of contrast and magnification for more accurate measurement. Taking into account the total population aged 25–69 years old in Hong Kong, 15 it was calculated that at least 255 subjects are needed to have a confidence level of 95% and the margin of error of 5%. The sample size of this study involved a total of 563 hand radiographs in 394 patients, which was proper in assessing the prevalence in our locality.
However, there were several limitations as well. The exact ancestry of the Chinese patients involved in this study was not reported. It could lead to potential error in our results. Indications of the hand radiographs were not clearly stated in the clinical management system. There may be undocumented hand trauma, which may potentially influence the result. By far, there is no consensus on the metric methods for defining BMP-V. This study followed the criteria in the studies by Garn et al. 4 and Brown et al. 5 using both 5th MP: 4th MP ratio and 5th MP: 5th PP ratio. The ratio criteria varied in other studies.9,13 There is no general agreement on the most suitable cut-off ratios. Further study could aim at determining suitable universal criteria for defining BMP-V.
This study explored the prevalence of BMP-V in our locality. This could aid our clinical judgement when encountering patient with such anomaly. For example, in daily practice, we would encounter patient complaining of finger deformity or abnormal X-ray findings on image report. The knowledge of BMP-V could aid our diagnosis. Over-investigation could be avoided in such cases, which could reduce unnecessary clinical cost and patients’ psychological stress.
Conclusion
The prevalence of BMP-V in the Chinese adult population was determined to be 11.2%. It is lower than the Japanese group but higher than other ethnic groups documented. In subjects with bilateral hand radiographs reviewed, BMP-V was found to be symmetrical. 6.82% of the BMP-V cases also presented with clinodactyly.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.