
Abstract
Background
The number of total hip arthroplasties increases every year as the population ages. The purpose of the study was to evaluate mid-term clinical and radiological results for a minimum of two years and the survival rate at the 5-year follow-up period using a fully hydroxyapatite (HA)-coated stem.
Methods
A single-center retrospective observational study was conducted, in which 121 primary total hip arthroplasties (THA) were performed between 2013 and 2015 using a standard offset Corail fully HA-coated stem. The study included 108 patients, with a median age among all patients of 55.00 years (range 18.0–79.0 years). The median follow-up time was 4 years and 9 months.
Results
Stem survival for any reason was 98.4% at 5 years. The mean Harris Hip Score and Engh Grading Scale before surgery and at the follow-up visit show statistically significant improvement, accordingly (44.70 vs 98.13; p < 0.001) and (17.42 vs 19.68; p < 0.01). There is no statistically significant correlation between radiological and clinical results and no correlation between follow-up time and results.
Conclusions
A completely coated hydroxyapatite standard offset Corail stem shows an excellent survival rate for a 5-year follow-up. Although the radiological results are not perfect, the clinical evaluation shows that the patients are satisfied and are not limited in their daily activities as before the surgery.
Keywords
Introduction
As the population ages, the number of primary and revision total hip arthroplasties (THAs) is predicted to increase in the coming years.1–3 According to the Centre for Disease Prevention and Control (CDPC), every year more than 3000 hip replacement surgeries are performed throughout the country, and the number is expected to increase. 4 Unfortunately, aseptic loosening is one of the most prevalent causes of initial total hip arthroplasty failure, 3 and patients who have undergone revision surgery typically complain of severe discomfort, 5 and their daily activities are limited.
The cementless Corail stem (Depuy Synthes, Warsaw, IN) has been used for more than 30 years. 6 For the last decade, the Corail stem has been one of the most widely used uncemented hip components in Norway, 7 Switzerland, 8 the United States, 9 and Australia, 10 according to reports from national arthroplasty registries. The main advantage of this stem is the hydroxyapatite (HA) coating, which ensures better fixation and regular periprosthetic bone activity. 6 The most commonly used hip stem is Pinnacle as a cup.6–8 Excellent results have been achieved over medium and long-term periods.6,11
Based on promising results, a first experience study was conducted in the particular region to assess the mid-term follow-up (two to eight years) of an uncemented fully hydroxyapatite (HA)-coated stem and estimate its future use. In addition, stem survival was evaluated to assess revision rates. Furthermore, clinical and radiological results were investigated and correlation with other factors was determined to obtain a complete picture.
Methods
A single-center cross-sectional retrospective study in which 127 patients (139 hips) underwent primary total hip arthroplasty between March 2013 and December 2015. Each patient was contacted for a follow-up visit and enrollment took place over 18 months. Several exclusion criteria were applied, and the final cohort includes 108 patients (120 hips) with a response rate of 85.04% (Figure 1). Exclusion criteria include the following: 8 patients (6.30%) died during the follow-up period, 5 (3.94%) could not be reached, 4 (3.15%) declined to participate, and 2 (1.57%) underwent revision surgeries. Patients with revision surgeries were included only for survival analysis, not the clinical and radiological data analysis.
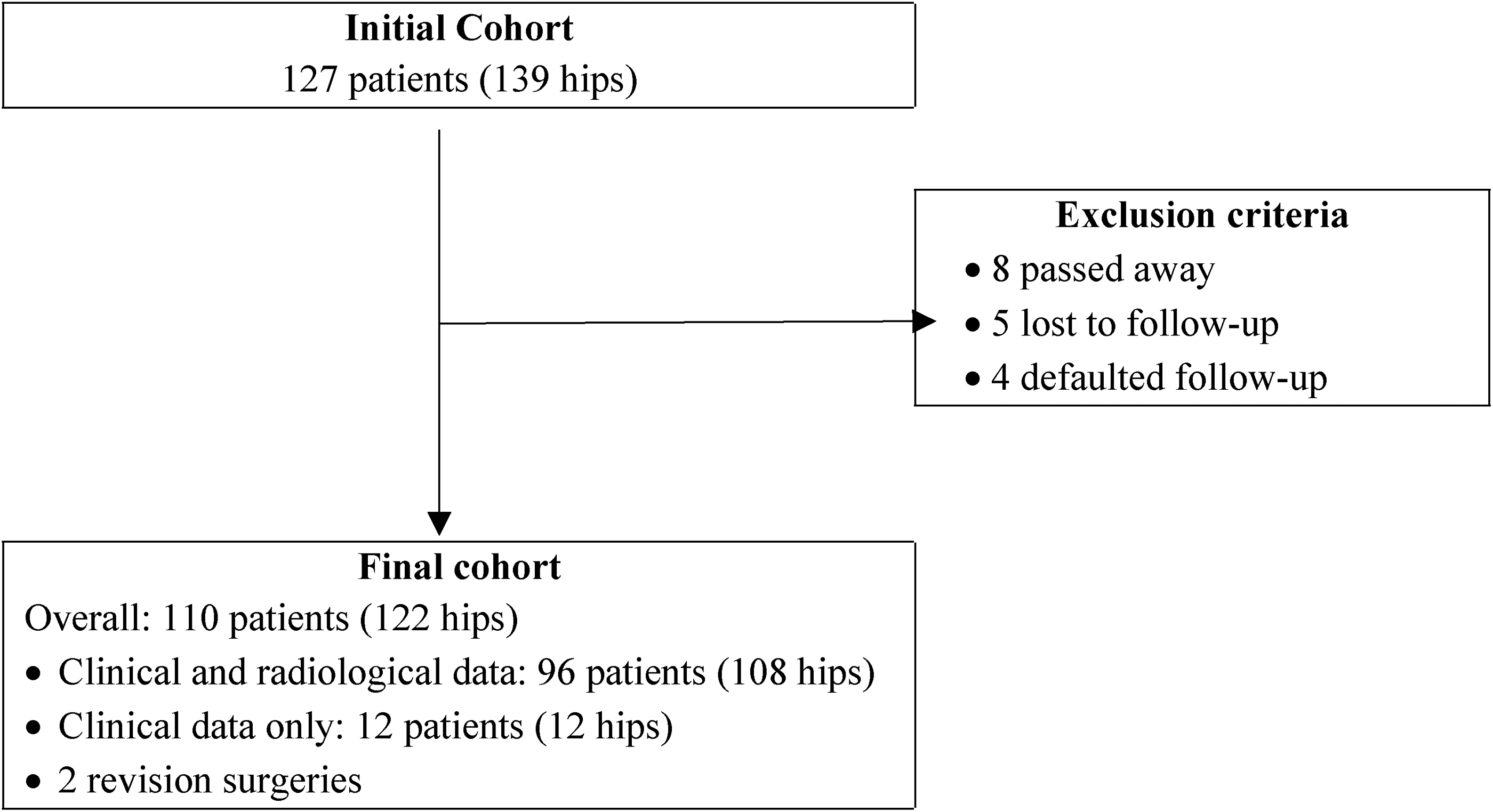
Flowchart depicting the initial cohort and final cohort.
Surgical technique and implants
Surgeries were performed by 12 surgeons specialized in arthroplasty, with the majority (42%) performed by a single surgeon. Due to the varying number of surgeries performed by each surgeon, no association was investigated between the surgeon and the outcome. The most widely used approach was the anterolateral approach (69.20%), followed by the direct anterior approach (27.50%) and the posterolateral approach (2.5%). The median surgery time was 80 min, but it is crucial to mention that several bilateral surgeries were performed in a single stage, so the surgical time increased. The median amount of blood loss was 350.00 mL.
Only one type of Corail® hip system endoprosthesis (DePuy Synthes, Warsaw, IN) was used: standard offset collarless (KS), with a neck angle of 135°. As only a collarless prosthesis was available then, no comparison could be made with the collared one. The Pinnacle acetabular cementless cup (DePuy Synthes, Warsaw, IN) was the only implanted as an acetabular component.
Clinical and radiographic evaluation
Clinically, all patients were evaluated using the Oxford Hip Score (OHS)12,13 and the Harris Hip Score (HHS). 14 HHS was used before and during the follow-up visit, but OHS was only used in the latter.
X-rays were taken twice - day two or three after surgery and at the follow-up visit. An independent radiologist examined the anteroposterior (AP) and lateral x-rays to provide radiographic evaluations using the Engh Grading Scale (EGS). It should be mentioned that the assessor was blinded. Radiographs were taken twice, the following days after total hip arthroplasty (THA), and again after a minimum of two years at a follow-up visit or in other medical centers. There were no artifacts on any of the radiographs and the prosthesis was visible throughout its length. 14 Numerous radiological indicators demonstrate the state of the surface and an ingrowth process. The presence of osteophytic zones and bony bridges was used to assess fixation. Stability was measured by evaluating radiolucency around the prosthesis, with considerable radiolucency indicating a poor prognosis.
Statistics
The data were evaluated using descriptive statistics, with the Shapiro-Wilk test being used to examine the data's standard distribution conformance.
Related samples, such as pre-operative and follow-up HHS and EGS, were analyzed with the help of the nonparametric test (Wilcoxon test). The Kruskal–Wallis test was used to determine the association between gender, age, and duration of surgery with results at the follow-up period. The Spearman correlation coefficient was determined to assess the relationship between radiological and clinical outcomes. The prosthesis survival analysis was performed using the Kaplan–Meier (KM) method, with revision of the femoral stem for any reason as the endpoint.
For all tests, the value of the P value <.05 was considered statistically significant. Statistical analysis was performed using the IBM SPSS statistical software program (version 27.0; IBM SPSS statistics for windows, Armonk, NY).
Results
Most of the patients were male (62; 51.70%) (Table 1), and the median age of all patients was 55 years. The dominant indication for surgery (98.3%) was primary osteoarthritis, followed by avascular necrosis of the femoral head (1.7%). The median follow-up time was 4 years and nine months, with a minimum period of 2 years. Most of the patients had poor pre-operative HHS (Table 2), but a convincingly high number, greater than 95%, had an excellent post-operative score, according to both OHS and HHS.
Demographic data.
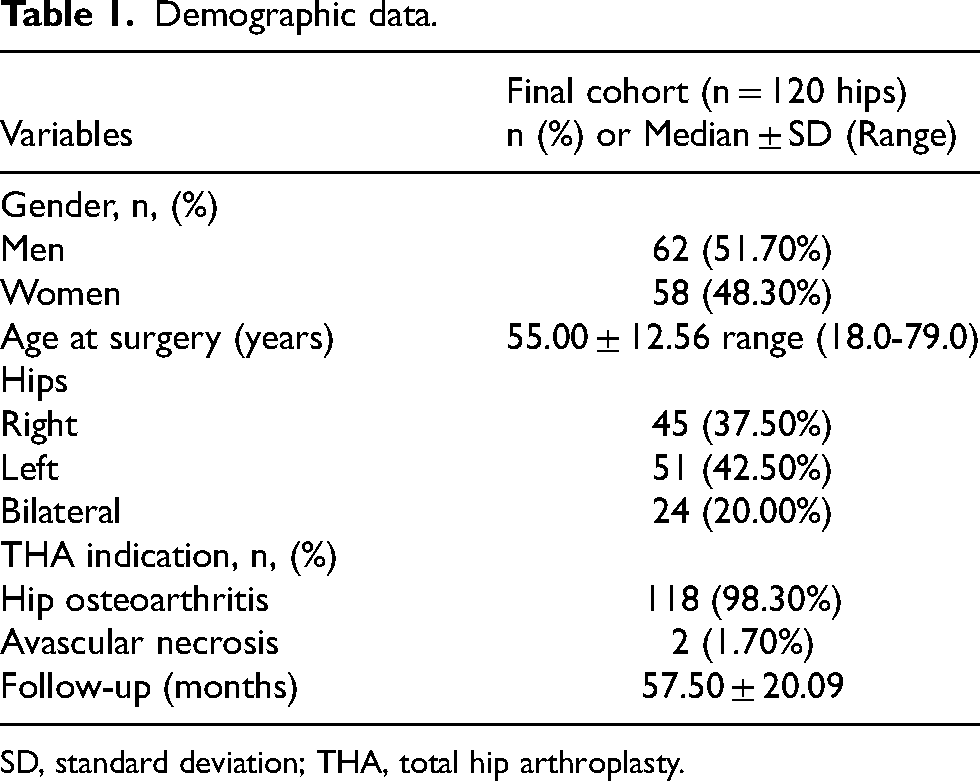
SD, standard deviation; THA, total hip arthroplasty.
Clinical results (OHS/HHS).

Taking into account that the overall rate of the stem for any reason using the Kaplan–Meier method for survival was 98.4% (95% confidence interval [CI], 95.8–99.5) at 5 years (Figure 2.). Failure of the stem has been identified in only two cases. For one patient, it accumulated 4 years and 4 months after THA due to hip pain, and the radiographic image showed a leg in the femur canal with a slight lateral localization. Another patient had a femoral periprostatic spiral fracture with dislocation 3 years and 8 months after primary THA.
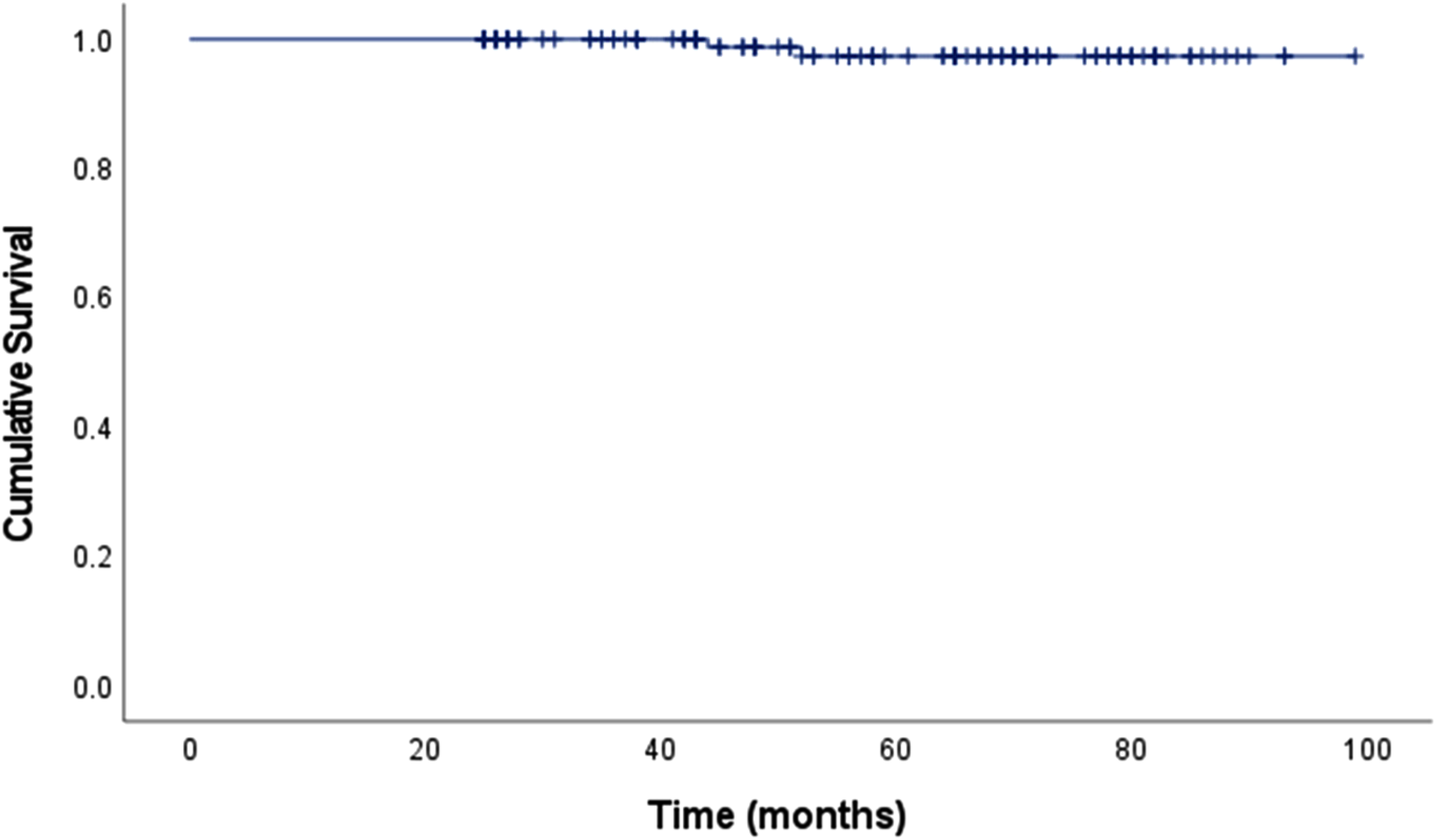
Cumulative survival by Kaplan-Meier method for the revision of femoral component for any reason.
Functional outcomes
Pre-operative HHS shows that most patients have poor functional outcomes, but the follow-up score goes in the diametrically opposite direction, as 100% of patients have an excellent outcome. The Spearman correlation showed a positive correlation between postoperative OHS and HHS, r (121) = 0.801; p < 0.001.
There is a statistically significant difference (Wilcoxon test) between HHS before (mean 44.70 ± 11.20) and after (mean 98.13 ± 2.69) surgery (p < 0.001) (Figure 3).
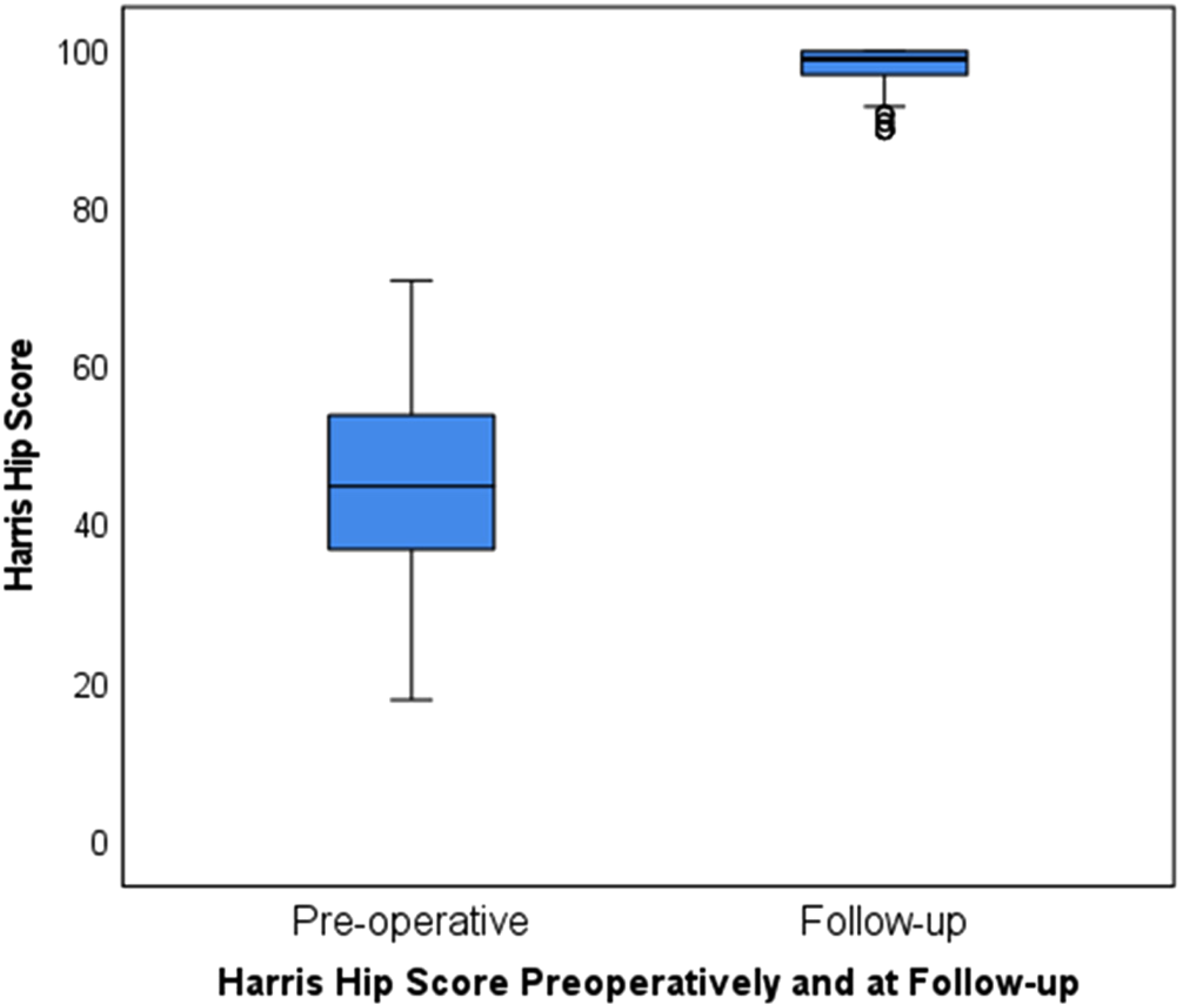
Harris hip score (HHS) before surgery and at a follow-up visit.
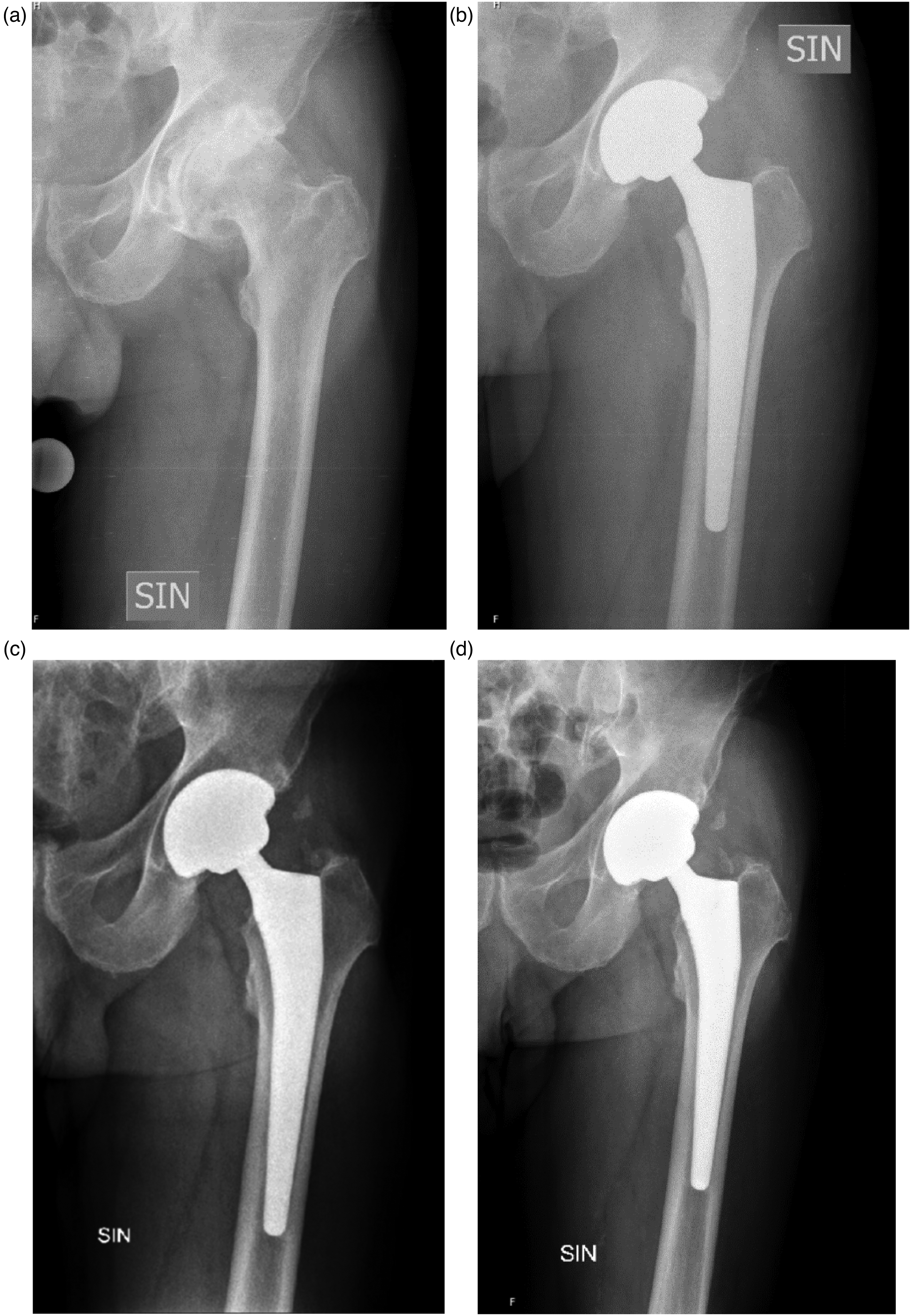
(a) Pre-operative radiograph showed severe osteoarthritis in the year 2013. (b) Radiograph taken postoperatively, three days after the surgery, showing only slight fixation but maximal stability. (c) Radiograph 4 years after the surgery. (d) Radiograph after seven years, showing the fixation at its maximum and good stability.
The mean OHS was 46.92 ± 2.060 (range, 37–48). When analyzing OHS, all elements are above the 3.80 score. The highest pain score at night, where the mean is (3.98, SD, 0.156), walking (3.97; SD, 0.180), and independent shopping (3.97; SD, 0.180). The lowest score was for socks (3.79; SD, 0.451) and pain in the hip (3.83; SD, 0.460).
Using the Kruskal Wallis test, there was no statistically significant difference between the postoperative HHS score and the patient's gender, age, duration of surgery, stem size, or follow-up time. Concerning OHS, an identical resemblance is seen.
Radiographical outcome
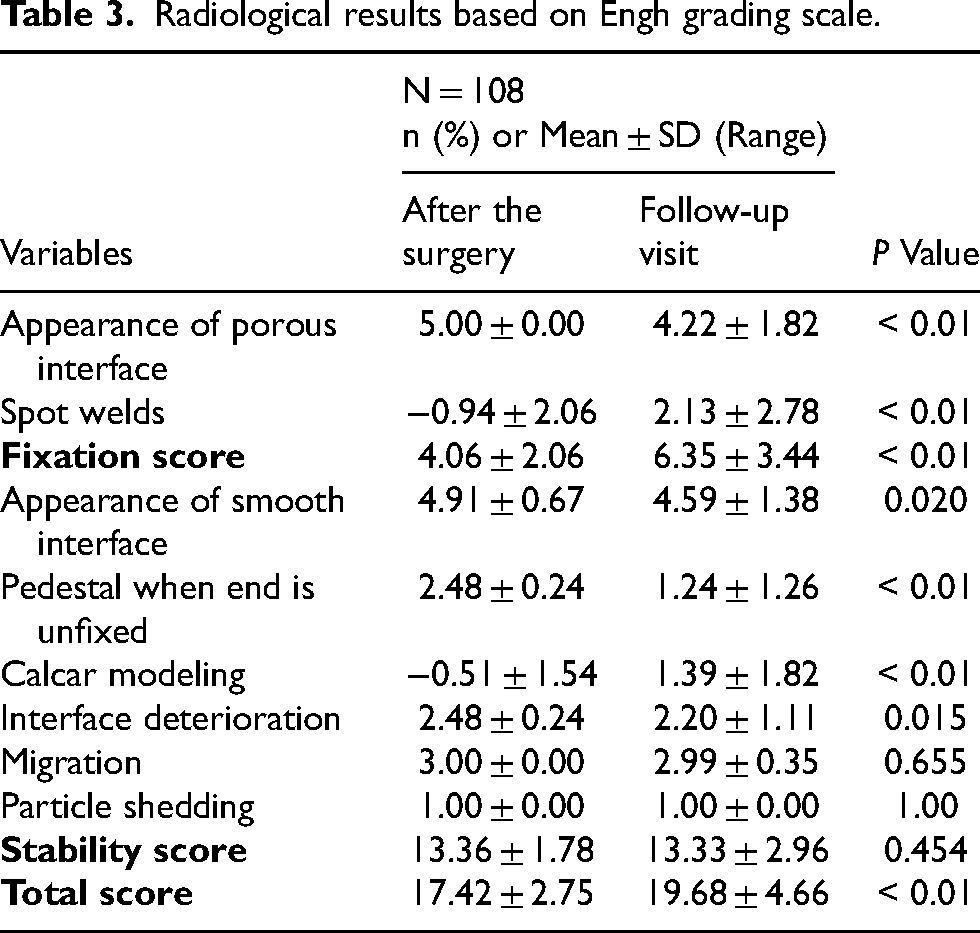
The Wilcoxon test analyzed two related samples. Statistical difference was observed between fixation right after surgery and at the follow-up visit (<0.001), and overall EGS overall (p < 0.001) was observed, but no differences between stability (p = 0.454) and overall score.
When evaluated by EGS (Table 3), all elements must be evaluated together, and some of them, such as the presence of a pedestal and the mild appearance of the porous surface (p < 0.01), show a negative score in the results. Therefore, the average total score of the x-rays after surgery was 17.42 ± 2.75, but at the follow-up visit, 19.68 ± 4.66 (p < 0.01), confirming the good osteointegration and stability of the prosthesis in dynamics.
Radiological results based on Engh grading scale.
The Spearman correlation did not show a statistically significant association between the time of follow-up and EGS (p = 0.892) and HHS (p = 0.611). Regarding the correlation between radiological and clinical results, the Spearman correlation shows no correlation between EGS and postoperative HHS r (109) = 0.111; p = 0.249.
Discussion
Survival
It is undoubtedly only beneficial as only two revision surgeries were performed with a survival rate of 98.40%, but it was impossible to analyze the factors that could influence the outcome. Our results for mid-term survival are in line with other studies; for example, in Switzerland, the 5-year survival rate is 96.8%, 8 while in Australia, 96.9%. 10 When the survival bar increases to ten years, survival varies between 95.0%-98.8%.10,11,15,16 Furthermore, extensive studies, such as a report from the Norwegian Registry of Arthroplasty with 28,928 standard collarless Corail stems, show 97.6% survival over a 10-year period, without stem revision for all causes of standard collarless stem. 7 After 20 years, the survival rate is above 96% 6 but decreases to 93.7% after 26 years of mean follow-up 17 and 88.4% for any non-infectious cause with up to 30 years of follow-up. 7 Especially the HA-coating could be beneficial in these promising results, as a femur stem with HA-coating had a 17% lower risk of revision for any reason than stems without HA-coating. 18 Aseptic loosening and periprosthetic fracture are often the main reasons for revision surgery,7,17 which is consistent with our study.
Clinical and radiological results
In a similar study with a mean follow-up period of eight years, the results align with our research – low stem revision rate and statistically significant in OHS and HHS. 19 A good correlation between OHS and HHS is observed, 12 but OHS benefits by reducing clinical time and expense during follow-up, therefore being more accessible in clinical practice. As in the present study, pre-operative OHS is not always obtained. 12 Patients can interpret the question based on their perspective and perception of hip function, which can vary due to the dynamic nature of pain and daily activities performed, and it can be difficult to distinguish symptoms of the afflicted hip from other comorbidities. 20 Furthermore, numerous patients revealed at follow-up appointments that they have discomfort in the other hip or have other comorbidities, making it challenging to differentiate directly from the operated hip.
Approaches associated with a higher risk of stem revision were anterior approaches (direct anterior and anterolateral) compared to the posterior approach. 7 A recent survey by the American Association of Hip and Knee Surgeons (AAHKS) shows that the most commonly used approaches for primary THA were posterior and direct anterior, accounting for more than 90% of cases, 21 which is contrary to the study findings, where the preference is for the anterolateral approach.
Although other authors indicate that the risks of stem revision increase by being male gender, being older than 70 years, having a small stem size (8–11) compared to medium ones (12–15), and having a non-osteoarthritis diagnosis, 7 our study did not find such a correlation. The clinical results could be evaluated as excellent, as they are also higher than in other studies,16,17 but it should be noted that there was also a longer follow-up period. In the present study, no statistically significant correlation was found between clinical and radiological results, so it should not be assumed that a patient with an x-ray outside the perfect score has any complaints or will need revision surgery in the following years.
The EGS is a reliable scale to use when reviewing radiographs, 22 and doing it by one person makes the review process more consistent.15,22 Therefore, radiographs play an essential role in the prognosis of stability of THA. It should not be forgotten that other factors could influence the outcome; for example, bone mineral density (BMD) can significantly affect EGS and be a significant predictor of prosthesis instability. 14 However, EGS is still not used in radiologists’ daily reports; therefore, some essential features, such as the pedestal sign, can be underestimated. There are no statistically significant differences in overall OHS for patients with or without significant radiolucent lines, 15 as observed in our study, where the clinical and radiological results did not correlate significantly.
The main strength was the high response rate of the patients. Furthermore, an independent radiologist who joined the study team only in the final stage of the study performed a radiological evaluation, making it more objective. However, despite excellent results, several limitations have been identified: a relatively small number of records and no control group to compare, lowering the precision of statistical analysis. Also, the uneven distribution of the follow-up period does not allow for the evaluation of the result. As other authors indicate, the better results were obtained for collared stems than for collarless ones, as standard collared stems had a lower risk of revision, 7 but only collarless stems were available in the hospital at the exact time so no comparison could be made between collarless and collared stems. As was also mentioned in our study, not all patients are evaluated clinically and radiographically, 23 but the Covid-19 situation also limited the options for patients to complete follow-up visits. Body mass index (BMI) is used to compare results between patients 17 but was not included in the study.
To conclude, a HA-coated standard offset Corail stem demonstrates good clinical results and excellent survival for initial THA treatment. Not only does having a low rate of revision surgeries allow patients to live painlessly and return to their daily activities, which is one of the main concerns for patients when having options for surgical or conservative treatment. This article supports previous studies and warrants the use of the particular stem. In future, the study will continue to evaluate long-term results in a further way and compared to the collared stem.
Footnotes
Acknowledgements
The authors would like to thank the Hospital of Traumatology and Orthopedics for helping with the data collection.
Author’ contributions
All authors participated in the conception and design of the research. Material preparation, data collection and analysis were performed by Pēteris Studers, Dārta Jakovicka, Jana Solska, Una Bladiko, Maija Radziņa. The first draft of the manuscript was written by Dārta Jakovicka and Pēteris Studers and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) state that they did not receive any funding, grants, or other support during the preparation of this manuscript.
Ethics approval
This study was carried out according to the principles of the Declaration of Helsinki. This study was approved by the Research Ethics Committee of Riga Stradins University and the Hospital of Traumatology and Orthopedics.
Consent to participate
Informed consent was obtained from all individual participants included in the study.