
Abstract
Background
The primary purpose of this study is to evaluate the long-term survivorship of medial open wedge high tibial osteotomy. The secondary purpose is to review the clinical outcome and surgical challenges during conversion knee arthroplasty.
Methodology
The patients with medial open wedge high tibial osteotomy performed from 1995 to 2019 were reviewed. The survivorship, surgical particulars and clinical outcomes of the conversion arthroplasty were reviewed.
Results
There were 61 medial open wedge high tibial osteotomy performed from 1995 to 2019. The overall 10-year survival rate of medial open wedge high tibial osteotomy is 83.7%. In total, 22 medial open wedge high tibial osteotomy required conversion arthroplasty and none of them required revision in the study period. The patients who required conversion arthroplasty had higher mean posterior tibial slope than those who did not require it (14.5° vs 11.6°; p = 0.047). In total, 52.3% required quadriceps snip for exposure, 14.3% need a tibial stemmed component and 9.5% need a constrained total knee replacement. There was statistically significant improvement in Knee Society knee score, functional score, and range of motion after the conversion arthroplasty.
Conclusion
The 10-year survival rate of medial open wedge high tibial osteotomy is satisfactory. The patients who required conversion arthroplasty had higher mean posterior tibial slope. In conversion cases, with careful pre-operative planning, most of them can be converted to conventional total knee replacement. The range of movement and functional scores significantly improved after conversion arthroplasty. Also, patellar baja or not does not predict the need for quadriceps snip during conversion arthroplasty.
Introduction
Osteoarthritis of the knee has become a major global health issue. Operative treatment is indicated in advanced knee osteoarthritis which affects the daily lives of patients. Apart from total knee replacement (TKR), there are other operative choices for unicompartmental knee osteoarthritis and varus knee deformity, including unicompartmental knee replacement (UKR) and high tibial osteotomy (HTO). Early studies showed that varus knee alignment was more commonly found in Chinese compared to other populations. 1
HTO is a common treatment for medial compartment osteoarthritis of knee, especially for those with varus knee deformity. 2 The aim of HTO is to overcorrect the knee mechanical axis and redistribute the load between the medial and lateral compartments of knee. It is more preferable in young patients with high functional demand, as it preserves the patients’ natural joint surfaces and allows subsequent conversion to TKR. There are different types of HTO including medial open wedge HTO (MOWHTO), dome shape HTO and lateral close wedge HTO. In our centre, MOWHTO is the most commonly performed type. Therefore, our study will focus on the outcome of MOWHTO.
Studies suggested that patients undergoing HTO had good short-term and intermediate-term functional outcomes. 3 However, they deteriorated after time and required conversion TKR or UKR. 4 This can be due to over-correction, under-correction or loss of correction of the alignment.
On the other hand, post-HTO conversion TKR faces several surgical challenges. Previous HTO causes difficulties in skin incision, surgical exposure, and bone cut etc. 5 We would like to review the surgical challenges, clinical, and outcomes of the conversion arthroplasty.
The primary aim of this study is to evaluate the long-term survivorship of MOWHTO in a local joint replacement centre, using conversion arthroplasty as end-point. Since the culture, activity level, bone morphology of Asian is different from Caucasian, local study reviewing the outcome of MOWHTO can allow surgeons and patient to consider the risk and benefits of this procedure. Lau et al. 6 published a study reviewing the survival of MOWHTO in a teaching hospital, which is the first study reviewing local long-term results in Hong Kong. Our study aimed at reporting the results of MOWHTO in a local joint replacement centre. We would like to identify any risk factor affecting the survival of HTO. The secondary aim is to review the surgical challenges and clinical outcome of conversion arthroplasty.
Methodology
This study has been granted approval from local research ethics committee on 5 June 2020. No identifiable patient's information is disclosed in the study; thus, consent was waived.
Selection criteria
Patients with HTO performed in a single centre from 1995 to 2019 were traced retrospectively. Patients underwent MOWHTO due to osteoarthritis and varus deformity were selected. Patient underwent other types of tibial osteotomy, including dome shape HTO and lateral close wedge HTO was excluded because only few of them were performed over the years. Other patients who underwent non-HTO for post-traumatic deformity and low tibial osteotomy for congenital deformity in paediatric patients were ruled out from the patient group.
Medial open wedge high tibial osteotomy
The indications for HTO included young or middle age and active adults with varus knee deformity and early-stage knee osteoarthritis. Contra-indications include severe bicompartmental or tricompartmental osteoarthritis (Kellgren and Lawrence grade 3 or above), inflammatory arthritis, significant knee contracture and advanced age above 65. The commonest type of HTO performed in our centre was MOWHTO.
MOWHTO was performed in uniplanar fashion. Pre-operative planning was done with Miniaci method on lower limb alignment film. The planned post-operative mechanical axis should be neutral or slightly overcorrect by passing through the Fujisawa point. The tibial bone cut was started medially at 3–4 cm below medial joint line, directed proximally towards fibula head, aiming at about 1 cm below lateral plateau. Intra-operatively, gradual opening of osteotomy was performed with verification by the cable method. Care was taken to avoid fracturing the lateral hinge. MOWHTO were fixed externally with Ilizarov fixator; or internally with Tomofix plate or Puddu plate in our centre, using bone substitute or autograft from iliac crest to fill the bone void.
Patient's gender, age, implant, use of autograft or bone substitute were reviewed. Peri-operative complications were reviewed from medical records. Standing long radiographs showing hip to ankle of bilateral lower limbs at pre-operative, post-operative and latest follow-up were reviewed to measure the lower limb alignment. Pre-operative and post-operative posterior lateral knee films were reviewed to measure the posterior tibial slope. The posterior tibial slope was measured on the lateral knee radiograph with reference to the proximal tibial anatomical axis, which is defined as the line joining the midpoints of the tibial shaft at 5 and 15 cm distal to the joint line (Figure 1). Another line is drawn along the tibial plateau. The posterior tibial slope angle was measured between the two lines. 7
Conversion arthroplasty
The surgical details of the conversion arthroplasty operation were studied, including the type of implant used, operative time and surgical approach. Due to previous knee surgery and scar formation, in cases with difficult soft tissue exposure, quadriceps snip was used. In cases with significant laxity or deformity, TKR with a tibial stem or condylar-constrained implant was used.
In terms of clinical performance, the knee society knee score, functional score and range of motion (ROM) were reviewed at pre-conversion arthroplasty and 1-year post-conversion arthroplasty. The pre-conversion lower limb alignment films and lateral knee radiographs were reviewed. The lower limb alignment was measured with standing long radiographs showing hip to ankle of bilateral lower limbs. The patellar height was measured with Insall-Salvati ratio and Caton-Deschamps index from the lateral knee radiographs. The posterior tibial slope was also measured on the lateral knee radiograph.
Data analysis
Non-parametric data were analyzed with Wilcoxon signed-rank test. Risk factors of early failure were analysed with cox regression test. Survival of the HTO was measured with conversion arthroplasty as endpoint. It was measured with Kaplan–Meier Method. All statistics were analyzed by using Statistical Package for Social Sciences version 20.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
102 cases were identified using “tibial osteotomy” as keyword from 1995 to 2019. After ruling out the dome shape HTO, lateral close wedge HTO, non-HTO cases, there were 61 medial open-wedge HTOs in 42 patients performed HTO in our centre from 1995 to 2019. Among these patients, 19 patients performed MOWHTOs on both knees, while 23 patients performed MOWHTO on a single knee. There were 22 male patients and 20 female patients. The mean age undergoing MOWHTO was 53.2 ± 5.1.
35 of 42 patients came back for regular follow-up, resulting in a patient follow-up rate of 83.3%. 3 patients defaulted follow-up throughout the years and 4 patients passed away during the follow-up period. The mean post-op follow-up period is 12.4 ± 6.0 years, with a range from 4 to 22 years. Follow rate at 5-year, 10-year and 15-year are 90.7%, 75.9%, and 50%, respectively.
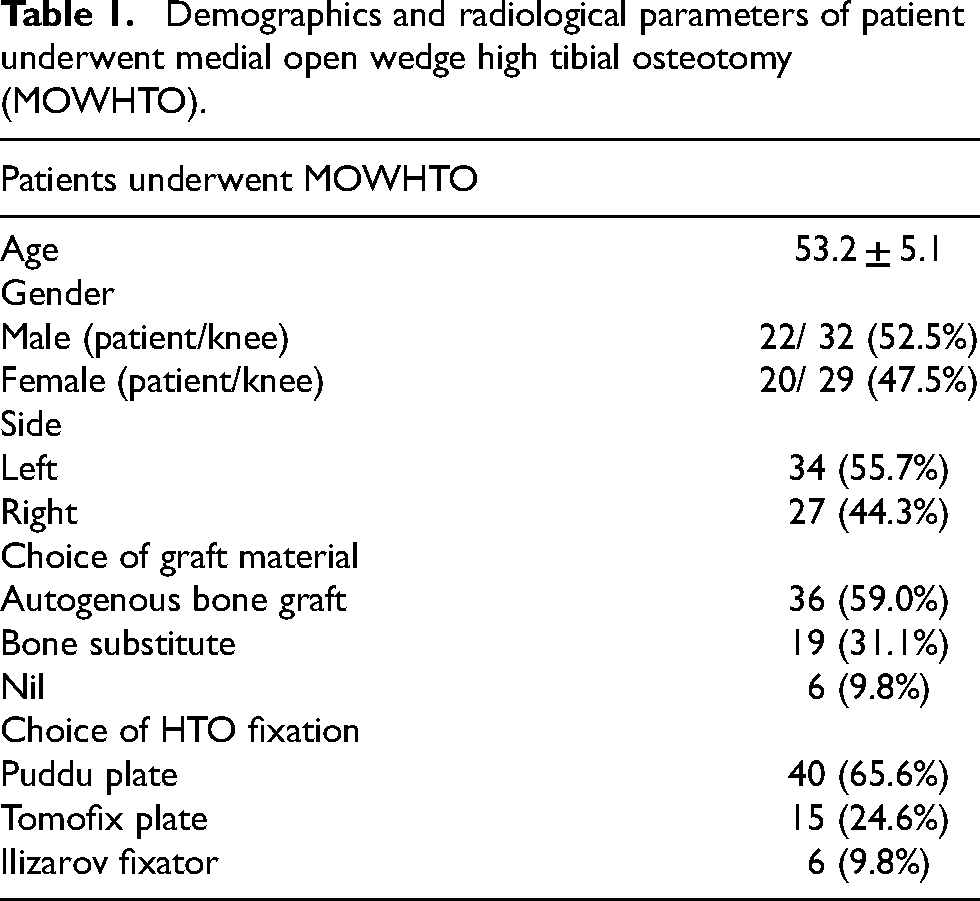
The MOWHTO are fixed with different methods. 40 of them were fixed with Puddu plates, 15 of them were fixed with Tomofix plates and 6 of them were fixed with Ilizarov fixators. Autogenous bone graft was used in 36 knees, bone substitute was used in 19 knees while no graft material was used in 6 knees (Table 1).
Demographics and radiological parameters of patient underwent medial open wedge high tibial osteotomy (MOWHTO).
Survivorship analysis
In total, 22 out of 61 HTOs required conversion arthroplasty. The conversion was performed at a mean of 11 ± 5 years after HTO. Using Kaplan Meier analysis, the 5-year and 10-year survival rates of MOWHTO were 91.4% and 83.7%, respectively (Figures 2 and 3). The mean survival of MOWHTO was 17.0 years, 95% confidence interval 15.1–18.9 years.
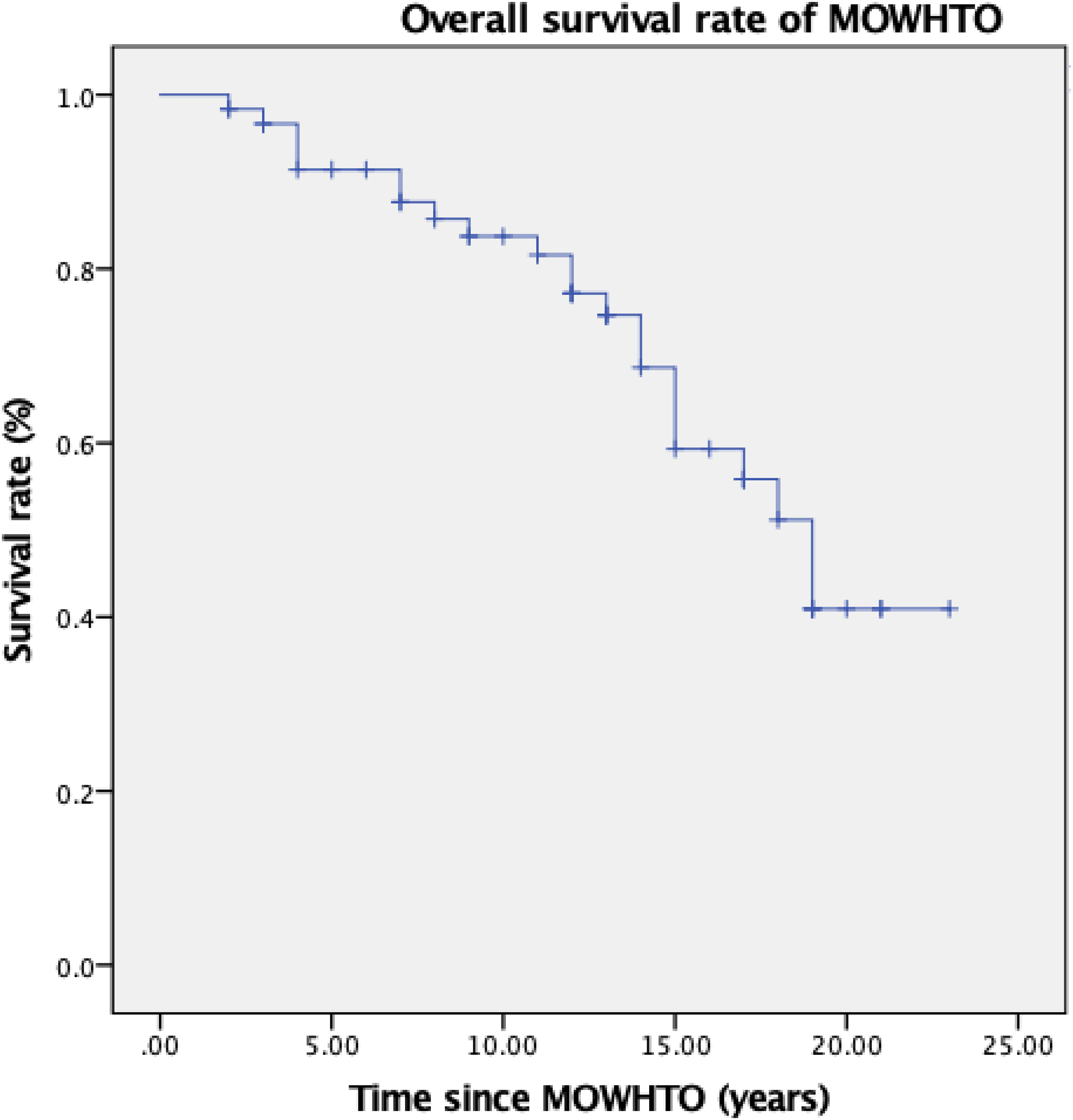
22 of 61 high tibial osteotomies (HTOs) required conversion. The conversion was performed at a mean of 11 ± 5 years after HTO. The 5-year and 10-year survival rates of HTO were 91.4% and 83.7% respectively.
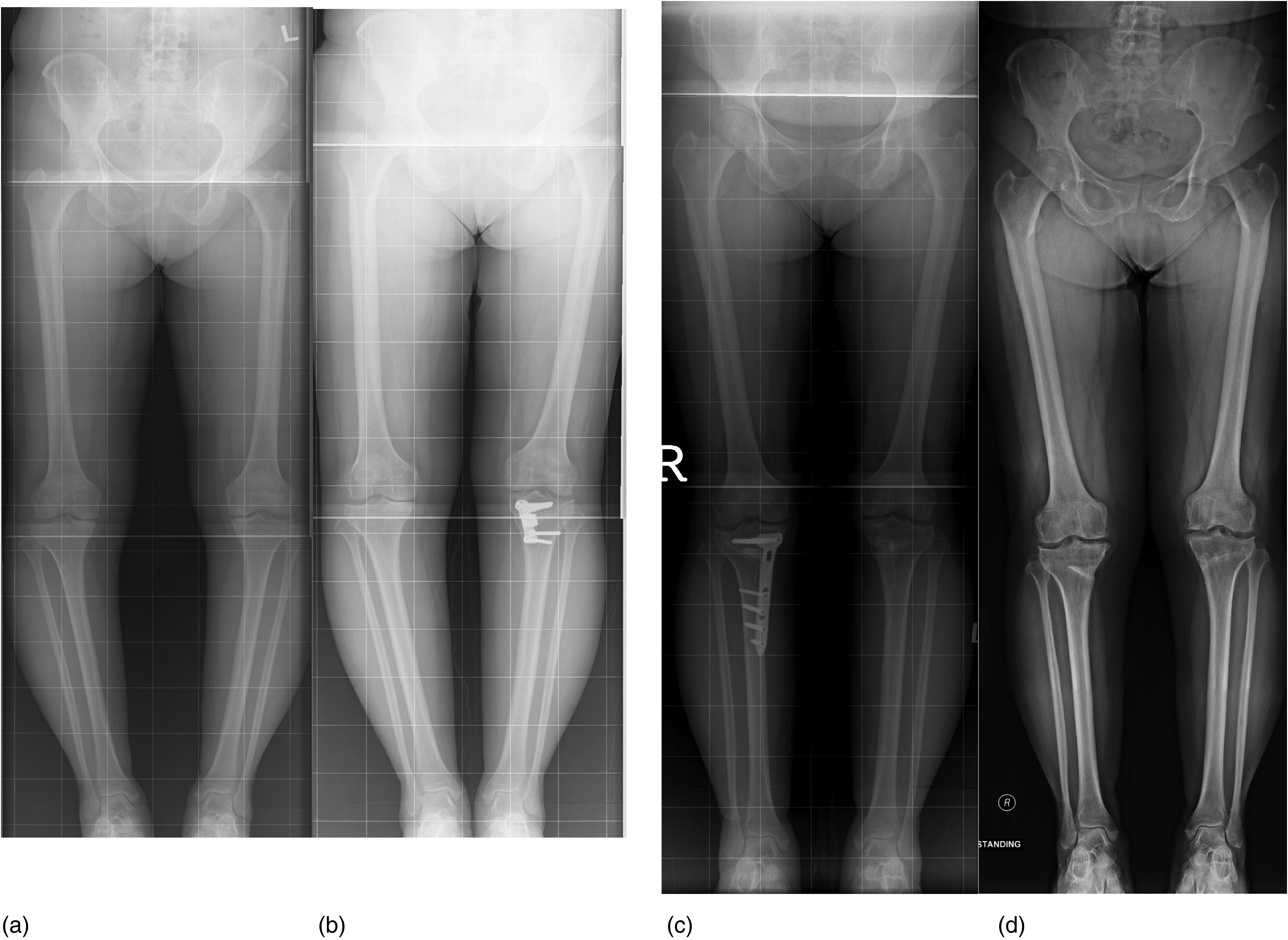
Varus deformity of 9° and 11° of left and right knees respectively (a) were corrected to neutral alignment (b and c). Long film taken 11 years post-operative showed 2° varus over right knee and neutral alignment over left knee. (d).
Pre-operative, post-operative and latest follow-up knee alignment
Standing anteroposterior radiographs showing patients’ bilateral lower limbs were taken before MOWHTO, early post-operative follow-up and at latest follow-up. However, some of the patients’ radiographs were not available due to loss of old records. The lower limb alignment was taken as hip-knee-ankle angle, by drawing the mechanical axis from hip centre through knee to ankle centre. 33 of the HTOs had pre-operative lower limb alignment films with mean lower limb alignment of −9.76 ± 3.72° (taking negative as varus alignment). In total, 48 of the HTOs had early post-operative lower limb alignment films with mean lower limb alignment of −0.02 ± 5.4°. In toral, 53 of the HTOs had the latest follow-up lower limb alignment films with mean lower limb alignment of −1.62 ± 6.3°. There is a significant correction of varus deformity after medial opening HTO with analysis using Wilcoxon signed-rank test (p < 0.001). (Table 2)
Radiological parameters of patient underwent medial open wedge high tibial osteotomy (MOWHTO).
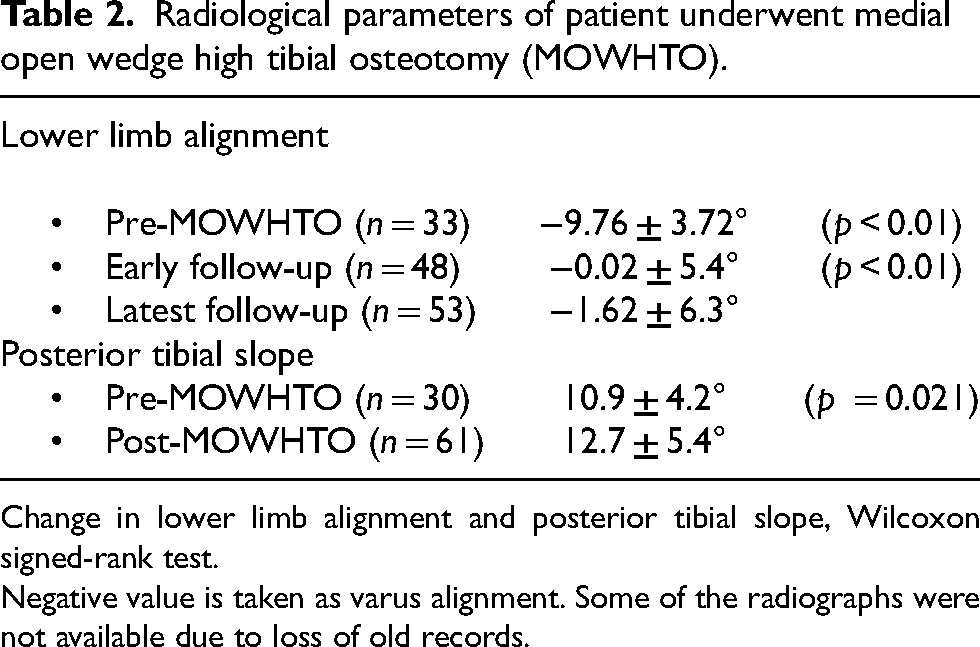
Change in lower limb alignment and posterior tibial slope, Wilcoxon signed-rank test.
Negative value is taken as varus alignment. Some of the radiographs were not available due to loss of old records.
30 of the HTOs had pre-operative lateral knee films with a mean posterior tibial slope of 10.9 ± 4.2°. All of the 61 HTOs had post-operative lateral knee films with a mean posterior tibial slope of 12.7 ± 5.4°. There is a significant increase in posterior tibial slope after MOWHTO with analysis using Wilcoxon signed-rank test (p = 0.021). (Table 2) The mean posterior tibial slope in MOWHTO requiring conversion arthroplasty and those did not require conversion were 14.5 ± 5.70° and 11.6 ± 5.05° respectively (p = 0.047).
Post-operative complications
There were 14 complications in the 61 MOWHTO (23.0%). There were 10 superficial infections, 2 delayed bony union, 1 broken implant and 1 iatrogenic tibial plateau fracture. There was no peroneal nerve injury.
Conversion arthroplasty
There were 21 conversions TKR and 1 conversion UKR. The mean operative time was 146 ± 27.6 min. Conversion TKR was performed in patients with a progression of osteoarthritic changes and knee pain after MOWHTO. While the patient underwent conversion UKR has under-correction of varus deformity and persistent medial knee joint pain (Tables 3 and 4).
Demographic data of patients underwent conversion arthroplasty.
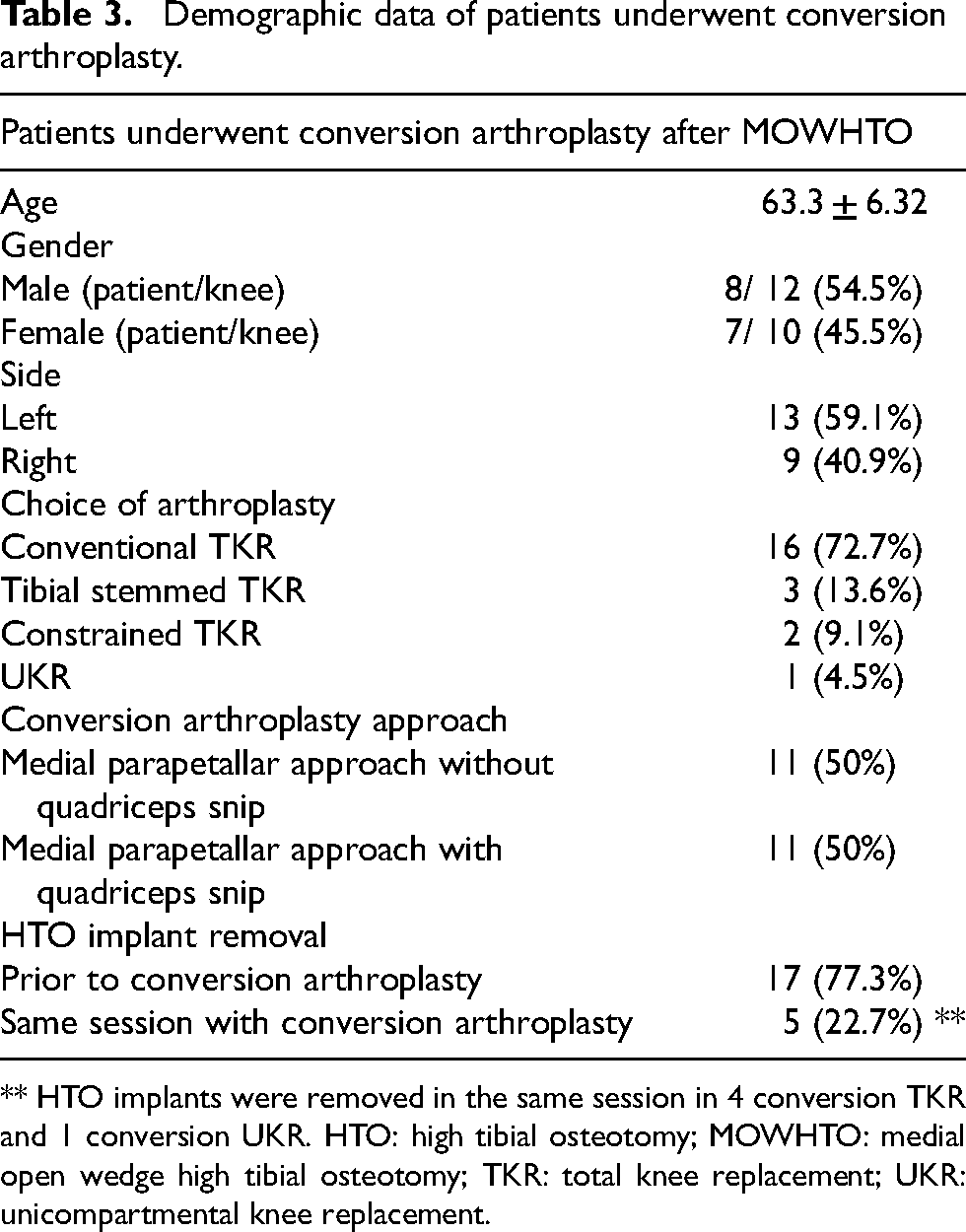
** HTO implants were removed in the same session in 4 conversion TKR and 1 conversion UKR. HTO: high tibial osteotomy; MOWHTO: medial open wedge high tibial osteotomy; TKR: total knee replacement; UKR: unicompartmental knee replacement.
Pre-conversion MOWHTO radiographic parameters (n = 22).
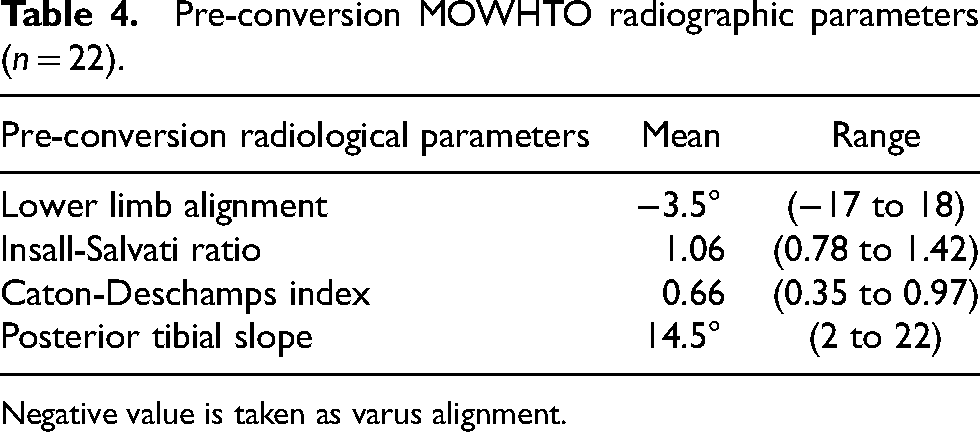
Negative value is taken as varus alignment.
All the conversion arthroplasties were performed with a medial parapatellar approach, incorporating the previous incision for HTO. In knees with difficult patellar eversion, quadriceps snip was used. In total, 11 conversions (50%) require quadriceps snip, while 11 conversions (50%) can be performed with conventional medial parapatellar approach. Although we have more than half of the cases with difficulty in exposure, the mean Insall-Salvati ratio of the pre-conversion knee is 1.06 ± 0.22° and only one knee had patellar baja with a ratio of 0.78; while the mean Caton-Deschamps index was 0.66 and 7 knees had patellar baja with index less than 0.6. The mean Caton-Deschemps index in knees requiring quadriceps snip and not are 0.62 and 0.71 respectively, with no significant difference between the 2 groups (p = 0.15).
Amongst the 21 conversion TKR, 4 knees (19.0%) had their HTO implants removal in the same operation, with the rest of 17 knees (81.0%) knees had their implants removed in a prior surgery. Tibial stemmed component was used in 3 conversion TKR (14.3%). Two of them required a tibial stem because they had the removal of previous HTO implant in the same operation as the conversion TKR (Figure 4). The other case had a severe varus deformity of 17° and medial tibial bone loss, thus requiring a tibial stem and metal wedge but a constrained implant was not necessary. Two TKR conversions (9.5%) required condylar-constrained implant due to over-correction with severe valgus knee alignment of 14 and 18° respectively (Figure 5). For the rest of the cases, a conventional posterior-stabilized TKR was implanted.
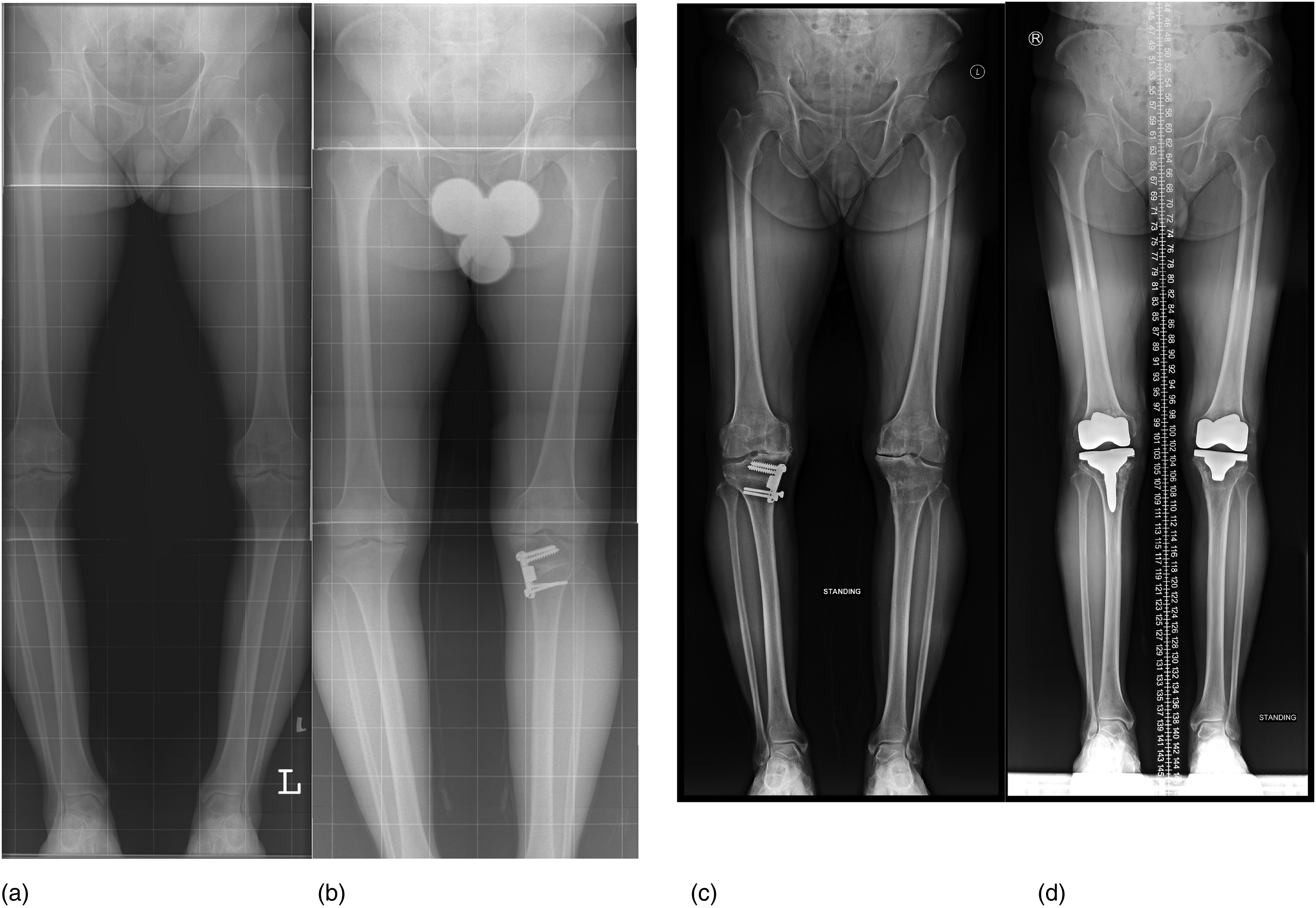
Varus deformity of 14° and 10° of left and right knee respectively (a) were corrected to neutral alignment after MOWHTO. (b and c) Right conversion TKR with tibial stemmed implant; left conversion TKR with conventional posterior stabilized implant were performed. MOWHTO: medial open wedge high tibial osteotomy; TKR: total knee replacement.

Over corrected left knee alignment 18° valgus after MOWHTO. (a) Condylar constrained TKR was performed to increase knee stability in coronal plane 14 years after MOWHTO. (b). MOWHTO: medial open wedge high tibial osteotomy; TKR: total knee replacement.
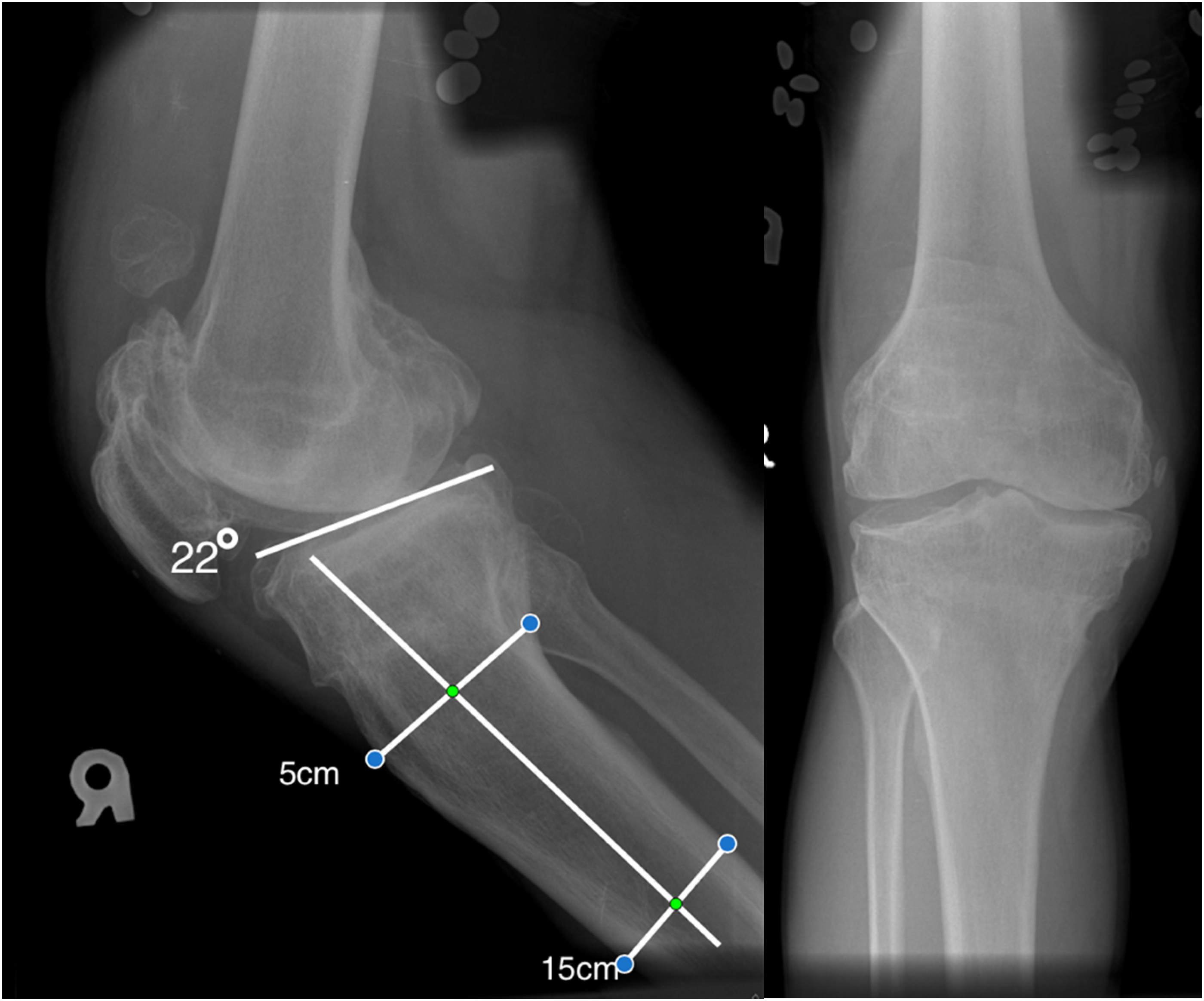
Patient with post medial open wedge high tibial osteotomy (MOWHTO) posterior tibial slope of 22°. This patient underwent conversion arthroplasty 11 years after MOWHTO.
The mean lower limb alignment of pre-conversion knee is −3.5 ± 8.55° (taking negative as varus alignment). There was statistically significant improvement in the average knee score, functional score and ROM after conversion arthroplasty. The mean pre-conversion knee score was 53.7 ± 14.7 while post-conversion knee score was 83.2 ± 10.0 (p < 0.001). The mean pre-conversion functional score was 51.4 ± 19.0 while post-conversion functional score was 61.6 ± 23.6 (p = 0.007). The mean pre-conversion ROM was 84.5 ± 22.6, while post-conversion ROM was 99.3 ± 12.1 (p = 0.005) (Table 5).
Conversion arthroplasty functional score and radiological parameters (n = 22).
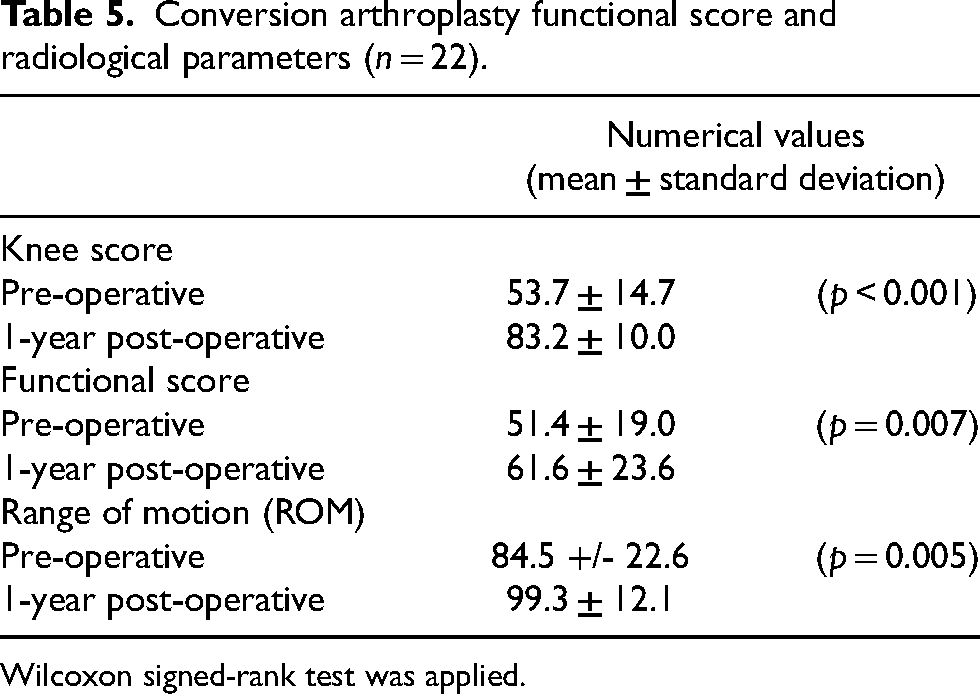
Wilcoxon signed-rank test was applied.
Risk factors affecting the HTO survival rate
The effect of patients’ age, gender, implant used, post-operative posterior tibial slope, pre-operative and post-operative lower limb alignment on MOWHTO survival rate, using conversion arthroplasty as endpoint, were analyzed with cox-regression model. For categorical paraments, patients with bone substitute inserted were compared to autograft. Patients undergoing surgery at older than 50-year-old were compared to 50-year-old or below. Male patients were compared to female patients. Pre-operative lower limb alignment with 10° varus or below were compared to more than 10° varus. Post-operative lower limb alignment 5° varus or below were compared to more than 5° varus. Patients with Puddu plate inserted were compared to other fixation (Tomofix plate or external fixator). For continuous variable, the effect of posterior tibial slope on survival was directly analysed.
The hazard ratio of the high post-operative posterior tibial slope was 1.08 (95% CI: 1.00–1.17) (p = 0.039), which suggested a high posterior tibial slope associated with poorer survival of the MOWHTO (Table 6). Although the results were statistically significant, the hazard ratio is close to 1, which may not suggest a significant risk of early conversion arthroplasty. Other parameters have no significant effect on the survival rate of HTO.
Cox regression model to identify independent risk factors of HTO survival rate.
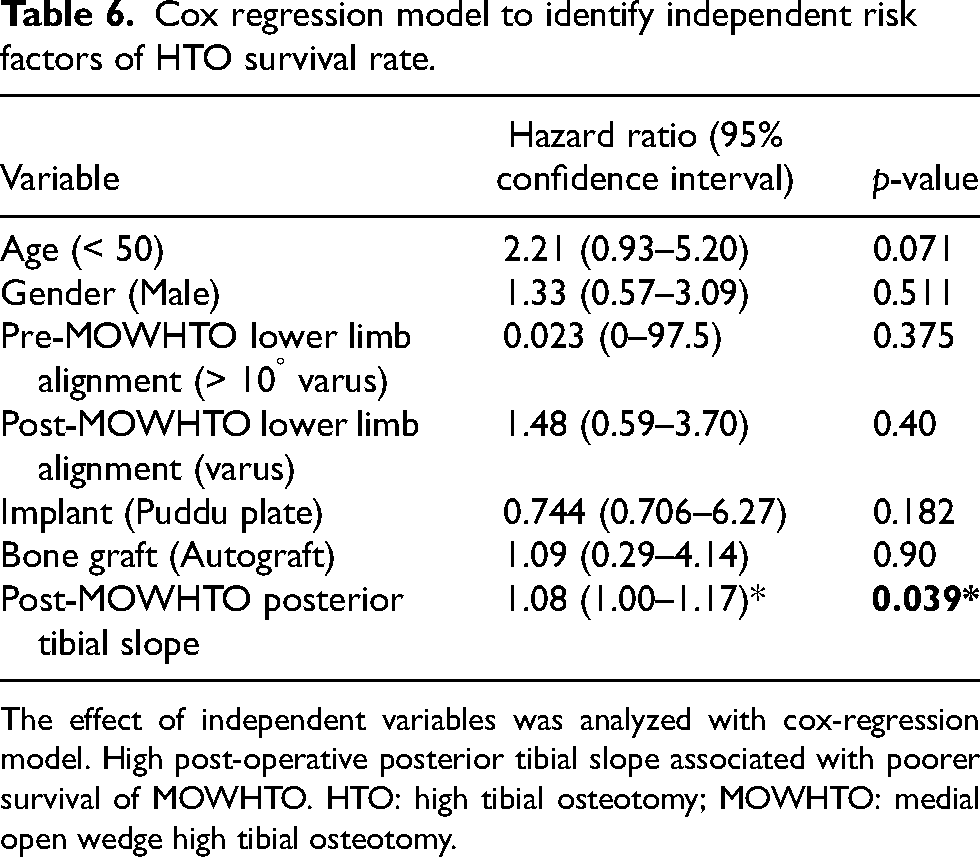
The effect of independent variables was analyzed with cox-regression model. High post-operative posterior tibial slope associated with poorer survival of MOWHTO. HTO: high tibial osteotomy; MOWHTO: medial open wedge high tibial osteotomy.
Discussion
Survival rate of MOWHTO
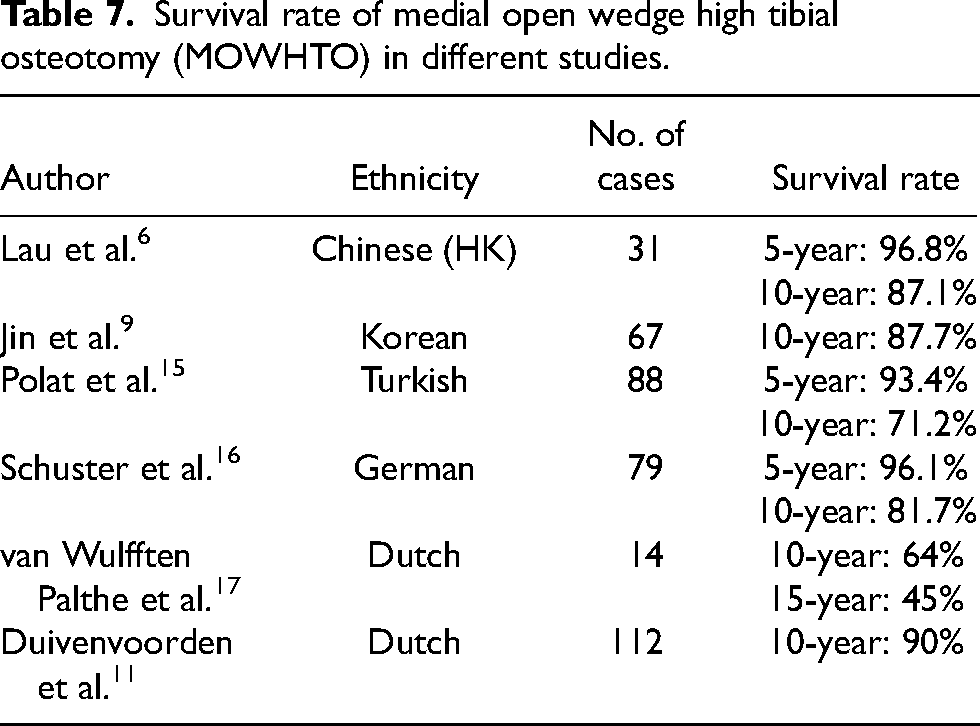
The overall survival rate of MOWHTO performed in our centre is compatible with other parts of Asia and the rest of the world. Lau et al. 6 reported a 10-year survival rate of MOWHTO in their centre in Hong Kong of 87.1%. Jin et al. 9 also reported a similar 10-year survival rate of MOWHTO of 87.7% in the Korean population. Other European studies showed the 10-year survival rate of MOWHTO from 64% to 90%. (Table 7)
Survival rate of medial open wedge high tibial osteotomy (MOWHTO) in different studies.
Complication of HTO
The complication rate of overseas studies ranges from 3 to 19% (Table 8). Common complications include deep vein thrombosis, peroneal nerve palsy, non-union and wound infection. In our study, there was no deep vein thrombosis but more wound infection is noted. This is possibly due to the overall incidence of deep vein thrombosis being lower in the Asian population. 10
Post-operative complication of high tibial osteotomy (HTO) documented in different studies.
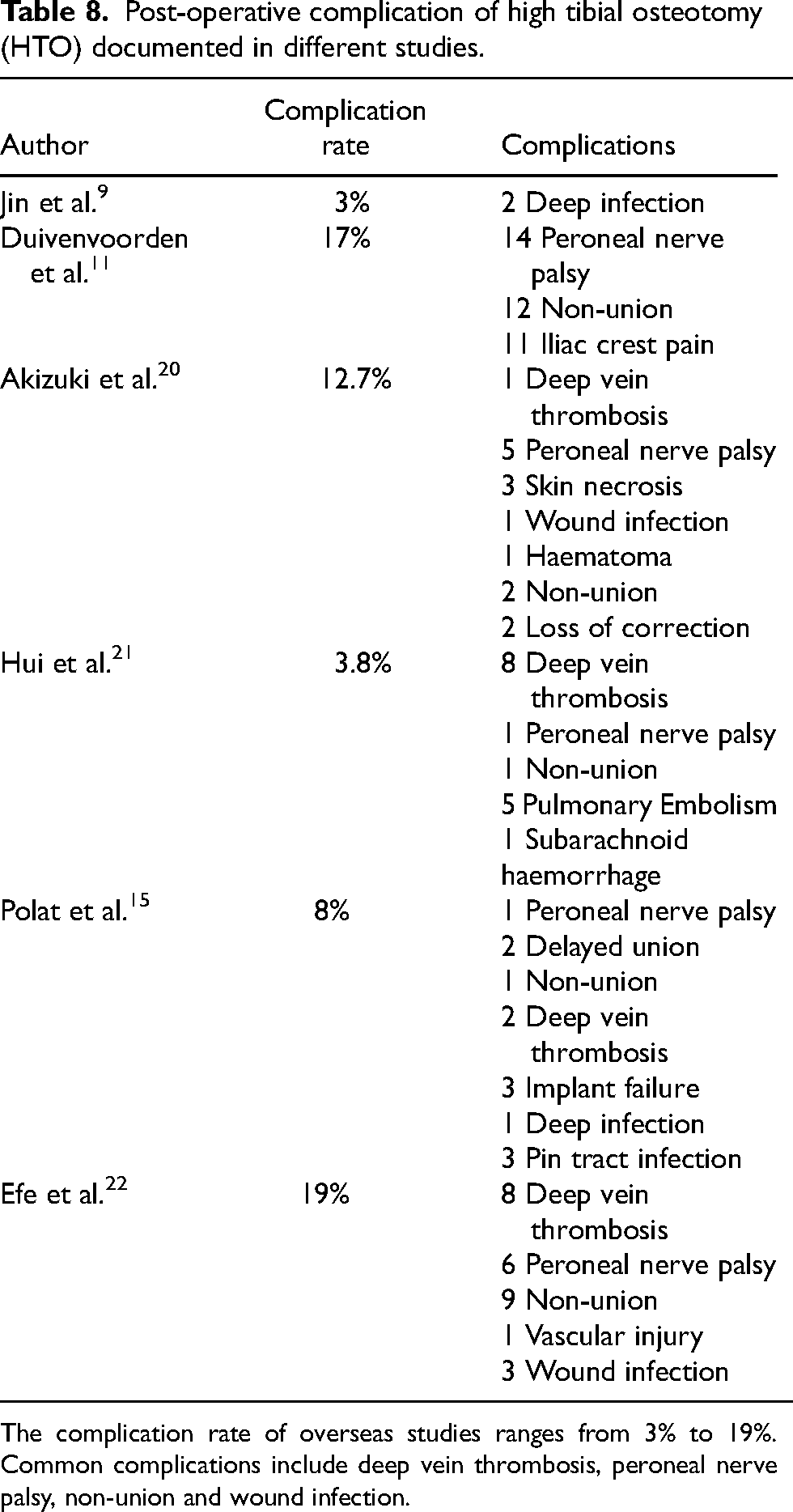
The complication rate of overseas studies ranges from 3% to 19%. Common complications include deep vein thrombosis, peroneal nerve palsy, non-union and wound infection.
Since we were doing medial opening wedge HTO, the peroneal nerve was not exposed and saved from injury. Duivenvoorden et al. 11 reported 14 cases of peroneal nerve palsy after HTO, all after lateral closing wedge HTO.
Conversion TKR
TKR is a reliable treatment measure for the patient with failed HTO. Study showed a 10-year revision-free survival rate up to 90%. 12 Meta-analysis showed no significant difference in function and pain scores between TKR with and without prior HTO. 13 Since prior HTO caused change in knee alignment and soft tissue scarring, there are several surgical challenges during the conversion TKR, which include problems in surgical approach, bone deformities, ligament balancing, and prosthesis selection. Knee arthroplasty after MOWHTO is technically easier compared to those after lateral closing wedge HTO. In conversion after MOWHTO, there is no disruption to proximal tibiofibular joint, less lateral soft tissue release and avoidance of peroneal nerve injury. 14
Blood supply to the skin of the knee joint mainly arises from the medial side, therefore multiple longitudinal incision may impair the blood supply to the skin flap. Alternative method to preserve the blood supply is to make a skin incision via the previous incision and then perform medial or lateral arthrotomy. For all our cases, though the previous incision for MOWHTO was at a medial paramedian location at the proximal tibia, we still managed to incorporate it into our incision for TKR, with the proximal part of the incision curving towards the midline.
Moreover, prior HTO may cause adhesion of the patella tendon and patella baja which makes the eversion of patella become difficult, especially in cases after lateral closing wedge HTO. Quadriceps snip, VY-plasty and tibial tubercle osteotomy can facilitate the exposure. Bastos et al. reviewed 141 conversion TKR following HTO, 8.3% of prior medial opening HTO and 24.8% of prior lateral closing HTO required additional exposure procedure including rectus snip and tibial tubercle osteotomy. 11 In our study, the mean Insall-Salvati ratio is 1.06 ± 0.22, with only one knee less than 0.80 and regarded as patellar baja. Apart from this case, there were 10 other cases that necessitated a quadriceps snip for exposure though without baja. This could be due to scarring patella tendon and fibrotic patellar fat pad. Erak et al. 18 reported the mean Insall-Salvati ratio to be 0.91 in knees after MOWHTO with 27% of the knees has patellar baja. They reported difficulties in patellar eversion in patients with patellar baja, one of their knees with patellar baja required quadriceps snip. Bastos et al. 19 reviewed 24 conversions TKR after MOWHTO with mean patellar height (Blackburn peel index) 0.79. They performed tibial tubercle osteotomy in 8.3% of the conversion TKR due to difficult soft tissue exposure.
Prior HTO may cause translation and meta-diaphyseal mismatch of the tibia, especially in knees with prior lateral closing wedge HTO. In the coronal plane, the proximal tibia was usually shortened, had a loss of bone stock and stem impingement on lateral tibial cortex, rendering difficulty in performing tibia resection and component placement.5,23 However, there was usually preservation of proximal tibial anatomy after MOWHTO and thus with less technical challenges. In the coronal plane, more intra-operative medial release is commonly performed in patient with prior MOWHTO. Bastos et al. 19 reported 91.7% of the patients with prior MOWHTO required medial release during conversion TKR because the medial structures were tensioned during the MOWHTO. In the sagittal plane, the tibial slope tends to increase after MOWHTO and this may lead to more anterior tibial bone resection and/or defect at the posterior tibia, leading to difficulty in flexion-extension gap balancing. 24 In our study, we found an increase in the mean posterior tibial slope of 14.5 ± 5.70°. Erak et al. 18 reported an increase in posterior tibial slope after MOWHTO. Their mean posterior tibial slope was 10.6° with 21% of the knees has posterior tibial slope more than 15°, which is similar to our findings. Yet, we did not have cases that were unable to achieve a balanced flexion-extension gap due to raised posterior slope.
In the patient with implant removal in same operation or tibial bone loss, a tibial stemmed implant can be chosen. In those who had excessive varus or valgus deformity, valgus-varus condylar constrained implant can be used. In our study, there were 3 cases (14.3%) required tibial stemmed implant and 2 cases (9.5%) required condylar constrained implant. Chalmers et al. 12 reported 4% and 8% of HTO required condylar constrained and tibial stem implant, respectively. Erak et al. 18 reported 27.8% of HTO required tibial stem. They used tibial stem in conversion TKR with removal of old implant in the same session in order to bypass the potential stress risers.
Conversion UKR
Although TKR is more commonly performed in conversion arthroplasty after HTO, we found that conversion UKR can be performed in suitable cases. In our study, the patient with conversion UKR complained of persistent medial knee pain 4 years after MOWHTO. The post-MOWHTO lower limb alignment film showed residual varus deformity. In view of the relatively young age, relatively well-preserved lateral joint space and medial knee pain, medial UKR was decided. The patient's knee pain and functional status improved after the conversion. Schuster et al. 16 reported 5 patients with previous MOWHTO converted into UKR. Schlumberger et al. 25 reported a 93% survival rate in 30 medial UKR with a history of HTO. They suggested patient without medial laxity and excessive valgus knee alignment can consider conversion UKR.
Risk factors affecting the survival of HTO.
The causes of conversion arthroplasty are multifactorial, which include the rate progression of osteoarthritis of the knee joint, coronal, sagittal lower limb alignment, activity level of patient. In our study, we noticed that high tibial posterior tibial slope associated with poorer survival of MOWHTO. However, the hazard ratio is close to 1, which may not suggest a significant increase risk of poor survival. Moreover, the mean posterior tibial slope in patients who required conversion arthroplasty was significantly higher than those who did not require conversion (14.5° VS 11.6°, p = 0.047). Studies reported that the posterior tibial slope increases after MOWHTO, which is compatible with our studies.26,27 Kim et al. 27 performed arthroscopy in patients before and after MOWHTO in a mean interval of 26.3 months. He found that high posterior tibial slope after MOWHTO associated with ACL degeneration. High posterior tibial slope after MOWHTO may alter the biomechanics by raising the anterior tibial translation. This may cause an increased tensile load of ACL and axial compressive force applied to knee joint which results in earlier degeneration of knee joint.
From other studies, age below 50 and body mass index below 25 are associated with better survival rate.20,21 This maybe due to different threshold on conversion arthroplasty. Most of the studies use conversion arthroplasty as end point for survival measurement. Survival is affected by multiple factors including waiting time for arthroplasty in local hospital, pain tolerance and willingness of performing operation of patients.
Limitations
The ROM, knee, and functional score of the patient before and after MOWHTO were not included in our study. This did not allow us to analyze the difference in the functional change after performing HTO. BMI was not recorded and analyzed in our study group, which is also a potential risk factor for the survival of MOWHTO. Moreover, some of the lower limb alignment films and lateral films of knee of the patients were not available for measurement due to loss of old films. Thus, the effect of alignment on survival of HTO cannot be fully demonstrated. Furthermore, post-TKR alignment was not reported and the outcome of the conversion TKR was not compared to our usual primary TKR in the current study.
Conclusion
In conclusion, MOWHTO gives a promising overall long-term survival rate and serves as a reliable measure to treat knee osteoarthritis with varus deformity. The survival of MOWHTO demonstrated in our study is compatible with local and overseas studies. The cause of conversion arthroplasty after MOWHTO is multifactorial, high posterior tibial slope may be one of the risk factor. If patients have progression of knee osteoarthritis after MOWHTO, conversion TKR and UKR can be promising treatment options. Most of the MOWHTO can be converted into conventional TKR. In cases with valgus overcorrection and or MOWHTO implant removal at the same operation, tibial-stemmed implant or condylar-constrained implants maybe required. In cases with difficulty exposure due to previous scarring, medial arthrotomy with quadriceps snip is an alternative approach. However, patellar baja or not does not predict the need for quadriceps snip during conversion arthroplasty.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.