
Abstract
Introduction
Radiographic study plays an important role in diagnosis of acute vertebral injuries and helps in proper management of those patients. X-ray radiographs and computed tomography (CT) are the initial imaging modalities used in the diagnosis of most cases of spinal injuries. But the magnetic resonance imaging (MRI) with an increasingly important role in the management of spinal injuries, it is the modality of choice for evaluation of ligamentous and other soft tissue structures, disc, spinal cord and occult osseous injuries.1–3
Reviewing the literature denote the superiority of MRI to CT of the thoracolumbar and lumbar spine for detection of ligamentous injuries, even in patients with negative CT findings.4–8 Due to high cost, it is necessary to detect the best use of this technique in the evaluation of thoracolumbar spinal injuries. 9
The PLC is composed of the supraspinous ligament, interspinous ligament, ligamentum flavum and the facet capsule. Importance of integrity of posterior ligamentous complex (PLC) as a major influencer on the spinal stability in patients with thoracolumbar fractures has recently been shown. Vaccaro et al. 10 reported a classification system including the patient's neurological status and PLC injury as items that can be evaluated. They also introduced a thoracolumbar injury classification and severity score (TLICS). This classification system was helpful in identifying posterior instability and is also used as a guide for treating thoracolumbar burst fractures.11–13 Many articles have reported that PLC injuries are a risk factor for delayed kyphotic deformity after spine fractures, because of its role in resisting flexion-deforming forces.14–16
Spinal stability was used to be assessed based on the fracture type and the integrity of the PLC, whereas the presence of anterior longitudinal ligament (ALL) or intervertebral disc injury is frequently ignored. Intervertebral disc injury is supposed to play an important role on spinal stability and fracture prognosis17,18 especially that thoracolumbar injuries are usually associated with intervertebral disc injuries19,20 which lead to kyphotic deformity through processes such as intervertebral disc narrowing and vertebral body collapse. Progressive intervertebral disc degeneration following injury has also been shown to affect kyphotic deformity over time.21–23
The aim of this study was to discover if presence of PLC injuries and/or intervertebral disc injuries or herniation will affect the results of management of thoracolumbar fractures.
Methods
The following study is a retrospective case series performed after obtaining institutional review board approval according to the principles of the Declaration of Helsinki. Seventy-two thoracolumbar spine injury cases were identified. The fractures were located in the thoracolumbar junction and lumbar region between T10 and L4. All blunt trauma patients over the age of 18 years with thoracolumbar spinal injuries were eligible for inclusion into the study. Exclusion criteria were patients more than 65 years of age to exclude osteoporotic fractures, pathologic spinal fractures, multiple vertebral fractures or vertebral appendices fractures. The fracture severity type was evaluated according to the Denis classification system and AO Spine classification system.11,24
Vertebral body measurements
Loss of vertebral body height (percentage of compression) was calculated as a percentage of the height loss normalized to the average of the vertebral bodies above and below the injured segment, as described by Willen et al. 25 kyphosis angle was measured as the angle between the superior endplate of the vertebra above the injured vertebra and the inferior endplate of the vertebra below the injured vertebra. Vertebral translation was also measured on midsagittal CT images. Vertebral translation was taken as the percentage of the distance from the postero-superior corner of the injured vertebral body to a line tangent to the posterior inferior cortex of the cephalad vertebral body (suprajacent translation) or to the posterior superior cortex of the caudal vertebral body (subjacent translation).
Scoliosis angle was measured as the angle between the intersecting lines drawn perpendicular to the superior end plate of vertebra above the fractured vertebra and inferior end plates of the vertebra below the fractured one.
The antero-posterior diameter and medial–lateral diameter of the spinal canal were measured at the injured segment. The sagittal transverse ratio was defined as the ratio of the antero-posterior spinal canal diameter to the medial–lateral spinal canal diameter, as described by Radcliff et al. 26
MRI examination technique and scanning protocols
MRI was done using 1.5 TESLA machine. Appropriate MR sequences and multiplanar imaging were performed for every patient using following sequences:
Localizer conventional spin echo sequence Axial and sagittal T1W sequence Axial, sagittal and coronal T2W sequence Sagittal-STIR T1W FS (fat saturated) sequence Coronal-TIRM (turbo inversion recovery magnitude) T2W sequence Susceptibility weighted imaging sequence.
Assessment of ligamentous injuries
Ligaments are essential components of the vertebral column, so, presence of their injury can change the stable injury to an unstable injury, 27 STIR-weighted MRI in the sagittal plane was used to identify the pattern of the fractures and to evaluate the state of the intervertebral discs, ALL and the PLC. Those imaging methods used to assess the level of injury and the integrity of the ALL and PLC at the spinal level were involved. Preoperative MRI was used to classify the PLC as either intact or disrupted based on the following criteria: (1) as focal disruption of the hypointense signal on all the sequences with associated prevertebral oedema best identified on STIR images, and/or (2) a high signal intensity on STIR-weighted MRI. The high signal intensity on STIR-weighted MRI was the most important finding, and the PLC injury was further classified as a supraspinous ligament and/or interspinous ligament injury based upon the MRI findings. 28
Assessment of intervertebral discs injury or herniation
Intervertebral discs injuries were checked through MRI. Intervertebral disc injuries were graded according to Sander's classification of traumatic intervertebral disc lesions. 29 Intervertebral disc injuries were classified as follows: grade 0, uninjured intervertebral discs in their normal condition; grade 1, hyperintense appearance on T2-weighted MRI images, as compared to adjacent intervertebral discs without traumatic change; grade 2, decreased signal intensity with perifocal hyperintense appearance on T2-weighted images and isointense to isointense appearance on T1-weighted images; and grade 3, an infraction of the disc into the vertebral body, annular tears or herniation into the endplate.
Assessment of neurological injury
Neurological injuries were assessed according to Frankel scale score.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS version 23.0) software for Windows (SPSS Inc., Chicago, IL, USA). All values are expressed as mean, standard deviation. Analysis of variance with a post-hoc test (Mann–Whitney U-test) was used for comparisons. Sample studied power was calculated using sample size post-hoc power calculator and it was 100%. In addition, some data were analyzed using Pearson's Chi-square and multivariate logistic regression techniques. P-values <0.05 were considered to be significant.
Results
Demographics
The study included 72 patients with thoracolumbar fractures. Patient's age ranged from 18 to 64 years (mean 38.4 years, females: average: 45 years (SD: 16.407, SD error: 3.421), males: average: 42.7 years (SD: 17.794, SD error: 2.468)). Thirty patients (45%) were females and 42 (55%) were males (P = 0.6038: non-significant). The causes of injuries were fall from a height, traffic accidents or direct. The fractures were located at the T11 level in 6 patients, at T12 in 22, at L1 in 24, L2 in 14, L3 in 3, L4 in 2 and L5 in one. There were 47 burst fractures, 13 compression fractures, 8 fracture-dislocations and 4 flexion distraction injuries (Figure 1).
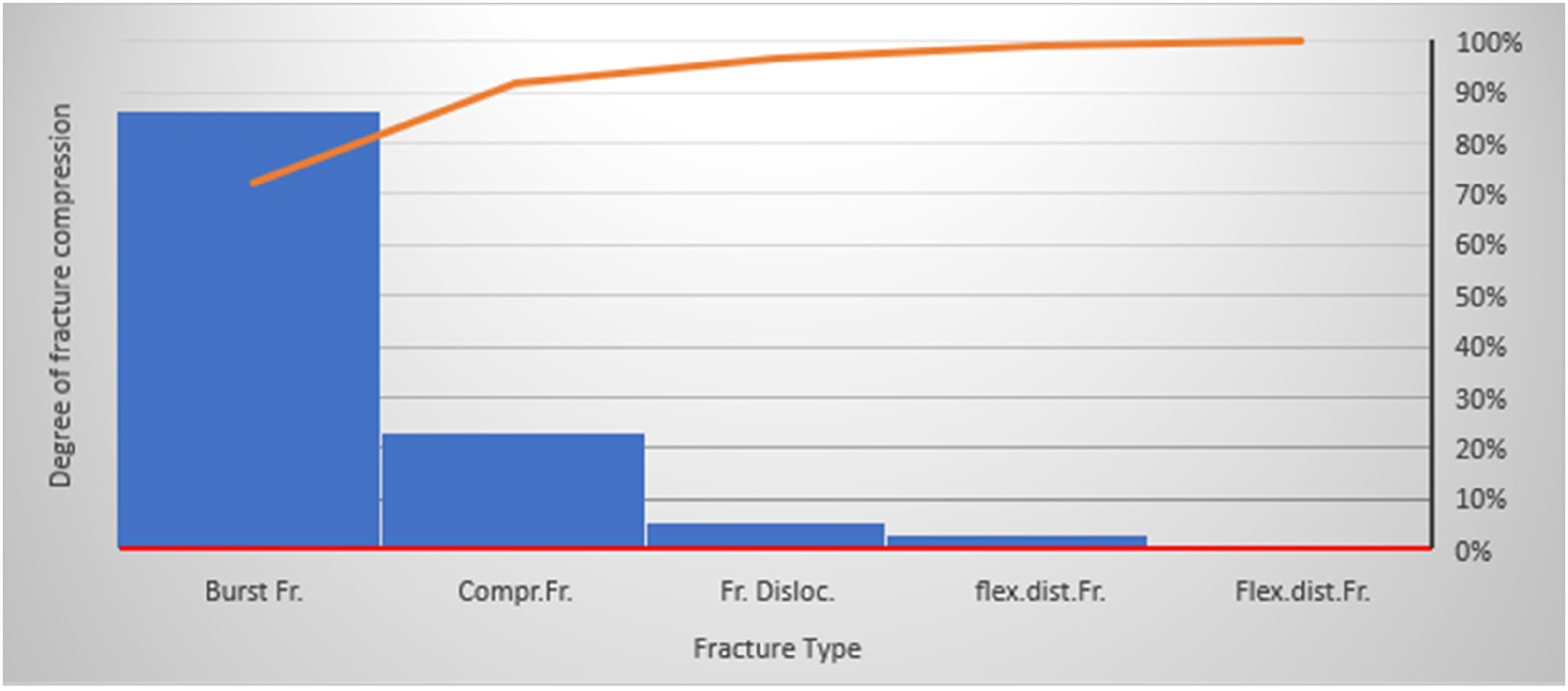
Correlation between vertebral body compression and type of fracture.
MRI evaluation revealed ligamentous injuries in 29 patients (39%) (Table 1). Correlation between fracture type and ligamentous injury was found to be significant: (P = 0.0143).
Correlation between ligamentous injury and fracture type.
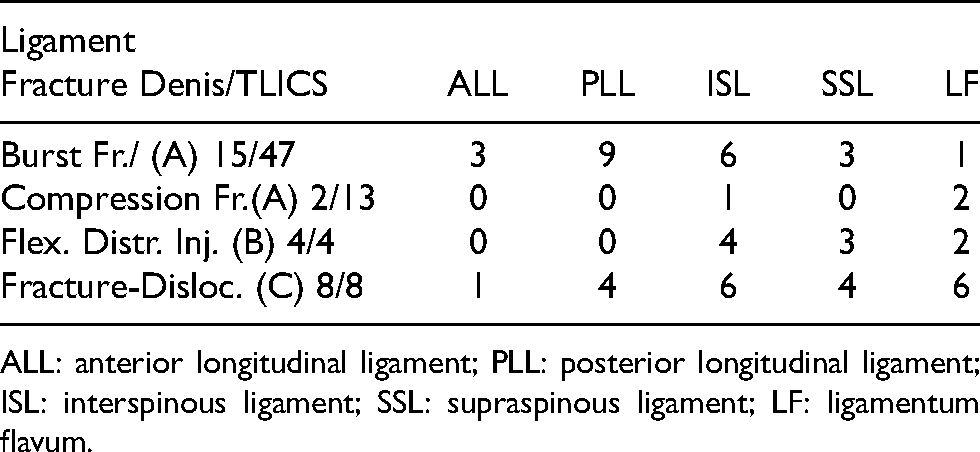
ALL: anterior longitudinal ligament; PLL: posterior longitudinal ligament; ISL: interspinous ligament; SSL: supraspinous ligament; LF: ligamentum flavum.
Degree of vertebral body compression ranged from 3% to 89%.
Correlation of percentage of compression with ligamentous injuries was non-significant statistically (P = 0.3480) (ANOVA).
Vertebral body translation was ranged from 0% to 75% and spinal canal narrowing ranged from 0% to 100% but no statistical significance was found between both parameters and ligamentous injuries (P was 0.0684 and 0.0753, respectively) (Figure 2).
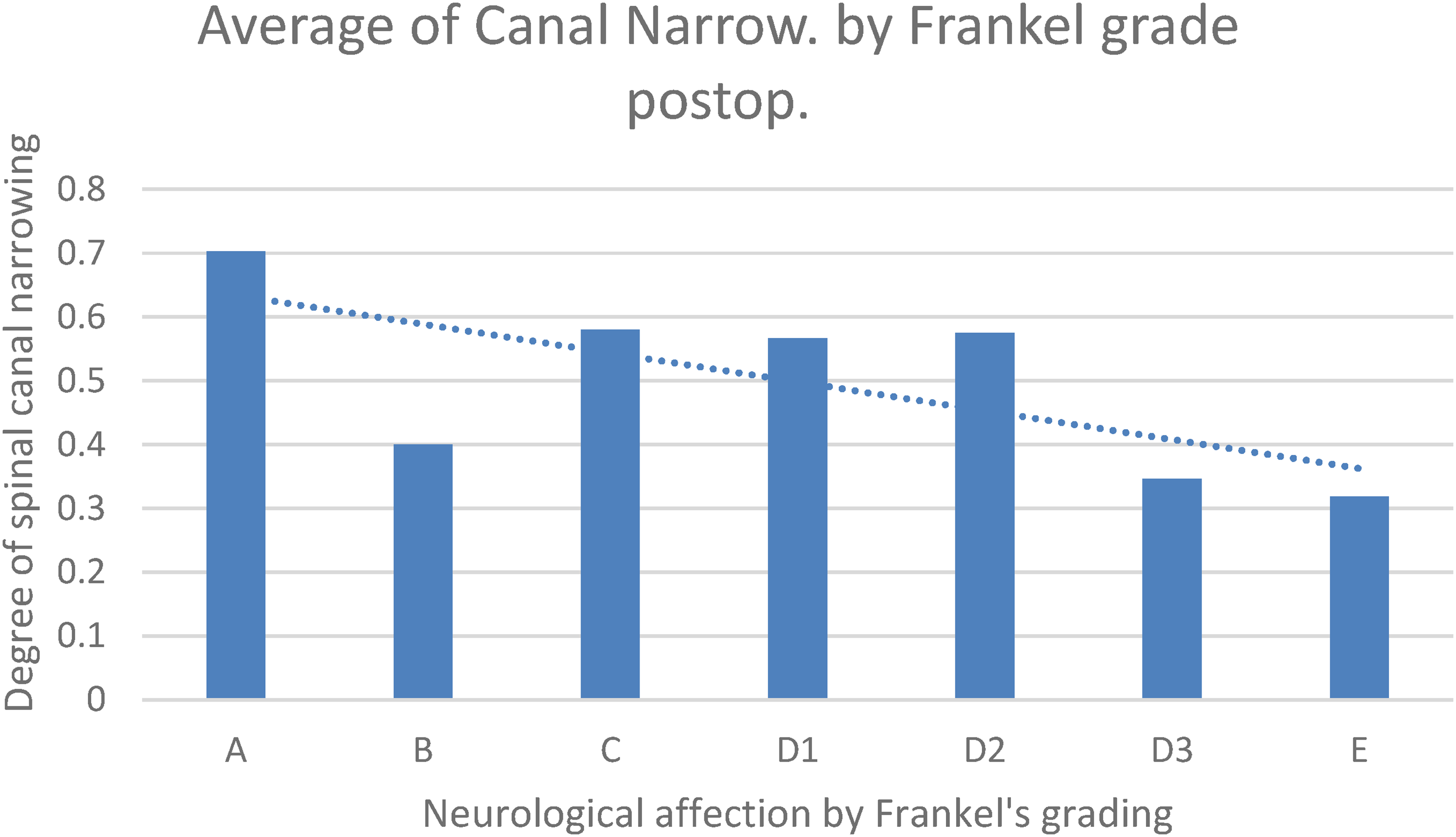
Correlation between spinal canal narrowing and improvement of Frankel grade.
Kyphosis angle ranged from 4° to 36°. Correlation between kyphotic angle with ligamentous injuries was non-significant (P = 0.8537) (ANOVA) (Figure 3).
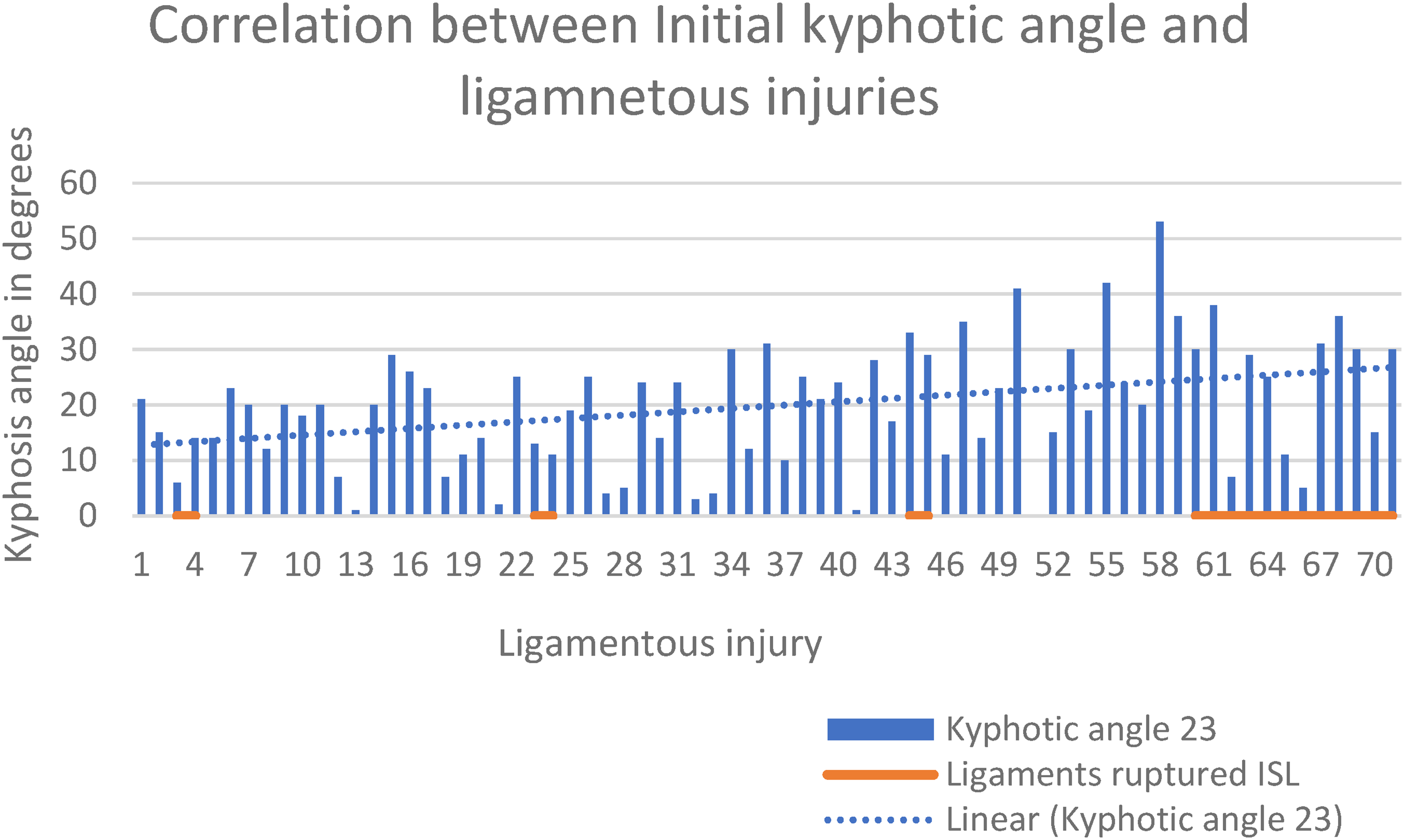
Correlation between kyphotic angle and ligamentous injuries.
Scoliosis angle ranged from 7° to 26°. Correlation between scoliotic angle with ligamentous injuries was also non- significant (P = 0.9864) (ANOVA).
MRI evaluation of intervertebral disc injuries upon admission revealed 14 cases grade 0, 17 cases grade 1, 9 cases grade 2 and 18 grade 3 cases according to Sander's classification (84% of the cases).
No statistical significance was found between Fracture type and disc injury: P = 0.4986.
Correlation between percentage of compression with Pre-Op. disc injury was non-significant (P = 0.4579) (ANOVA).
No statistical significance was found between scoliotic angle with Pre-Op. disc injury (P = 0.7502) (ANOVA).
Also, correlation between kyphotic angle with Pre-Op. disc injury was non-significant (P = 0.0863) (ANOVA).
Intervertebral disc herniation was found in 14 cases.
Correlation between fracture type and disc herniation was found to be insignificant (P = 0.4117).
Correlation between scoliotic angle with disc herniation was insignificant (P = 0.9832) (ANOVA).
Correlation between percentage of compression with disc herniation was also insignificant (P = 0.6897) (ANOVA).
But correlation between kyphotic angle with disc herniation was significant (P = 0.0219) (ANOVA).
The preoperative neurologic status was 19 patients being classified as Frankel E, 18 patients as Frankel D3, 12 patients as D2, 3 patients as Frankel D1, 6 patients as Frankel C, 5 patients as Frankel B and 9 patients as Frankel A.
The postoperative neurologic status was 34 patients being classified as Frankel E, 15 patients as Frankel D3, 6 patients as D2, 3 patients as Frankel D1, 3 patients as Frankel C, 3 patients as Frankel B and 8 patients as Frankel A. Correlation between postoperative neurological status and ligamentous injury was found to be significant: (P = 0.0344) (Figure 4).
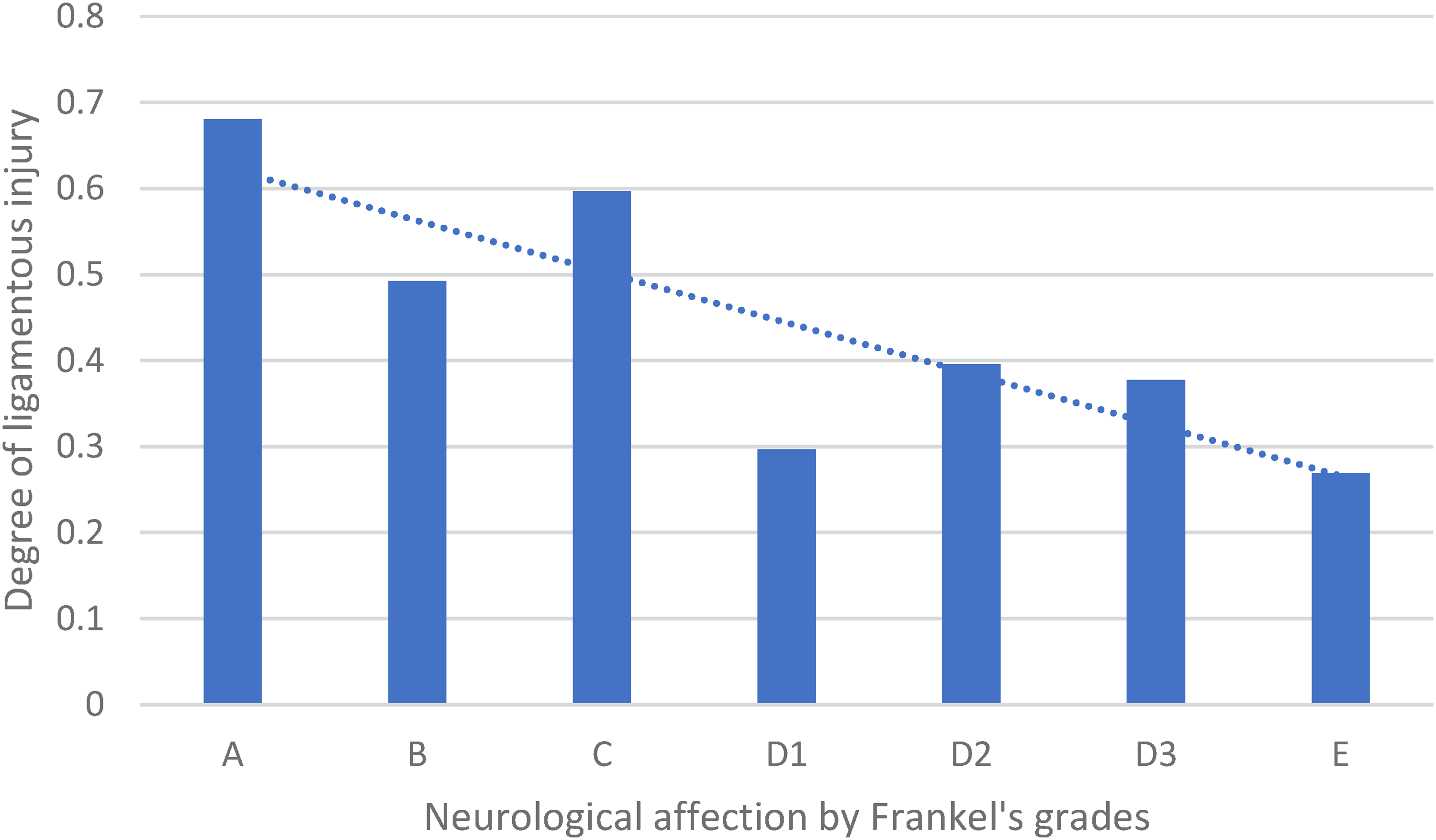
Correlation between ligamentous injury and neurological status.
Discussion
Thoracolumbar spine is the commonly affected region for spine fractures, followed by lumbar and cervical spine fractures, which account for almost 90% of all spinal injuries. 30 There were marked controversy over methods of diagnosis and treatment in the literature.31–33 The controversy was mainly regarding the assessment of fracture stability, where presence of different opinions in evaluation of fracture stability led to the differences in treatment choice of thoracolumbar burst fractures.
Imaging plays an important role in the diagnosis and clinical management of spinal trauma. AO Spine guidelines suggested that MRI should be performed in adult patients with acute spinal cord injury before surgical intervention to aid in clinical decision making, and before or after surgical intervention for predicting neurologic outcomes. 34 Öner et al. highlighted MRI's diagnostic power against conventional radiographs and CT in the reproducibility of AO classification. 35
The clinical evidence that the common radiological parameters used for assessment of thoracolumbar injuries as loss of vertebral height, local kyphotic angle, vertebral body translation, canal compromise and so on are reliable indicators of PLC injury is very low.36,37
The role of intact PLC is to keep stability of the thoracolumbar spine and its disruption may lead to relative instability of the spine and subsequently surgical intervention.
In this study, evaluation of injury of soft tissue components of the spinal column (PLC and intervertebral discs) and its correlation to management outcomes was assessed. Seventy-two patients with thoracolumbar spine injury cases were evaluated. The fracture severity type was evaluated according to the Denis classification system and AO Spine classification system.11,24
Ligamentous injury was found in 39% of the patients. In this study, Singh et al. 27 mentioned that there was no ligamentous injury seen in 50% of cases.
This study used MRI to identify the presence of a PLC injury in thoracolumbar and lumbar fractures and examined whether radiographic parameters could be predictors of a PLC injury as there is little to no supportive clinical evidence that they are reliable indicators of PLC injury. The results showed that there was no correlation between those parameters and PLC injury. Hiyama et al. found that vertebral body height, vertebral translation and canal compromise were not associated with PLC injury, while local kyphosis > 20° was associated with PLC injury in patients with thoracolumbar fractures. 38 McAfee et al. 15 recommended 30° kyphosis as a threshold for surgical intervention, since kyphosis >30° is associated with instability. From these data, it is widely accepted that the posterior ligaments have probably failed if there is greater than 30° of kyphosis and/or 50% of vertebral body height on plain radiographs. On the other hand, some studies had reported the successful conservative treatment of patients with this sign of instability.36,37 Radcliff et al. 26 reported that a loss of vertebral body height of >50% and kyphosis >20° are not predictive of PLC injury in patients with thoracolumbar burst fractures. Petersilge et al. did not find any significant correlation between the radiographic appearance of the fractures and PLC injury. 39
Supporting our findings, study was done by Hartmann et al. 40 where they could not evaluate a clear, simple formula for definitively identifying PLC injuries and Alanay et al. 41 who followed up the natural course of thoracolumbar fractures with intact PLC using MRI and revealed that the intact PLC is not sufficient to prevent correction loss provided by closed reduction.
Reviewing the literature, we could not find any articles correlating the ALL injury with the clinical results of thoracolumbar injuries. Haris et al. 42 comparing preoperative MRI evaluation with operative findings found that 15 patients of which 6 were found to be injured on the preoperative MR images out of the 9 that were injured on operative assessment. The remaining three were reported as false negative thus giving a sensitivity of 66.6%. Goradia et al. 43 had reported a similar limited sensitivity (71%) for the ALL. This may add more on confusing classification systems used for assessment of thoracolumbar injuries.
Intervertebral disc injury is an important factor that influences postoperative spinal stability and prognosis. However, the common clinical classification systems for thoracolumbar vertebral fractures, including the AO classification, Denis classification, load-sharing classification and TLICS, have not provided an adequately detailed description for the severity of intervertebral disc injury.17,18
The intervertebral disc is a cartilage complex that is vulnerable to injury from stretches or shear force, whereas great compression forces can also result in traumatic intervertebral disc injuries. 44
This study did not find any correlation between traumatic intervertebral disc injury and fracture type, vertebral compression, kyphotic or scoliotic angles but statistically significant correlation was found between intervertebral disc herniation and kyphosis angle. Su et al. 45 study indicated that the degree of intervertebral disc injury increases with the severity of the fracture and that intervertebral disc injury is positively correlated with the AO fracture type and need to integrate the assessment of intervertebral disc injury into the classification system for thoracolumbar vertebral fractures.
Kanezaki et al. 46 denoted that the kyphotic changes noticed in thoracolumbar spine fractures follow up occurred mainly at the intervertebral disc level rather than at the site of the vertebral body. And while the vertebral body kyphosis angle does not change after bone union, injured intervertebral discs can still undergo degeneration. They found that kyphotic deformity occurred mainly at the intervertebral disc level, which is also consistent with results reported by Aono et al. 22 But anyway, they could not find any correlation between kyphosis and intervertebral disc degeneration as our findings denoted. It can be concluded that severe intervertebral disc injuries do not necessarily result in kyphotic deformity. Helton et al. 47 analyzed separately the height of the fractured vertebral body and of its adjacent disks, and in the final evaluation of sagittal alignment they observed that the main factor related to the loss of the correction obtained by surgery was the reduced height of the intervertebral disks adjacent to the fractured vertebra.
One could argue that radiological changes are only relevant if they are strongly associated with changes in clinical outcomes, which is not necessarily true. 32 This study denoted that correlation between postoperative neurological status and PLC injury was found to be significant. Reviewing the English literature, we could not find many articles discussing this issue. Machino et al. 48 concluded that the presence of PLC injury significantly influenced the severity of neurological damage. Helton et al. 47 concluded that there was no correlation between correction of fracture and functional result was observed in his patients. Only the loss of height of the intervertebral disk adjacent to the fractured vertebra was related to unsatisfactory functional results.
This study had some limitations, being retrospective with small heterogeneous sample including thoracolumbar and lumbar vertebral fractures with potential risks of bias. On the other hands, the results of this study add more light to the importance of intervertebral disc injury or herniation in assessment of thoracolumbar spine injuries.
Conclusion
Results of this study demonstrated that there is a correlation between the fracture type and neurological improvement with the ligamentous injury while vertebral body compression, translation, scoliosis, kyphosis and canal compromise do not significantly correlate with PLC spine injury in thoracolumbar fractures.
No correlation was found between the disc injury and fracture type. Kyphotic deformity occurs mainly due to disc herniation at the level of the intervertebral discs not the vertebral body.
Footnotes
Author contribution
The author is responsible for the manuscript from developing the idea and research question to data collection and writing the manuscript.
Availability of data and materials
The datasets generated during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The study was approved by the local ethics committee and followed the Declaration of Helsinki and the Guidelines for Good Clinical Practice.
Consent to Participate
All participants signed a consent to participate.
Consent to Publish
Here is my consent as an author for publishing the manuscript in international orthopedics.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.