
Abstract
Keywords
Introduction
Flat foot deformity is characterized by loss of the medial longitudinal arch, forefoot abduction, hindfoot eversion, and often Achilles’ tendon contracture, with the entire sole coming into complete or near-complete contact with the ground. 1
During foot development until 6–7 years of age, the lower extremity is physiologically positioned in calcaneal valgus, knee valgus, hip valgus, and internal rotation. Around the age of 6 years, the knee joint axis straightens, and the calcaneal valgus decreases.2,3
Flatfoot deformity may develop due to injury, posterior tibialis tendon dysfunction (PTTD), unusual or prolonged stress to the foot, faulty biomechanics, as part of the normal aging process, with increased connective tissue laxity, obesity, and diabetes, in pregnant women due to increased elastin.4,5
Johnson & Strom in 1989 described three stages of PTTD, universally accepted for a long time, 6 Bluman et al. in 2007 updated this classification to provide a more descriptive and comprehensive system. 7
Many strategies for the treatment of flexible flatfoot have been reported, including calcaneal osteotomy, lateral column lengthening, subtalar arthroereisis, and arthrodesis. 8
Arthroereisis is a procedure in which an implant screw is inserted inside the sinus tarsi. The implantation of the screw expands the subtalar joint vertically, elevating the head of the talus which realigns the longitudinal arch of the foot and subsequently reduces the flatfoot deformity. 9
Medializing calcaneal osteotomy (MDCO) can be used to restore foot alignment, decrease the load on the medial arch, normalize force at the talonavicular joint, re-position the Achilles tendon to function as a heel inverter, to produce the desired hindfoot correction. 10
Controversy remains regarding indication, timing, and method for operative treatment of flat foot; thus, this study was conducted to compare two different surgical treatments for symptomatic Planovalgus feet: MDCO and subtalar arthroereisis.
Materials & methods
Institutional review board approval was acquired for a prospective randomized double center study that was done at Kasr al Ainy foot and ankle department & orthopedic department of El Sahel teaching hospital between May 2017 & May 2019; this study was implemented to compare two surgical methods for management of symptomatic flexible flat feet; the first method was represented in a MDCO utilizing modified step plate, while the second method was represented in arthroereisis utilizing subtalar implant.
Inclusion criteria
Stage 2 according to Johnson & Strom classification system, stage 2.A.1 according to Bluman & Myerson classification system, flexible pes Plano valgus deformity, painful symptoms refractory to conservative treatment, independent ambulation without assistive devices, age between 14 and 60.
Exclusion criteria
All stages according to Johnson & Strom classification system rather than stage 2, all stages according to Bluman & Myerson classification system rather than stage 2.A.1, patients taking medication affecting motor control, rigid flatfoot, midfoot or hindfoot arthritis, age below 14 and above 60.
Sample size
Assuming a standard deviation (SD) of 10, the minimum needed sample size to detect a difference of 10 points on the American Orthopaedic Foot and Ankle Society (AOFAS) score at an alpha threshold of 0.05 with 80% power is 34. So, each group should include at least 17 feet. Therefore, we included 20 feet per group to allow for drop-off.
Clinical assessment
The AOFAS score for ankle and hindfoot: It covers four different regions of the foot: The ankle–hindfoot, midfoot, metatarsophalangeal (MTP)-interphalangeal (IP) for the hallux, and MTP-IP for the lesser toes, each measure is comprised of nine questions covering three categories: pain (40 points), function (50 points), and alignment (10 points). These are all scored together for a total of 100 points, (90–100 points) was considered excellent score, (80–89 points) referred to as good score, fair (70–79 points), and poor (<70 points).
The Foot Functional Index (FFI): It consisted of 17 questions; the pain subcategory consisted of five items and measures foot pain in different situations; the disability subcategory consisted of nine items and measures difficulty performing various functional activities because of foot problems; the activity limitation subcategory consisted of three items and measured limitations in activities because of foot problems; scores were ranged from 0 to 100, with a higher scale indicating worse score.
Radiographic evaluation
Standard radiographs of the foot including weight-bearing anteroposterior (AP), weight-bearing lateral, oblique, hindfoot alignment radiographs while computed tomography and magnetic resonance imaging were done preoperatively to exclude tarsal coalitions, look for PTT, medial collateral, and spring ligament pathologies. Radiographs were taken preoperative and postoperative at 1st day, 2nd, 6th, 12th week; Varied angles that were recorded preoperative and postoperative at 6th and 12th week including AP radiographs angles: AP talo 1st metatarsal angle (APTM1, normal: 0), AP talocalcaneal angle (APTCA, normal: 17°–21°), lateral radiographs angles: lateral talocalcaneal angle (LTCA, normal: 35°–50°), calcaneal inclination angle (CIA, normal: 20°–30°).
Operative details & randomization
Forty feet were prepared for surgery during the study period with all patients who gave informed consent for participation and technique were selected according to a random number generated by the computer that was enveloped securely to be opened at surgery time; patients were under spinal anesthesia; surgeries were performed on a standard radiolucent table, with the presence of intraoperative fluoroscopy (C-arm); Tourniquet was applied.
MDCO technique using modified step plate
The patient was positioned in the lateral decubitus position; incision was made approximately 1.0 cm posterior to the tip of the lateral malleolus and 1.0–2.0 cm anterior to the insertion of the Achilles tendon; it was also extended from the superior border of the calcaneus anterior to the retrocalcaneal space to the inferior border of the calcaneus deep to the plantar fascia (Figure 1). The sural nerve and peroneal tendons were avoided. The dissection was continued down to the periosteum, which was reflected at the proposed osteotomy site, the lateral wall of the tuberosity was exposed and Hohman retractors were placed on the dorsal and plantar aspects of the tuberosity; an oblique osteotomy was made in line with the skin incision using oscillating saw blade; it was made approximately 1 cm posterior to the posterior process of the talus and perpendicular to the lateral border of the calcaneus; completion of the medial cortex was done in a carefully controlled manner using a broad osteotome; a toothless lamina spreader was placed in the osteotomy site and spread to relax the medial soft-tissue attachments to the calcaneus. After removal of the lamina spreader, the posterior calcaneal tuberosity was translated 7.5–10 mm medially according to the desired degree of correction and secured with a 7.5-mm or 10 mm modified locked step plate, screw placement was checked under fluoroscopy; followed by subcutaneous and skin closure of incision, then the incision was covered by sterile dressing with the application of below-knee posterior slap.
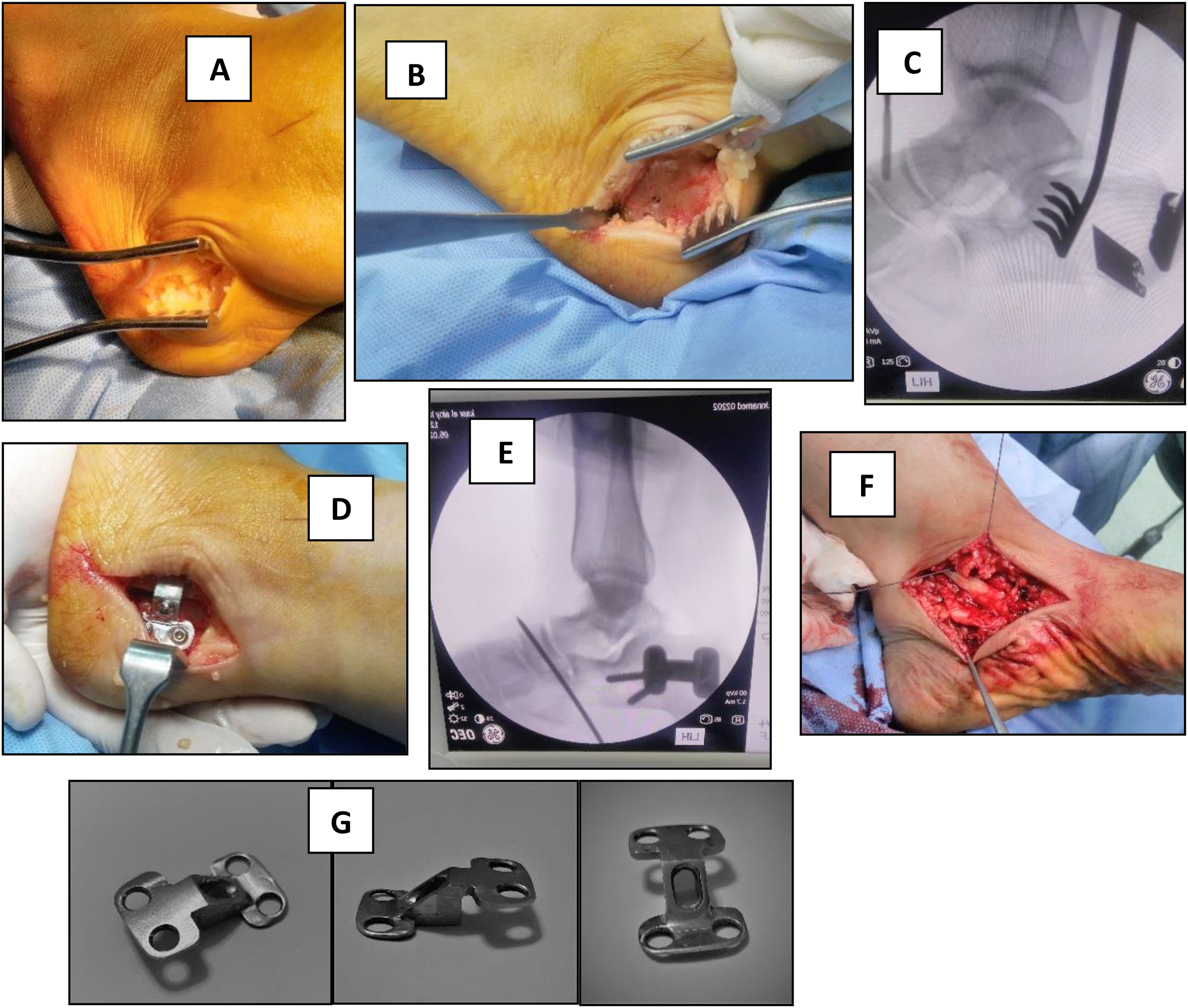
MDCO technique using modified locked step plate with FDL transfer. (A) Oblique skin incision over the lateral calcaneal border. (B) Exposing lateral calcaneal wall. (C) Oblique osteotomy using an oscillating saw. (D) Medialization and fixation using modified locked step plate. (E) Screws and plate adjustment under fluoroscopy. (F) FDL tendon transfer. (G) Modified locked step plate (images were taken intraoperatively at orthopedic surgery operative rooms of Kasr Al Ainy Hospital, January 2019).
Arthroereisis technique using conical subtalar implant
The patient was placed in a supine position; the Sinus Tarsi was palpated just inferior and distal to the tip of the fibula; a longitudinal 1 cm incision was created dorsal to the peroneal tendons over the soft-tissue sulcus; blunt dissection with a hemostat exposed the tarsal canal; a blunt guidewire was then inserted from lateral to medial through the sinus tarsi ; the trial sizers were advanced into the sinus tarsi beginning with the 8 mm sizer and increasing as necessary by increments of 1 mm; the appropriate sizer limits pathologic eversion without causing hindfoot varus; once the best sizer was identified, the AP radiograph was checked; the trial implant or the sizer typically crosses half of the mediolateral diameter of the talar neck and should not protrude beyond the lateral border of the talar neck; the conical subtalar implant was then inserted over the guidewire after which the guidewire was removed and the wound was closed in routine fashion; at the end of the procedure incision was covered by sterile dressing with the application of elastic bandage (Figure 2).
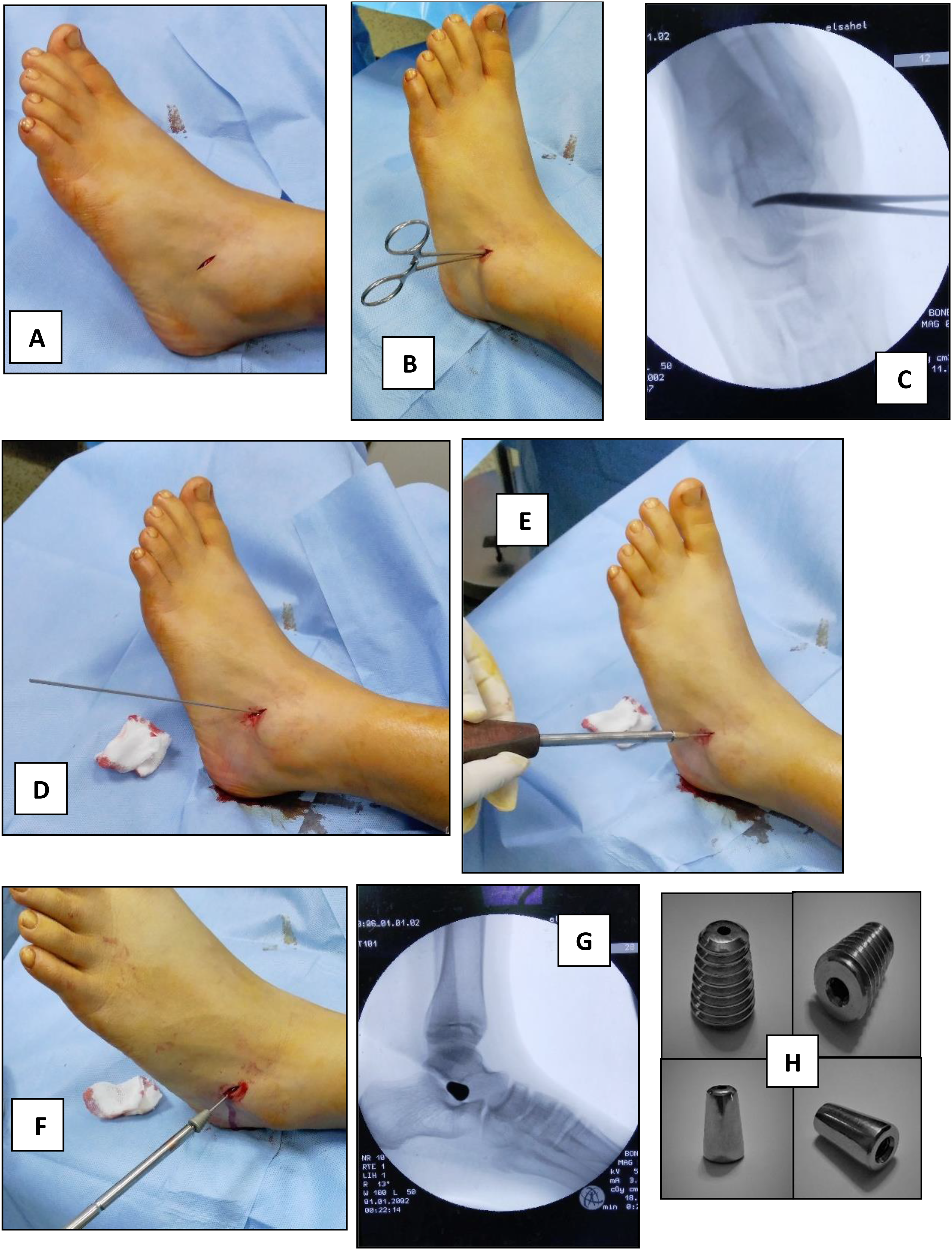
Arthroereisis technique using subtalar threaded cannulated conical implant. (A) 1 cm skin incision over sinus tarsi. (B) Blunt hemostat. (C) Checking direction under fluoroscopy. (D) Blunt guide wire inserted from anterolateral to posteromedial. (E) Trial sizer with increments of 1 mm. (F) Screw placement over the guidewire. (G) Checking screw placement under fluoroscopy for final adjustment. (H) Screw and trial sizer (images were taken intraoperatively at orthopedic surgery operative rooms of El Sahel Teaching Hospital, October 2017).
At the end of each procedure
If Achilles’ tendon tightness was encountered, lengthening was performed and Flexor digitorum longus tendon transfer had been done if more correction was required.
Post-operative care
MDCO patients follow-up
Patients in this group were instructed not to weight bear during the first 6 weeks; at the 2nd week post-operative posterior slap and stitches were removed, with the application of below-knee cast; 6-weeks post-operative cast was removed and patients were allowed to completely weight bear after confirmation of bony union. Patients were instructed to come for follow-up every 3 months to continue assessment and look for complications or recurrence.
Arthroereisis patients follow-up
All patients were instructed not to weight bear during the first 2 weeks; 2-weeks post-operative elastic bandage and stitches were removed, patients were allowed to completely weight bear; if there's a difficulty in weight-bearing or walking, 2 weeks’ physiotherapy was prescribed. Patients were instructed to come for follow-up every 3 months to continue assessment and look for complications or recurrence. Removal of the arthroereisis implant was done if there's a complication encountered and not removed routinely.
Statistics
Data were statistically described in terms of mean, all statistical calculations were done using computer programs SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA) version 23 for Microsoft Windows, parametric one-tailed Student t-test for dependent means was used to compare preoperative and postoperative results while the parametric two-tailed student t-test for independent means was used to compare between the two groups; a p-value of less than 0.05 was considered a statistically significant outcome.
Results
Time plan, sample size, follow-up period
By the end period of the study (May 2019), arthroereisis was done in 20 feet & MDCO was done in 20 feet but there were only 26 patients (37 feet) available for our analysis of results. 17 feet in the MDCO group utilizing modified step plate (group A) & 20 feet in the arthroereisis group utilizing subtalar implant (group B) as 3 patients (3 feet) were dropped off and we were unable to know the exact reason for missing follow-up; our follow-up period ranged from 7 to 14 months with a mean follow-up period 10.14 months (group A: 10.65 months, group B: 9.7 months).
Gender & age distribution
About 25 males and 12 females were available for analysis; gender distribution in our study includes 10 males and 7 females in the group (A) while in the group (B) there were 15 males and 5 females; patient's ages ranged at the time of surgery from 14 to 50 years (mean 21.38 years); group (A) ages ranged from 17 to 50 years (mean 23.82 years) while group (B) ages ranged from 14 to 42 years (mean 19.3 years).
Clinical results
Flexible flat feet were bilateral in 11 patients; 10 of them were males & 1 female; arthroereisis was done bilaterally in six patients while MDCO on one side and arthroereisis on the other side in five patients; within the MDCO group FDL transfer was done in 9 feet while both FDL transfer and TAL were done in 2 feet, unlike arthroereisis group in which TAL was done in 2 feet, although we did not find any significant difference in postoperative clinical and radiological scores between patients undergone soft tissue procedure combined with arthroereisis or MDCO and patient undergone arthroereisis or MDCO alone (Figures 3–8).

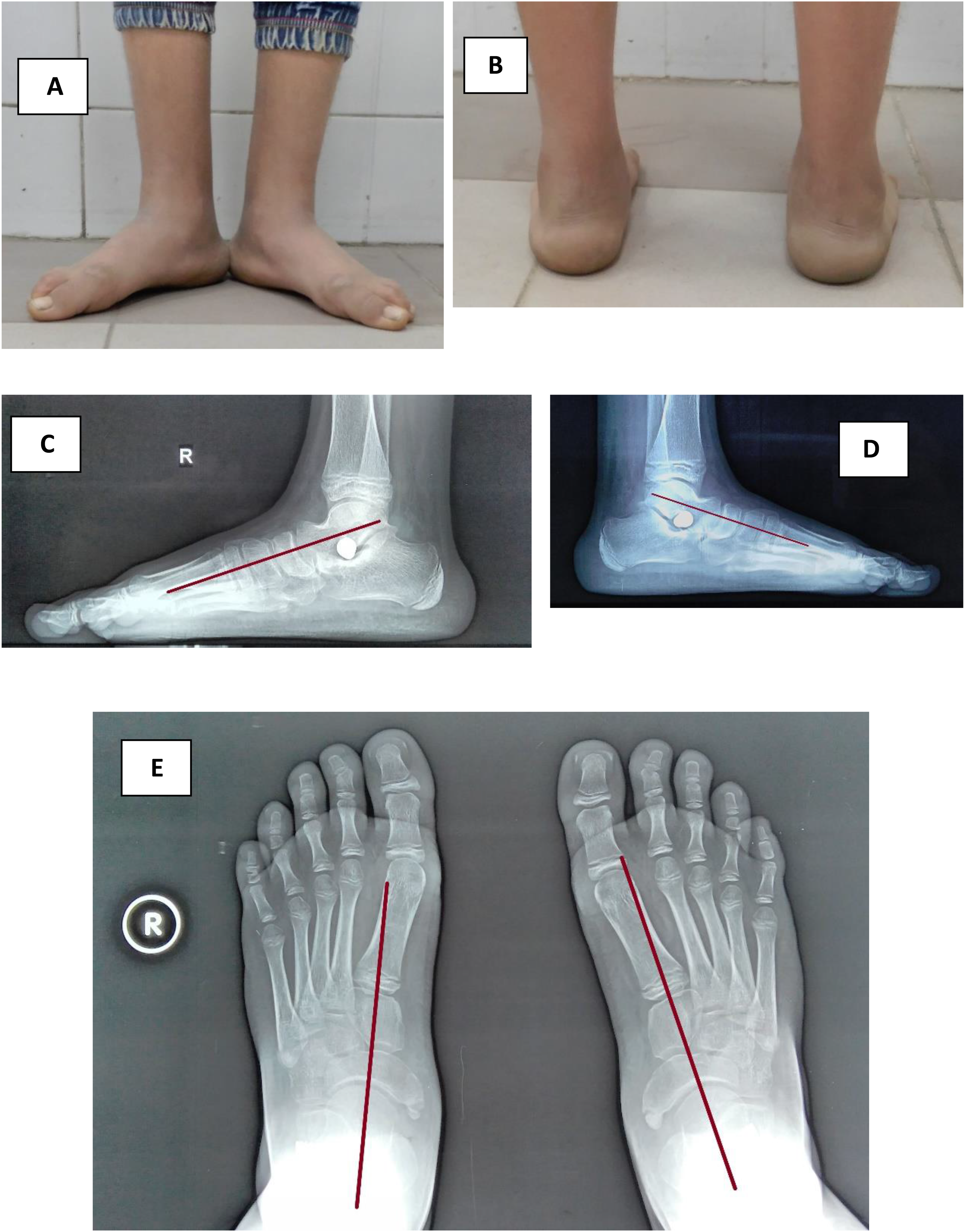
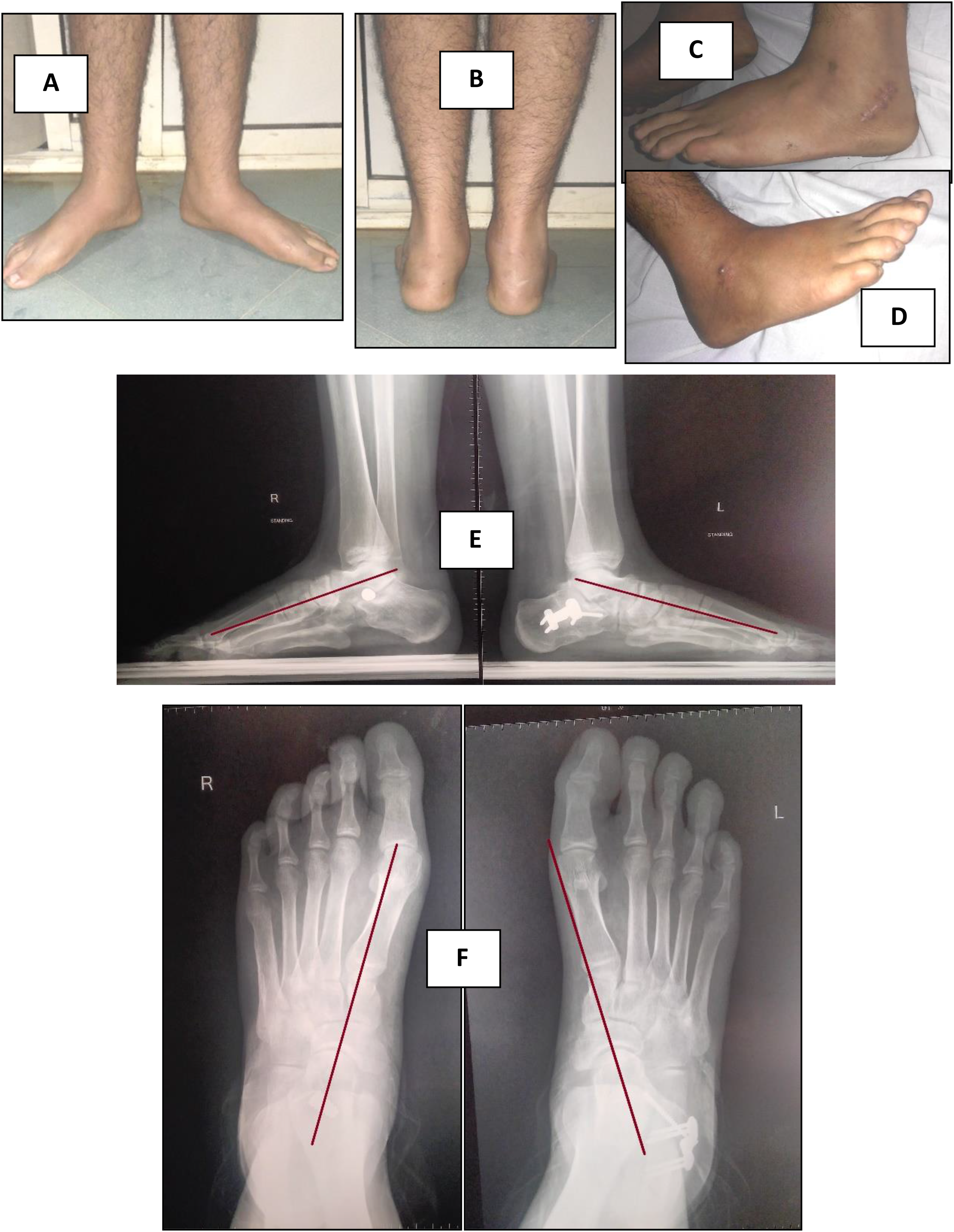
Preoperative clinical and radiological assessment of both feet in a 15 years old male. (A) Frontal foot view of both feet revealing flat feet. (B) Rear feet view showing valgus heels. (C) Tiptoe standing revealing flexible flat feet. (D) Oblique view X-rays of both feet showing that there is no tarsal coalition. (E) AP standing view revealing talonavicular uncoverage in both feet. (F) Lateral standing view showing talar declination in both feet. (images were taken at orthopedic surgery outpatient clinic of El Sahel Teaching Hospital).
Postoperative clinical and radiological results at the 3rd month postoperatively in a 15 years old male under gone arthroereisis bilaterally. (A) Frontal foot view of both feet revealing restored medial longitudinal feet arches. (B) Rear feet view showing restored neutral alignment of both heels. (C and D) Lateral standing view showing improvement of talar declination in both feet. (E) AP standing view revealing improvement of talonavicular coverage in both feet (images were taken at orthopedic surgery outpatient clinic of El Sahel Teaching Hospital).
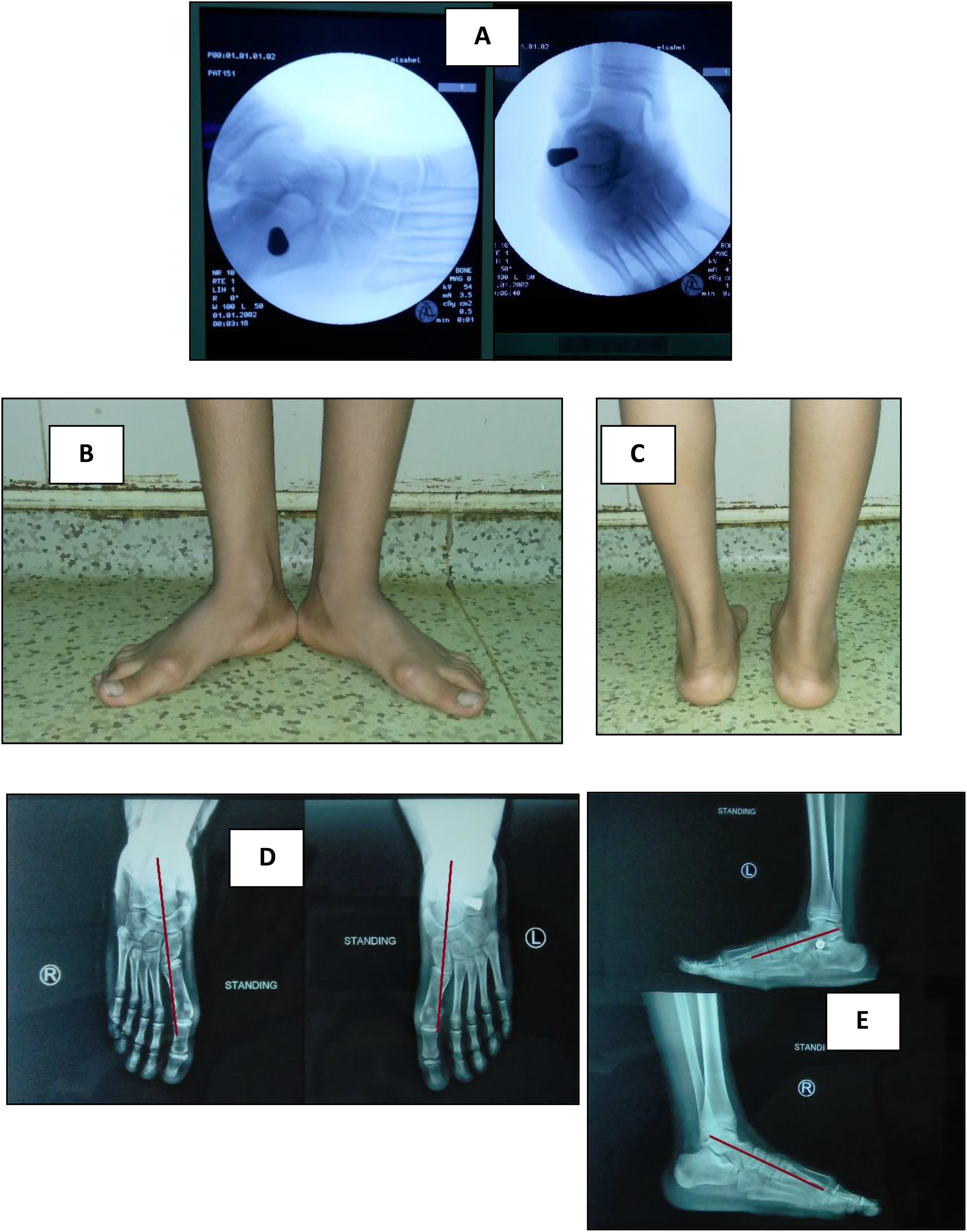
Postoperative clinical and radiological results at the 8th month follow-up after removal of the extruded screw from RT foot of a 15 years old male undergone arthroereisis bilaterally. (A) Intraoperative X-rays showing extruded screw from RT foot. (B) Frontal foot view of both feet showing maintained improvement of medial longitudinal feet arches without recurrence of deformity. (C) Rear feet view showing maintained neutral alignment of both heels. (D) AP standing view revealing maintained improvement of talonavicular coverage in both feet. (E) Lateral standing view showing maintained improvement of talar declination in both feet (images were taken at orthopedic surgery outpatient clinic of El Sahel Teaching Hospital).

Preoperative clinical and radiological assessment of both feet in an 18 years old male. (A) Frontal foot view of both feet revealing flat feet. (B) Rear feet view showing valgus heels. (C) Tiptoe standing revealing flexible flat feet. (D) Oblique view X-rays of both feet showing that there is no tarsal coalition. (E) AP standing view revealing talonavicular uncoverage in both feet. (F) Lateral standing view showing talar declination in both feet (images were taken at orthopedic surgery outpatient clinic of Kasr al Ainy Hospital).
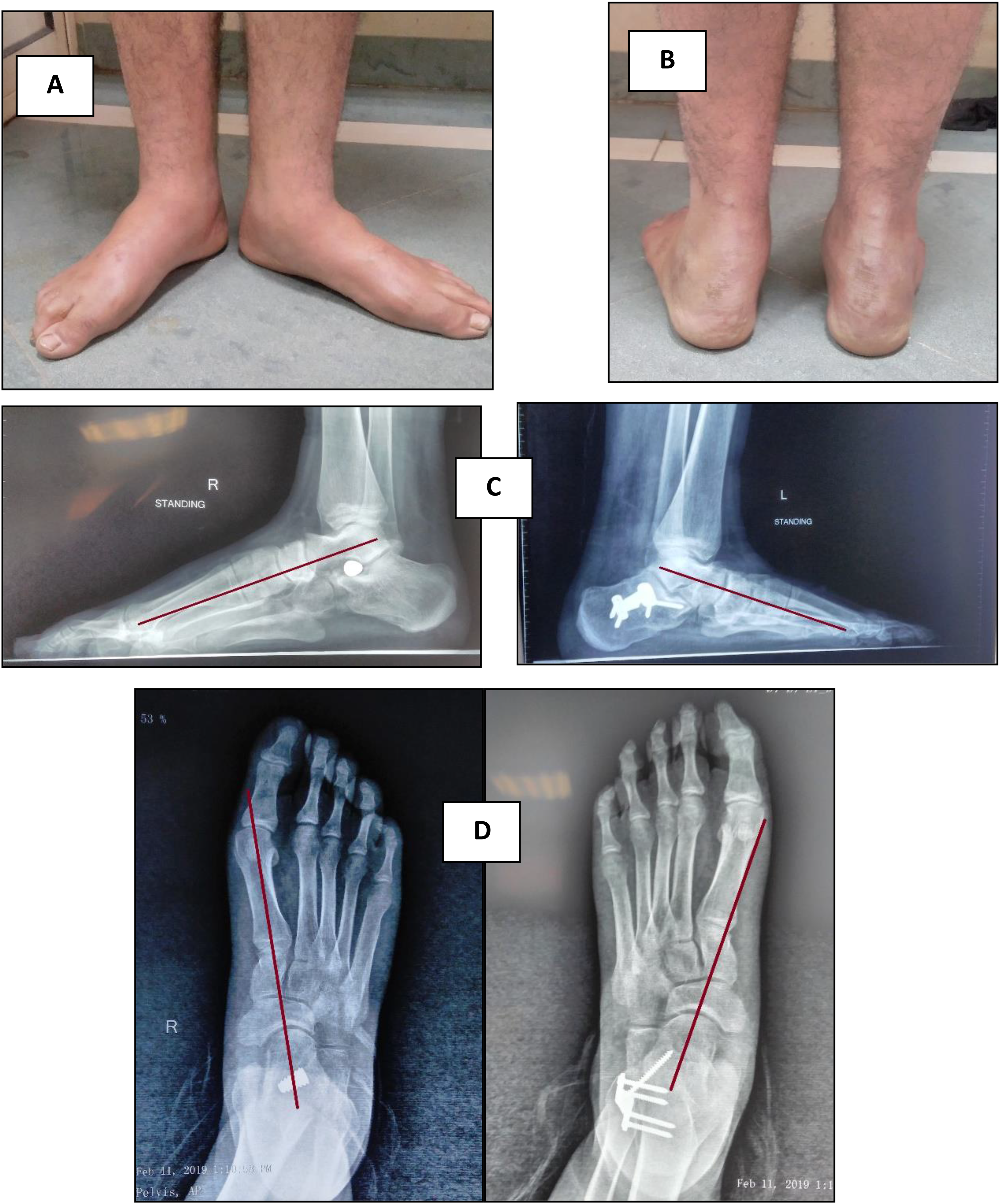
Postoperative clinical and radiological results at 3rd month postoperatively in an 18 years old male undergone MDCO in LT foot and arthroereisis in RT foot. (A) Frontal foot view of both feet revealing restored medial longitudinal feet arches. (B) Rear feet view showing restored neutral alignment of both heels (C and D) wound healed without any complications. (E) Lateral standing view showing improvement of talar declination in both feet. (F) AP standing view revealing improvement of talonavicular coverage in both feet (images were taken at orthopedic surgery outpatient clinic of Kasr al Ainy Hospital).
Postoperative clinical and radiological results at 6th month postoperatively in an 18 years old male undergone MDCO in LT foot and arthroereisis in RT foot. (A) Frontal foot view of both feet revealing maintained improvement of medial longitudinal feet arches. (B) Rear feet view showing maintained neutral alignment of both heels. (C) Lateral standing view showing maintained improvement of talar declination in both feet. (D) AP standing view revealing maintained improvement of talonavicular coverage in both feet (images were taken at orthopedic surgery outpatient clinic of Kasr al Ainy Hospital).
American Orthopaedic Foot and Ankle Society score
About the 3rd month of follow-up both groups showed improvement in their AOFAS scores where the arthroereisis group mean score was improved from 50.6% preoperatively to 85.9% postoperatively, while the MDCO group showed a shift from 50.76% to 85.59%; the one-tailed student t-test showed significant improvement in both groups with a “p-value less than 0.00001” (significant at p < 0.05) for the arthroereisis group and a p-value less than 0.00001” for the MDCO group while the two-tailed student t-test showed non-significant difference between both groups with a “p-value of 0.91.”
In the 6th month of follow-up, both groups’ AOFAS scores were improved when comparing it to the 3rd month, where the arthroereisis group mean score was shifted from 85.9% to 88%, and the MDCO group was improved from 85.59% to 87.65%; the one-tailed student t-test done for the arthroereisis group showed significant improvement with a “p-value of 0.001,” although the test for MDCO group showed significant improvement with a “p-value of 0.002” (significant at p < 0.05), while the two-tailed student t-test showed non-significant difference with a “p-value of 0.91.”
Foot Functional Index
About the 3rd month of follow-up, both groups showed improvement in their FFI scores where the mean FFI score of the arthroereisis group was improved from 39% preoperatively to 5.3% postoperatively while the MDCO group showed a shift from 39% to 5.71%; the one-tailed student t-test showed significant improvement in both groups with a “p-value less than 0.00001” (significant at p < 0.05) for the arthroereisis group and “p-value less than 0.00001” for the MDCO group while the two-tailed student t-test showed non-significant difference between both groups with a “p-value of 0.89.”
In the 6th month of follow-up, both groups’ FFI scores were improved when comparing it to the 3rd month, where the arthroereisis group mean FFI score was shifted from 5.3% to 5.05%, and the MDCO group was improved from 5.82% to 5.41%; the one-tailed student t-test done to compare between the 3rd & 6th-month FFI scores for the arthroereisis group showed significant improvement with a “p-value of 0.0105”; although the test done for MDCO group showed significant improvement with a “p-value of 0.01” (significant at p < 0.05), while the two-tailed student t-test showed non-significant difference with a “p-value of 0.90.”
Radiological results
AP talo first metatarsal angle
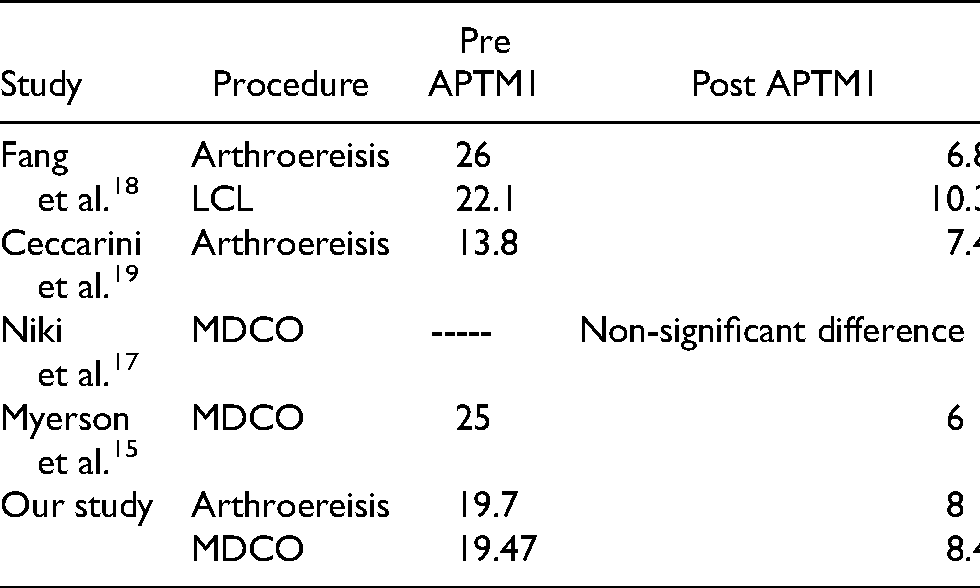
Both groups showed improvement in their AP talo first metatarsal angle at 3rd month of follow-up where the arthroereisis group mean APTM1 angle was improved from 19.7° preoperatively to 7.9° postoperatively while the MDCO group showed a shift from 19.47° to 8.3°; the one-tailed student t-test showed significant improvement in both groups with a “p-value less than 0.00001” (significant at p < 0.05) for the arthroereisis group and p-value less than 0.00001” for the MDCO group, while the two-tailed student t-test showed non-significant difference between both groups with a “p-value of 0 .84.”
After 6 months follow-up, the arthroereisis group mean APTM1 angle was shifted from 7.9° at 3rd month to 8°, and the MDCO group was shifted from 8.3° to 8.4°; the one-tailed student t-test was done to compare between the 3rd month & the 6th month APTM1 angle for the arthroereisis group showed non-significant shift with a “p-value of 0.25”; although the test done for MDCO group showed non-significant shift with a “p-value of 0.27” (significant at p < 0.05), while the two-tailed student t-test showed non-significant difference with a “p-value of 0.83.”
Antero posterior talo calcaneal angle
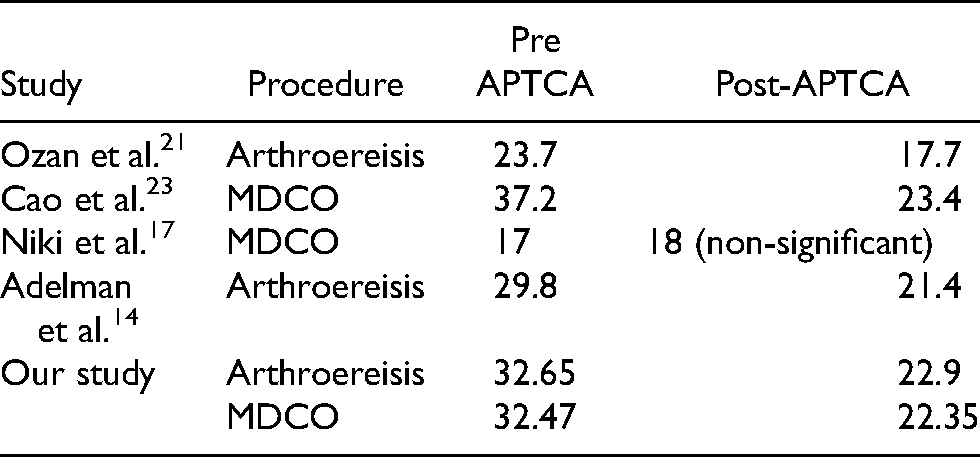
Both groups showed improvement in their APTCA at 3rd month of follow-up where the arthroereisis group mean APTCA was improved from 32.65° preoperatively to 22.8° postoperatively while the MDCO group showed a shift from 32.47° to 22.58°; the one-tailed student t-test showed significant improvement in both groups with a “p-value less than 0.00001” (significant at p < 0.05) for the arthroereisis group and “p-value less than 0.00001” for the MDCO group, while the two-tailed student t-test showed non-significant difference with a “p-value of 0 .83.”
After 6 months follow-up, the arthroereisis group mean APTCA was shifted from 22.8° at 3rd month to 22.9°, and the MDCO group was shifted from 22.58° to 22.35°; the one-tailed student t-test was done to compare between the 3rd month and the 6th-month APTCA for the arthroereisis group showed non-significant shift with a “p-value of 0.16,”, although the test done for MDCO group showed non-significant shift with a “p-value of 0.08” (significant at p < 0.05), while the two-tailed student t-test showed non-significant difference with a “p-value of 0.76,”
Lateral talocalcaneal angle
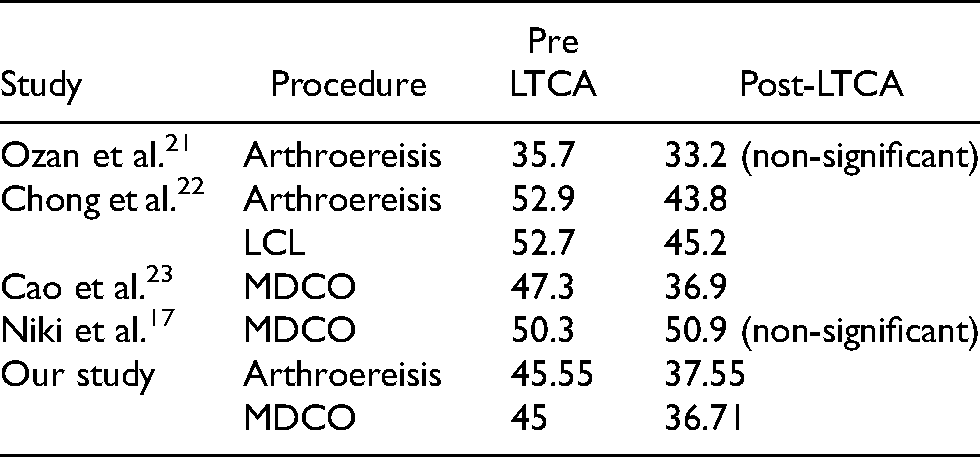
Both groups showed improvement in their LTCA at 3rd month of follow-up where the arthroereisis group mean LTCA was improved from 45.55° preoperatively to 37.65° postoperatively while the MDCO group showed a shift from 45 to 36.88°; the one-tailed student t-test showed significant improvement in both groups LTCA with a “p-value less than 0.00001” (significant at p < 0.05) for the arthroereisis group and p-value less than 0.00001” for the MDCO group; the two-tailed student t-test showed non-significant difference with a “p-value of 0.39.”
After 6 months follow-up, the arthroereisis group mean LTCA was shifted from 37.65° at 3rd month to 37.55°, and the MDCO group was shifted from 36.88° to 36.71°; the one-tailed student t-test was done to compare between the 3rd month & the 6th-month LTCA for the arthroereisis group showed non-significant shift with a “p-value of 0.31”; although the test done for MDCO group showed non-significant shift with a “p-value of 0.21” (significant at p < 0.05), while the two-tailed student t-test showed non-significant difference with a “p-value of 0.30.”
Calcaneal inclination angle
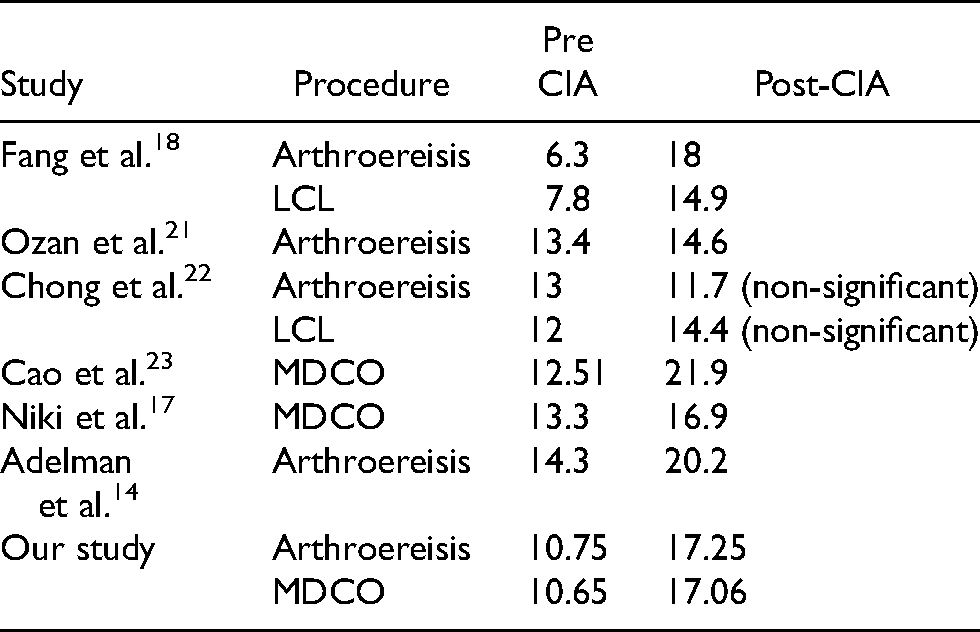
Both groups showed improvement in their CIA at 3rd month of follow-up where the arthroereisis group mean CIA was improved from 10.75° preoperatively to 17.2° postoperatively while the MDCO group showed a shift from 10.65° to 16.94°; the one-tailed student t-test showed significant improvement in both groups with a “p-value less than 0.00001” (significant at p < 0.05) for the arthroereisis group and p-value less than 0.00001” for the MDCO group, while the two-tailed student t-test showed non-significant difference with a “p-value of 0.77.”
After 6 months follow-up, the arthroereisis group mean CIA was shifted from 17.2° at 3rd month to 17.25° & the MDCO group was shifted from 16.94° to 17.06°; the one-tailed student t-test was done to compare between the 3rd month & the 6th month CIA for the arthroereisis group showed non-significant shift with a “p-value of 0.39,” although the test done for MDCO group showed non-significant shift with a “p-value of 0.08” (significant at p < 0.05), while the two-tailed student t-test showed non-significant difference with a “p-value of 0.85.”
Complications
The overall complication rate in our study was 16.2% that was encountered in 6 feet, arthroereisis complications representing 20% (4 feet out of 20 feet) while MDCO complications representing 11.76% (2 feet out of 17 feet); superficial infection was encountered in 2 feet within the MDCO group; that was managed by doing culture and sensitivity test for the wound discharge then prober antibiotics were given for 3 weeks after which superficial infection was resolved and the patients did well clinically and radiographically at subsequent follow-up; sinus tarsi pain was encountered within the subtalar arthroereisis group in 3 feet and this complication was managed by implant removal at 8 months after surgery, without change in their clinical or radiological parameters, with improvement of their pain after surgery; the other complication was implant progression within sinus tarsi in one foot only that was encountered in first follow-up after surgery because the implant size was too small and revision surgery was done with another implant of bigger size placed instead after which patient did well clinically and radiographically at subsequent follow-up; only one patient with bilateral flexible flat feet undergone arthroereisis in one side and MDCO in the other side did not show any clinical or radiological improvement at subsequent follow-up and patient was asked for revision surgery but patient refused to do so and we did not include it as a complication.
Discussion
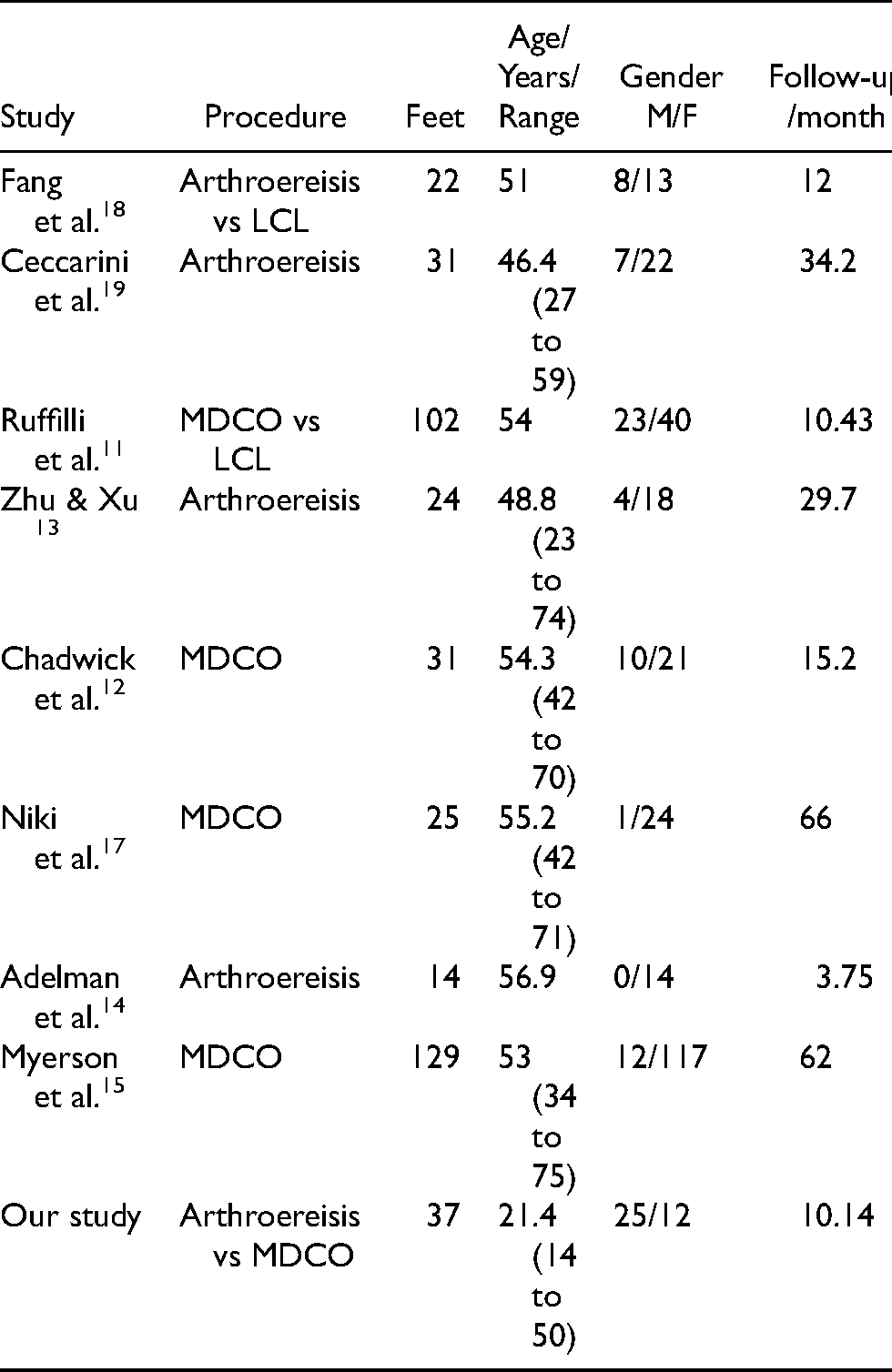
The demographic data in our series represented in sample size was comparable to other series while the mean follow-up period was shorter than that of other series; gender distribution revealed more males, unlike other series where females were more (Table 1).
Demographic data comparison with other series (sample size, mean age, gender, mean follow-up).
Adjunctive procedures within the MDCO group in our study were FDL transfer in 9 feet while both FDL transfer and TAL in 2 feet, unlike arthroereisis group in which TAL was done in 2 feet, although we did not find any significant difference in postoperative clinical and radiological scores between patients undergone soft tissue procedure combined with arthroereisis or MDCO and patient undergone either arthroereisis or MDCO alone.
Ruffilli et al. evaluated surgical treatment of stage II posterior tibialis tendon (PTT) dysfunction; the results obtained in this case series encourage the reparation of the degenerated tibialis posterior tendon when the healthy portion is more than 50% of tendon area and in the absence of significant tendon elongation otherwise FDL transfer should be adopted, associated bony procedures are mandatory in the presence of grade II PTTD to restore correct stance and to protect tendon repair. 11
Chadwick et al.’s long-term follow-up adjunctive procedures included FDL transfer beside the MDCO in all patients which provided long-term pain relief and satisfactory functional outcome in the management of stage II posterior tibial tendon dysfunction. 12
Zhu & Xu aimed to evaluate the outcome of subtalar arthrodesis in treating stage II Adult-Acquired Flatfoot (AAFD); the conclusion was that subtalar arthroereisis alone or combined with other soft-tissue or osseous procedures appears to be a reasonable treatment option for AAFD stage IIA and IIC, subtalar arthroereisis alone can be used to correct mild hindfoot valgus, and it can be an alternative to calcaneal osteotomy. 13
The retrospective study was done by Adelman et al. in 2008 radiographically evaluated endoscopic TAL, subtalar joint arthroereisis, and FDL transfer for surgical correction of stage II posterior tibial tendon dysfunction and found that combination of these procedures significantly improved the radiographic variables. 14
Myerson et al. studied treatment of stage II posterior tibial tendon deficiency with MDCO and the adjunctive procedure in all patients (129 feet) was FDL transfer, the combination of both yielded excellent results with a high patient satisfaction rate. 15
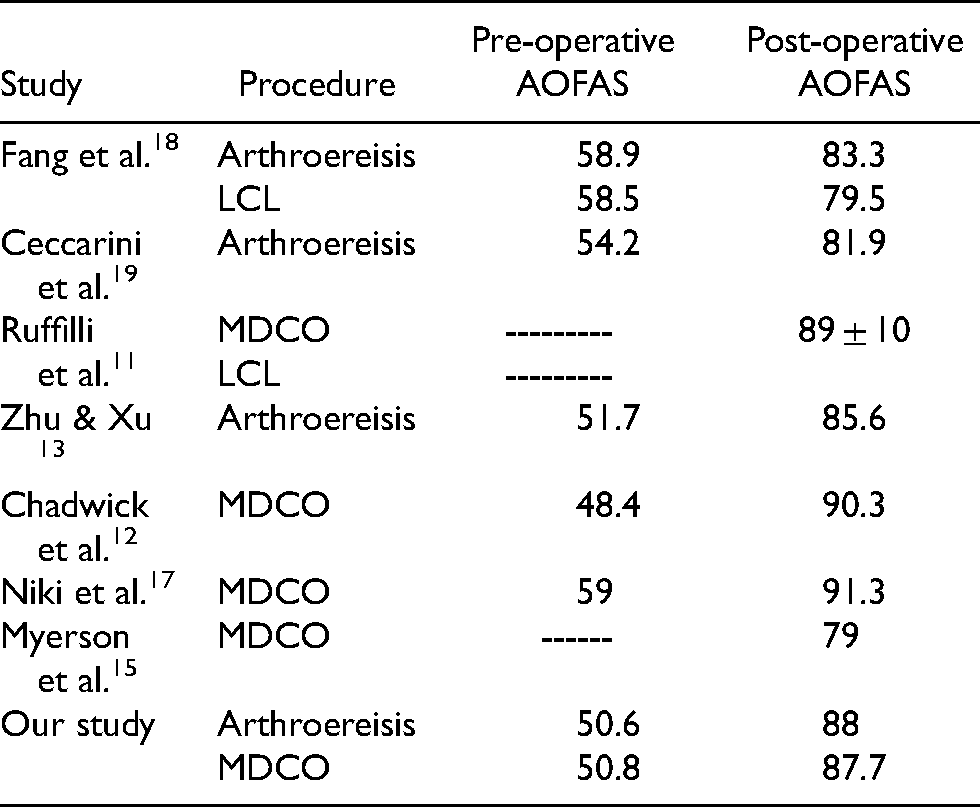
About the 3rd and 6th months of follow-up, both groups in our study showed improvement in their AOFAS scores & FFI scores, those results were comparable to other series (Table 2).
Mean AOFAS scores compared with other series.
Faldini et al. studied outcomes after subtalar arthroereisis with bioabsorbable implants for flexible flatfoot in growing age and found excellent results with an average FFI score of 4.5; out of 173 patients, 4 needed a second surgery for removing the implant. 16
Niki et al. retrospective study evaluated MDCO for correction of AAFD and there was an improvement in the mean FFI scores from 75 to 9. 17
Regarding radiological outcome, both groups in our study showed improvement in their APTM1, APTCA, LTCA, CIA at the 3rd and 6th months of follow-up and those results were comparable to other series (Tables 3–6).
Mean APTM1 comparison with other series.
Mean APTCA comparison with other series.
Mean LTCA comparison with other series.
Mean CIA comparison with other series.
The overall complication rate in our study was 16.2% that was encountered in 6 feet, MDCO complications representing 11.76% while arthroereisis complications representing 20%, superficial infection was encountered in 2 feet within the MDCO group; sinus tarsi pain was encountered within the subtalar arthroereisis group in 3 feet; the other complication was implant progression within sinus tarsi that was encountered in first follow-up after surgery because the implant size was too small; only one patient with bilateral flexible flat feet undergone arthroereisis in one side and MDCO in the other did not show any clinical or radiological improvement at subsequent follow-up and we did not include it as a complication.
In the study done by Fang et al. that compared arthroereisis and Evans osteotomy, six patients complained of sinus tarsi pain with four patients requiring implant removal in the SA group at a mean of 27 months postoperatively. 18
Ceccarini et al. studied the arthroereisis procedure in adult flexible flatfoot, pain in the tarsal sinus was reported in 5 out of 29 (16.1%) feet for the first three months after surgery, which was resolved within 6 months by physical therapy, 3 of 29 (10.34%) patients removed the arthroereisis. 19
Saxena et al.’s prospective study evaluated subtalar arthroereisis implant removal in 100 adults, no significant difference was found in the incidence of removal according to patient age or endoscopic gastrocnemius recession. 20
Conclusion
In our prospective randomized double center study that was done for comparing arthroereisis utilizing the subtalar implant with MDCO utilizing the modified step plate for management of flexible pes planus, we have found that both methods significantly improved radiographic and subjective clinical outcome measures without any significant differences between the outcomes which suggest that both methods provide an appropriate solution in the management of symptomatic flexible flat feet in children & adults but the less-invasive nature, lower potential morbidity, and rapid recovery suggest that judicious use of arthroereisis is more appropriate; but unfortunately, we have relatively small sample size & short follow-up period so we were unable to warranty the maintenance of improvements.
Recommendations
Further studies with more patients & long-term follow-up should be warranted to demonstrate the efficacy of both methods in maintaining functional & radiological improvements; reducing age gab, doing procedures unilaterally and by the same surgeon will reduce any bias. Furthermore, patients with bilateral and different procedure stated that they would rather prefer to do single procedure at instance in order to facilitate ambulation, also they recommend arthroereisis over MDCO due to faster recovery and ambulation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.