
Abstract
Keywords
Introduction
The incidence of anterior glenohumeral instability is around 21.9 dislocations per 100000 individuals per year in developing countries. 1 The most common dislocated synovial joint of the human body is glenohumeral joint. Generally, “forced abduction and external rotation” is the mechanism of injury. It is common among young males involved in activities such as cricket, weight lifting, heavy labor work, and gym training. In developing countries, these patients present at later stages with significant glenoid bone loss. In India, for the first time of the dislocation, patient visits local bonesetters and generally presents to orthopedic surgeons after a long period. In which, with frequent and further instances of dislocation, there is markedly alteration and disturbance in normal anatomy of the humeral head, the glenoid rim, capsule, surrounding ligaments, and the labrum. 2 Anatomical repairs, for example, Bankart repair aim at stitching the torn glenoid labrum back to its position over glenoid rim. Isolated capsulolabral arthroscopic repair is advised for the treatment of glenohumeral instability with glenoid bone loss of less than 15–20% but with glonoid bone loss exceeding 20–25% non-anatomic procedure like bone transfer surgeries is recommended,3,4 which works on the principle of an active muscular sling with the coracoid transfer. The latarjet procedure involves the transfer of the coracoid process along with the attached conjoined tendon to anteroinferior glenoid. De Beer's modification to this classic technique is termed the congruent-Arc Laterjet, This technique involves rotating the coracoid graft 90° about its longitudinal axis and transferring it such that the inferior surface reconstitutes the glenoid articulation. 5 This alteration was originally advocated due to the observation that the inferior curvature of the coracoid would result in improved glenohumeral congruity and thus stability. The aim of the study is to analyze the functional outcome of Congruent Arc Latarjet Procedure in recurrent anterior shoulder dislocation with glenohumeral instability and analyze its outcomes.
Materials and method
This retrospective single case-series study level IV includes 20 patients operated at SVPIMSR hospital, Ahmedabad from January 2018 to November 2021 with their informed consent. Inclusion criteria for our study were osseous Bankart's lesion with glenoid bone loss >20%, recurrent shoulder instability after surgery, and ISIS (International Shoulder Instability Score) greater than or equal to 6. Exclusion criteria were fracture-dislocation, congenital ligament laxity, neuromuscular disorders, with concurrent Hill-Sachs lesion, ISIS less than 6, acromioclavicular dislocation, distal clavicle fracture, or other scapular fractures (except osseous Bankart lesions), and patients with neurovascular injury. The radiographic evaluation was done based on X-ray (Antero-posterior, lateral, scapular Y, and axillary views), preoperative CT scan with 3-dimensional (3D) reconstruction. The glenoid bone loss was assessed on the en-face view of the 3D reconstruction as described by Chuang et al. by PICO method. 6 All patients were operated with Congruent Arc Latarjet procedure with beach chair position by the deltopectoral approach by the senior author. They were evaluated postoperatively at the following intervals 1 month, 3 months, 6 months, 12 months, and 24 months. The evaluation was done on the basis visual analog scale (VAS) pain score, Active Range of motion (Forward elevation, External rotation, and Internal rotation), American Shoulder and Elbow Surgeons (ASES) score, and (ROWE) score and Postoperative CT scan at 6 months to assess graft union and screw-related complications. For statistical analysis, to analyze the functional outcome of Congruent Arc latarjet procedure paired t-test was used in these patients. This test is used to analyze the differences before and after the surgical procedure. The significance level was set at p < 0.05. SPSS software is used for statistical analysis.
All surgical procedures were performed by our senior author. The patients underwent general anesthesia and were given beach-chair position with headrest and enough pads kept overall bony prominences. Preparation and draping were done of the affected shoulder in a sterile fashion. The marking of the surface anatomy is done. A standard deltopectoral approach was taken (Figure 1(a)). The coracoid was identified and Coracoacromial ligament (CAL) is cut at midway to preserve the stump of it which can be used to enhance the repair. From the medial aspect of the coracoid process, Pectoralis minor tendon is released. A medial-to-lateral osteotomy was performed at the base of the coracoid. The coracoid graft is grasped with forceps and coracohumeral ligament is released (Figure 1(b)). The medial surface is further rasped till the cancellous surface is seen. During graft preparation, preserve coracoacromial ligament stump and conjoint tendon insertion as it provides blood supply to the coracoid graft. The subscapularis muscle is made under tension by external rotation and the plane is created along with fibers by splitting at superior ⅔ and inferior ⅓ junctions (Figure 1(c)). Capsulotomy was done. Anteroinferior glenoid labrum was dissected subperiosteally and neck of the glenoid was freshened as a further bed for bone placement. Using the Fukuda retractor, the glenohumeral joint is exposed. The coracoid graft is rotated 90° laterally and the longitudinal axis of the coracoid graft is aligned superoinferiorly along with the 3-'o' and 5-'o' clock position of the articular surface of the glenoid neck so that the curved inferior surface is congruent to the anteroinferior part of glenoid and medial surface acts as a bone bed for fusion (Figure 1(d)). Although placing graft with taking care that graft is not too medial or too lateral to the glenoid rim. Definitive screw fixation is performed using partially threaded two 3.5 mm cannulated screws following the principle of lag technique (Figure 1(e)). Further, the remaining part of the coracoacromial ligament attached to the coracoid process is sutured along with the capsule which further increases the strength of the capsule. A schematic diagram showing the difference between classical and congruent arc latarjet included (Figure 2). Mobility was checked and closure was done in all layers. After the operation, a shoulder immobilizer is given with wrist and finger mobilization immediately for two weeks followed by elbow mobilization for the next two weeks. After four weeks, active shoulder range of motion exercises and Codman pendulum exercises was initiated.
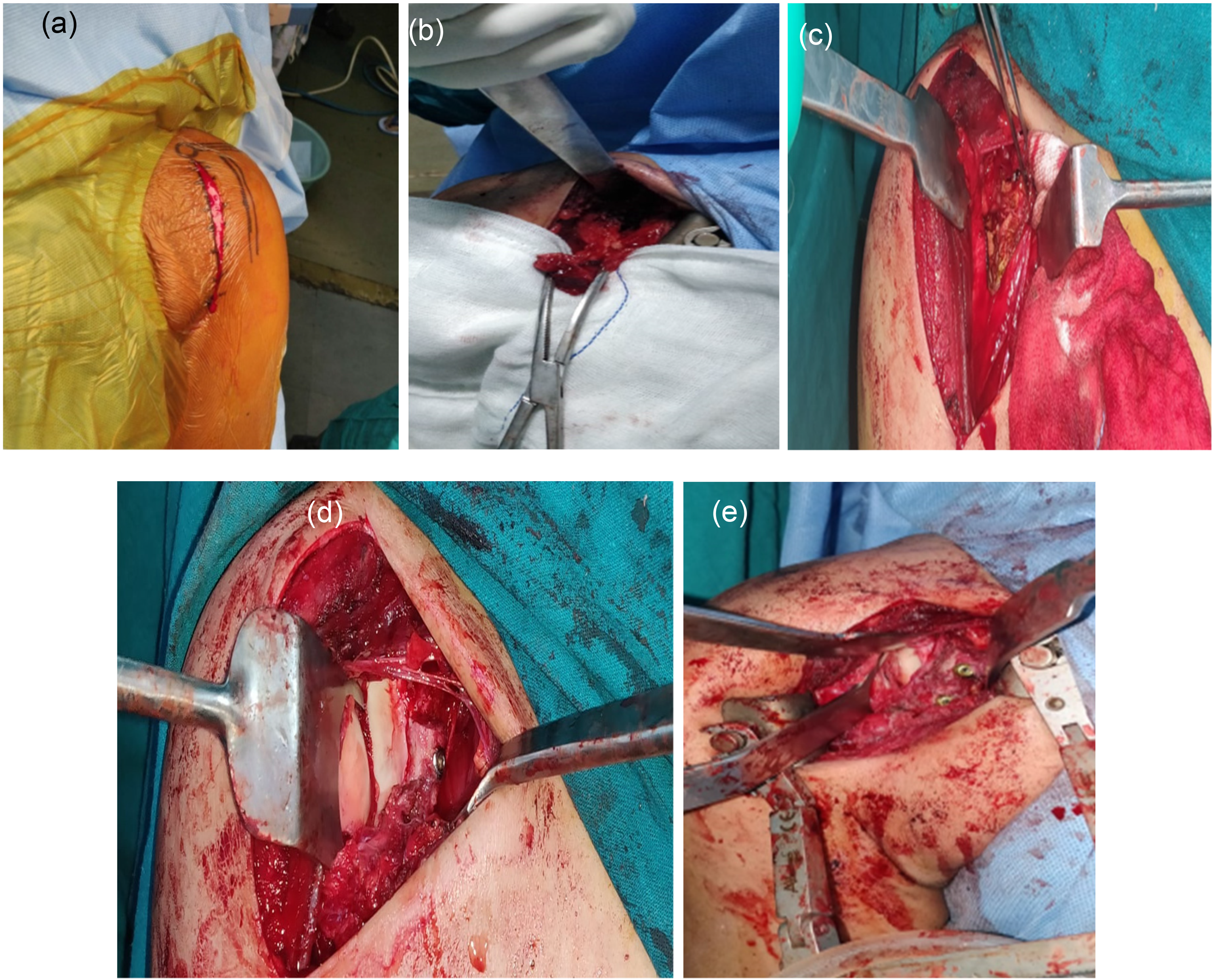
(a) Skin reference markings for the deltopectoral approach. (b) Coracoid osteotomy with preservation of coracoacromial ligament. (c) Glenoid preparation and exposure by subscapularis splitting technique. (d) Coracoid bone with inferior surface parallel to glenoid (congruent arc) fixation using 3.5 cc screws restoring the anatomic surface. (e) Two 3.5 cannulated cancellous screw used.
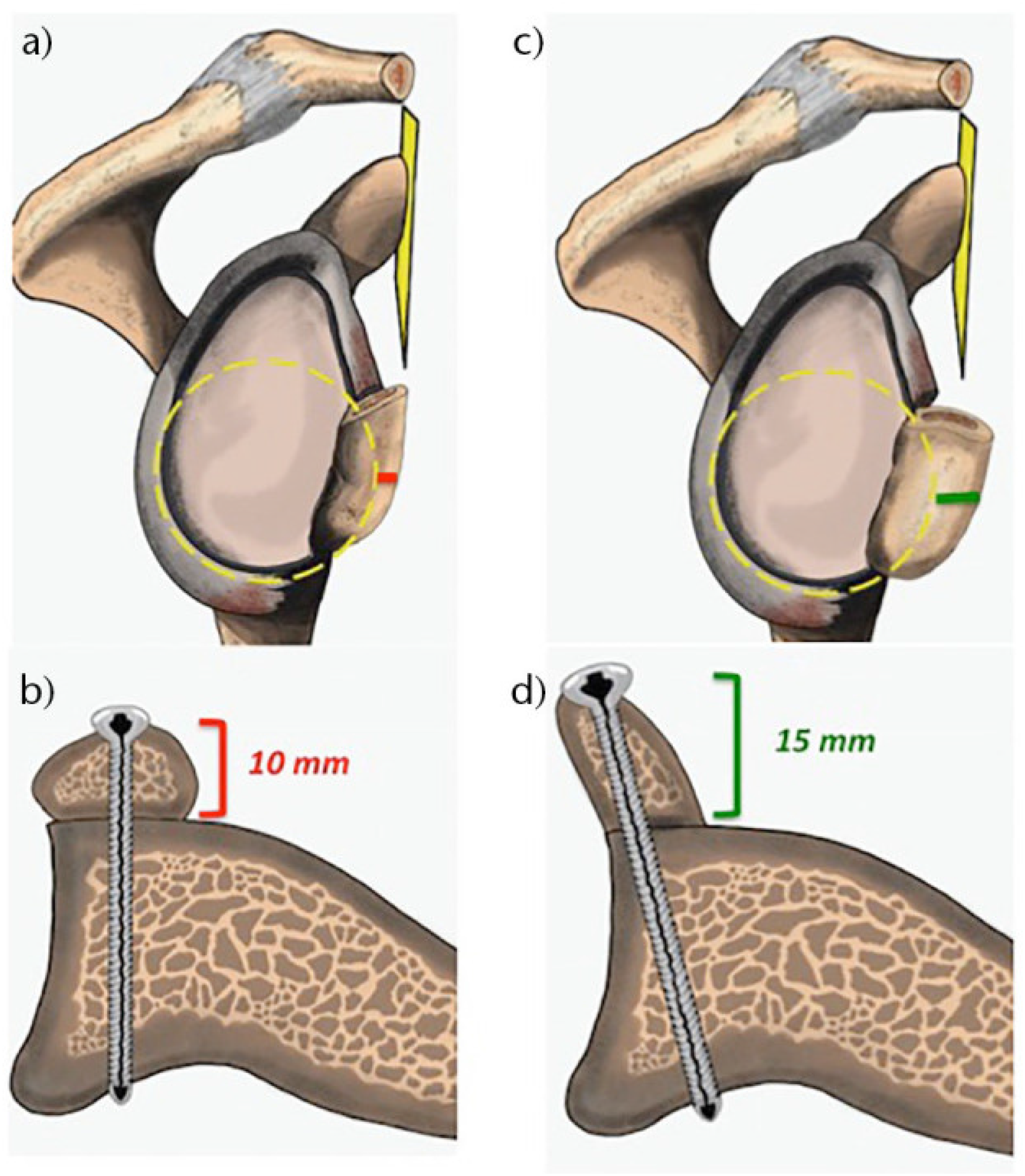
Glenoid bone reconstruction. (a) Sagittal and (b) coronal images of the traditional latarjet (TL). (c) Sagittal and (d) coronal images of the congruent-arc latarjet.
Results
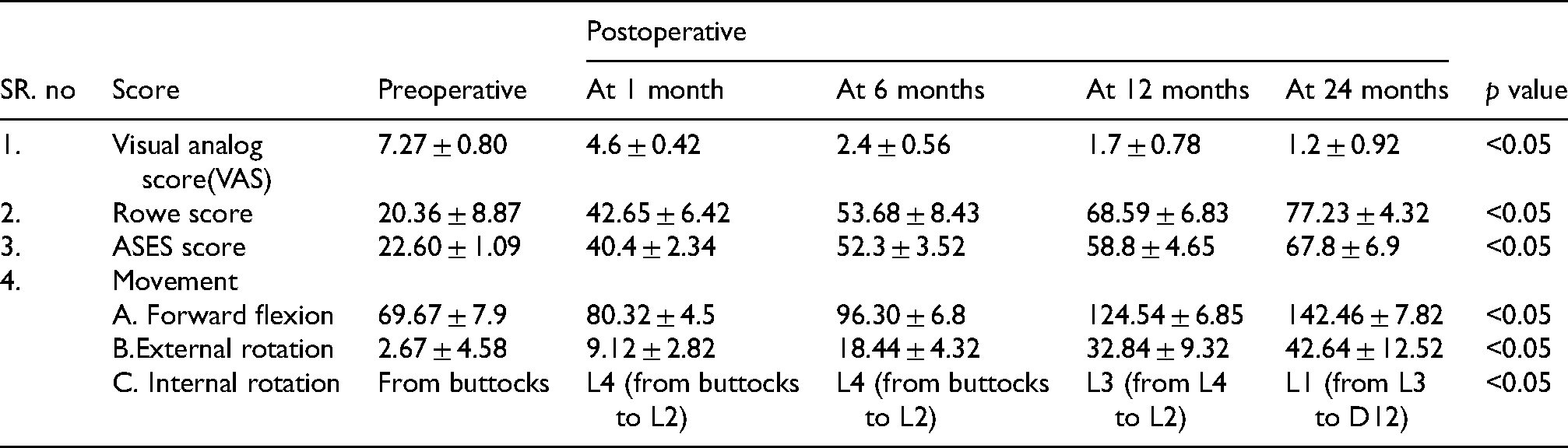
All 20 patients had a solid bone union at six months on CT scan. In our study, all 20 patients were followed up for 24 months, and no patient was lost to follow-up. There were 14 males and 6 females in the group. There were 10 patients in the age group 20–30, 8 patients in the age group 30–40, and 2 patients in the age group above 40. One patient had a family history of recurrent shoulder dislocations.6 patients had their first episode while engaging in sports activities. Nine patients had their first episode in accidents occurring while engaged in manual labor. Five patients had their first episode in road traffic accidents or household falls. At the time of the 24-month follow-up, mean visual analog score decreased from 7.27 ± 0.80 to 0.80 ± 1.15, p = 0.001, the range of motion as mentioned in Table 1, and the shoulder functional evaluations based on ROWE score which was 89.64 ± 5.71 (range 80–95) improved to 20.36 ± 8.87 (range 10–30), p = 0.001. The mean preoperative ASES score was 22.60 ± 1.09 (range 20.6–25) which improved to 72.50 ± 7.33 (range 52.8–77.2), p = 0.001, which is significantly improved. The overall re-dislocation or subluxation rate was 0% (0 of 20). In our study, 60% had excellent outcomes, 30% had good outcomes and 10% had fair outcomes on the basis of ROWE scores. Three of the patients had joint stiffness, ROWE score of 80 each, with further aggressive physiotherapy and passive range of motion exercises score improved to 85 which is a good outcome. During the first 10 months, there is an average loss of external rotation by 25° compared to the normal contralateral shoulder. One of the patients had distal screw loosening due to osteolysis, which was removed after one year once the bony union was confirmed on a follow-up CT scan. All patients have reported back to routine work after six months period.
Results.
Discussion
Normal glenoid becomes like bitten pear shape when bony Bankart lesion with bone loss greater than 20–25% of joint surface area occurs due to repeated anterior shoulder dislocation where the superior diameter is greater than inferior diameter.7,8 When looking at the anatomy of the coracoid, the radius of curvature of its inferior surface is congruent to that of the articulating surface of the glenoid. In the classic latarjet technique, after coracoid osteotomy, it is fixed to anteroinferior surface of the glenoid where the inferior surface of the coracoid is the bone fusion site. There is a markable difference in curvature of the radius between the inferior aspect of the coracoid process and the anteroinferior surface of the pathological glenoid for which the inferior surface of the coracoid has to be decorticated enough to make it congruent with the anterior aspect of the pathological glenoid for bony fusion.9–12 Therefore, when a large amount of decortication is needed for achieving a congruent surface it always comes with the risk of fracture, and the chances of proximal osteolysis are increased. As per de beer et al., 5 modifying the classic Latarjet procedure by rotating the coracoid by 90° about its longitudinal axis such that its inferior surface becomes parallel to the joint surface of the glenoid and medial surface of the coracoid process becomes the bone bed for fusion without the need of a large amount of decortication of flat medial surface for enabling bone fusion. This technique indeed helps in preserving bone stock of the graft, which is one of its biggest advantages. There are some hazards with this technique. First, when coracoid process is exposed for osteotomy it is advisable to be on the lateral side of the conjoint tendon to avoid the risk of musculocutaneous nerve lesion. Also, there is an increased chance of musculocutaneous nerve lesion when coracoid process is rotated laterally outside by 90° in modified latarjet technique.13–16 Second, there is a loss of some degrees of external rotation compared to contralateral healthy shoulder because of impingement between the subscapularis tendon and the coracoid bone block.17 Third, for fixation of the bone block when drilling is done along with lateral to medial surface of the coracoid which has less width that requires utmost care, precision and expertise to avoid the risk of fracture of the graft.
In our present series, 18 out of 20 patients had excellent to a good outcome. There was no history of re-dislocation in any of the patients. Among complications, we had no musculocutaneous nerve lesion in any of the patient. There was a mean loss of 25° of external rotation compared to contralateral shoulder. With the great precision and expertise of senior author, there was no incidence of graft fracture while tunnel drilling. One of the patients had distal screw loosening due to osteolysis, which was removed after one year once the bony union was confirmed on a follow-up CT scan.
The limitation of this study is a small sample size. It is a single-center case series, and there is no head-to-head comparison between classic Latarjet surgeries. Our mean follow-up is 24 months and only longer follow-up can tell whether congruent arc Latarjet has advantages over Classic Latarjet in the development of shoulder osteoarthritis. Our study population did not have professional sportspersons, especially those in contact sports. The functional demand of these patients may be different from our study population.
Conclusion
Our study results show that Congruent Arc Latarjet procedure effectively restores joint stability in recurrent shoulder dislocation with glenoid bone deficiency of >20%. They were found to have a low rate of persistent glenohumeral instability, redislocation, or subluxation limited shoulder range of motion and early onset of glenohumeral osteoarthritis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.