
Abstract
Background
The most common complication in the surgery for rotator cuff (RC) tears is postoperative shoulder stiffness. The evidence for the postoperative treatment of this condition is scarce. This study assessed the effects of a postoperative program at the onset of shoulder stiffness following arthroscopic RC repair.
Methods
A single-group pre- and post-test design was included. Participants performed a 6-week program. Primary outcomes were shoulder and upper limb function assessed with the Constant–Murley and Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaires, respectively. Secondary outcomes included pain intensity at rest and during movement with the visual analog scale (VAS), and shoulder range of motion assessed with a goniometer.
Results
A total of 115 adult males were included. The intervention produced a positive effect on the Constant–Murley (+35.6 points, p<0.001) and DASH questionnaire (−26.2 points, p = 0.005); VAS at rest (−2.8 cm, p<0.001); VAS at movement (−2.7 cm, p<0.001); and shoulder ROMs.
Conclusion
The program showed clinically and statistically significant benefits in most of the functional outcomes in the study participants.
Keywords
Introduction
Rotator cuff (RC) disease is the most common etiology of shoulder pain and is responsible for up to 70% of all shoulder-related visits to physicians. 1 The prevalence of RC tears increases with age, from 9.7% in patients <20 years old to 62% in patients over 80 years old. These rates are increased in symptomatic patients and after shoulder dislocation. 2 Despite this widespread prevalence in the general population, optimal management remains controversial. 3
Surgery for RC tears is usually performed after conservative treatment has not been effective. 4 Surgical options include partial repair and/or debridement, repair (open or arthroscopic), reconstruction (muscle transfer or processed tissue), and arthroplasty (hemi or reverse shoulder). 5 According to the preferences of patients, available resources, training, and surgeon’s surgical experience, these procedures can be performed in an open, mini-open, or all-arthroscopic RC repair.4,5 Widespread use of arthroscopy has been related to a significant increase in RC repair procedures, and currently, arthroscopic repair has replaced open surgery and is now used to treat more than 95% of all RC tears. 6 Despite this, postoperative shoulder stiffness is the main complication of arthroscopic RC repair. 7
Shoulder stiffness is a condition of a restricted glenohumeral range of motion (ROM), which can arise spontaneously (primary or idiopathic shoulder stiffness, also known as “frozen shoulder”) or as a consequence of a known cause, including surgical procedures on the shoulder (secondary and postoperative shoulder stiffness). 8 The rate of postoperative shoulder stiffness following arthroscopic RC repair is variable due to the heterogeneity of diagnostic criteria and is reported to be from 2.3% to 28.5%.8,9 Preoperative risk factors for developing shoulder stiffness following arthroscopic RC repair may include preoperative shoulder stiffness, age <50 years old, workers’ compensation, diabetes, hypothyroidism, calcific tendonitis, or adhesive capsulitis. 9 Other intraoperative risk factors include single-tendon tears, partial articular-sided tears, and concomitant labral repair. 8
Patients with postoperative shoulder stiffness are characterized by spontaneous onset of pain with significant restriction of both active and passive shoulder ROM, which is associated with kinematics alterations in the glenohumeral and scapulohumeral joints. A systematic review concluded that the effective treatment for this condition remains unclear. 10 Despite this, different therapeutic interventions have been used, including non-steroidal anti-inflammatory medications, corticosteroid injections, postoperative interventions (exercise plus other physical therapies, such as joint mobilization or transcutaneous electrical nerve stimulation), manipulation under anesthesia, and arthroscopic capsular release. 10
A staged approach to the rehabilitation of shoulder disorders has been recommended based on symptoms of irritability combined with pathoanatomic considerations to diagnose and treat these patients. 11 The concept of irritability reflects the ability of tissues to handle physical stress and theoretically relates to its physical status and the degree of inflammatory activity present. 11 A classification of irritability was proposed by a consensus of experts using pain levels, the relationship between pain and motion, and self-report of disability. 12 Therefore, postoperative programs should be based on the stage of tissue irritability to guide the intensity of treatment, and impairments are used to guide the selection of the therapeutic interventions that are used.
To our knowledge, no previous study has reported the effects of a postoperative program considering the level of irritability in patients with shoulder stiffness. Accordingly, the aim of the present study was to assess the effects of a 6-week postoperative program on functional outcomes in patients with shoulder stiffness with low to moderate irritability following arthroscopic RC repair. We hypothesized that a postoperative program would improve shoulder and upper limb function, shoulder motion, and pain relief in these patients.
Methods
Study design and participants
A single-group pre- and post-test observational design was approved by the Ethics Committee of the Central Metropolitan Health Service of Chile (no. 18/2016). Between February 2016 and February 2020, 115 patients with shoulder stiffness after RC repair were prospectively recruited. All patients who had a full-thickness supraspinatus tear, stage 2 or less fatty infiltration, and mild or no muscle atrophy that was confirmed by preoperative ultrasound and magnetic resonance imaging were repaired arthroscopically with single row sutures. Postoperative shoulder stiffness was considered if forward flexion was <110°, external rotation with the arm at the side was <25° or internal rotation was below the second sacral vertebral level. 13 All patients were treated with postoperative immobilization with a sling and 500 mg of naproxen orally twice daily for 14 days; at 6 weeks after surgery, they were referred to physical therapy. All subjects were informed about the procedure and gave their written consent to participate.
The inclusion criteria for participants were (i) being older than 18 years old with shoulder stiffness and low to moderate irritability (Supplemental Table S1) following arthroscopic repair of a non-retracted isolated full-thickness supraspinatus tear. Conversely, patients were excluded if they met the following criteria: (i) having a massive or irreparable RC tear; (ii) anteroinferior labral (Bankart) or superior labrum anterior to posterior lesions; (iii) glenohumeral osteoarthritis grade III or above (X-ray evaluation with the presence of osteophytes according to the Kellgren–Lawrence classification); (iv) adhesive capsulitis; or (v) previous surgery on the affected shoulder and re-tears of the RC.
Postoperative program
All patients were treated with a standard exercise program based on the consensus statement on shoulder rehabilitation developed by the American Society of Shoulder and Elbow Therapists. 14 Between 6 and 12 weeks after surgery, a supervised exercise program involving active or active-assistive ROM with limits of <120° of forward elevation and <30° of external rotation was performed. The exercises within this category used gravity-minimized positions, such as supine or side-lying and/or short lever arms, to promote RC and deltoid balance. Six exercises were performed, including the towel slide or horizontal dusting, active-assistive ROM supine washcloth press-up, active ROM supine press-up, side-lying supported active elevation, active ROM reclined wedge press-up, and supine elastic band forward elevation. 14 The prescription was 8 to 10 repetitions for each, maintaining the task for 5 to 10 s, with 1 min of rest between each repetition. Two sessions were performed per week over a 6-week period.
Additionally, two manual therapy techniques were applied. “Posterior glenohumeral mobilization” with the patient in the supine decubitus position with 20° abduction and slight external rotation of the shoulder, along with axial distraction in the inferior direction, and then a posterior glide maintained for 1 min, was performed. 15 Also, “scapular mobilization” with the patient in the side-lying position was performed, with the physiotherapist applying superior and inferior gliding, rotations, and distraction to the scapula of the affected shoulder. Each application was applied three times for 10 repetitions and at a rate of one cycle every 6 s, with a 30 s interval between sets. 16 Finally, with the patient in the supine position setting the elbow at 90° and shoulder at 0°, a self-assisted passive mobilization maneuver for external rotation (using a stick) was performed, and in the final sensation of restriction of movement, an isometric handgrip task was performed for 15 s (Supplemental Figure S2). 17 The postoperative program was delivered by two physiotherapists with a master’s degree in manual therapy and more than 15 years of experience in musculoskeletal physiotherapy.
Primary outcomes
Two blinded evaluators performed outcome assessments at baseline and at the end of the 6-week intervention. Both physiotherapists assessed the same proportion of patients. The primary outcomes were shoulder and upper limb function with the Constant–Murley and Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaires, respectively. The Constant–Murley questionnaire was used to assess shoulder function, scores range from 0 to 100, with lower scores indicating a worse condition. This questionnaire shows high reliability and sensitivity for the detection of post-intervention changes in a wide variety of shoulder pathologies and showed good inter- and intra-observer reliability (intraclass correlation coefficients, 0.71–0.93). 18 A previous study has shown that an increase of 11 points can be considered the minimal clinically important difference. 19
The Spanish version of the DASH questionnaire was used to assess the function of the upper limb. 20 Scores range from 0 to 100, with higher scores indicating a worse condition. This version of the DASH questionnaire has been shown to be a reliable, valid (Cronbach alpha = 0.96), and responsive instrument (test–retest reliability r = 0.96) that can provide a standardized measure in Spanish patients with upper extremity musculoskeletal disorders. 20
Secondary outcome measures
Pain intensity at rest and during movement was assessed using the visual analog scale (VAS), with scores ranging from 0 (“no pain”) to 10 (“the worst imaginable pain”). The VAS has been shown to be a reliable and valid instrument for the assessment of changes in pain intensity, and it is still commonly used in clinical and home settings. 21 Finally, a universal goniometer (Plastic BASELINE® Model 12–1000, White Plains, New York), with precision ±2°, was used to assess the passive ROM of the shoulder in external rotation, abduction, scaption (elevation in the scapular plane), and flexion. Each movement was measured three times, and the mean of these measurements was used for the analysis. The goniometer has good intra-rater reliability when consistent body landmarks are used (intraclass correlation coefficient ≥0.85). 22
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 26 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to describe the demographic and clinical characteristics of the patients. The parametric distribution of the continuous variables was checked using both the Kolmogorov–Smirnov test and graphical procedures (normal probability plot). Data were presented as means and standard deviations (SDs) for continuous variables and as numbers and percentages (%) for categorical variables. To assess the differences between pre-test and post-test, paired sample t-tests were conducted. Univariate testing for intragroup comparisons was conducted to analyze differences between pre- and post-test (Δ). Each analysis was covaried for the relevant baseline score, in addition to the specified participant age at assessment, sex, comorbidities, and level of irritability. Bonferroni adjustment was performed as a comparison test and a p-value of <0.05 was considered statistically significant
Results
The baseline characteristics for the participants are presented in Table 1. At the end of the early postoperative intervention program, there were no patient-informed complications associated with the treatment received, and there were no dropouts or withdrawals.
Baseline characteristics of patients with postoperative shoulder stiffness after arthroscopic RC repair.
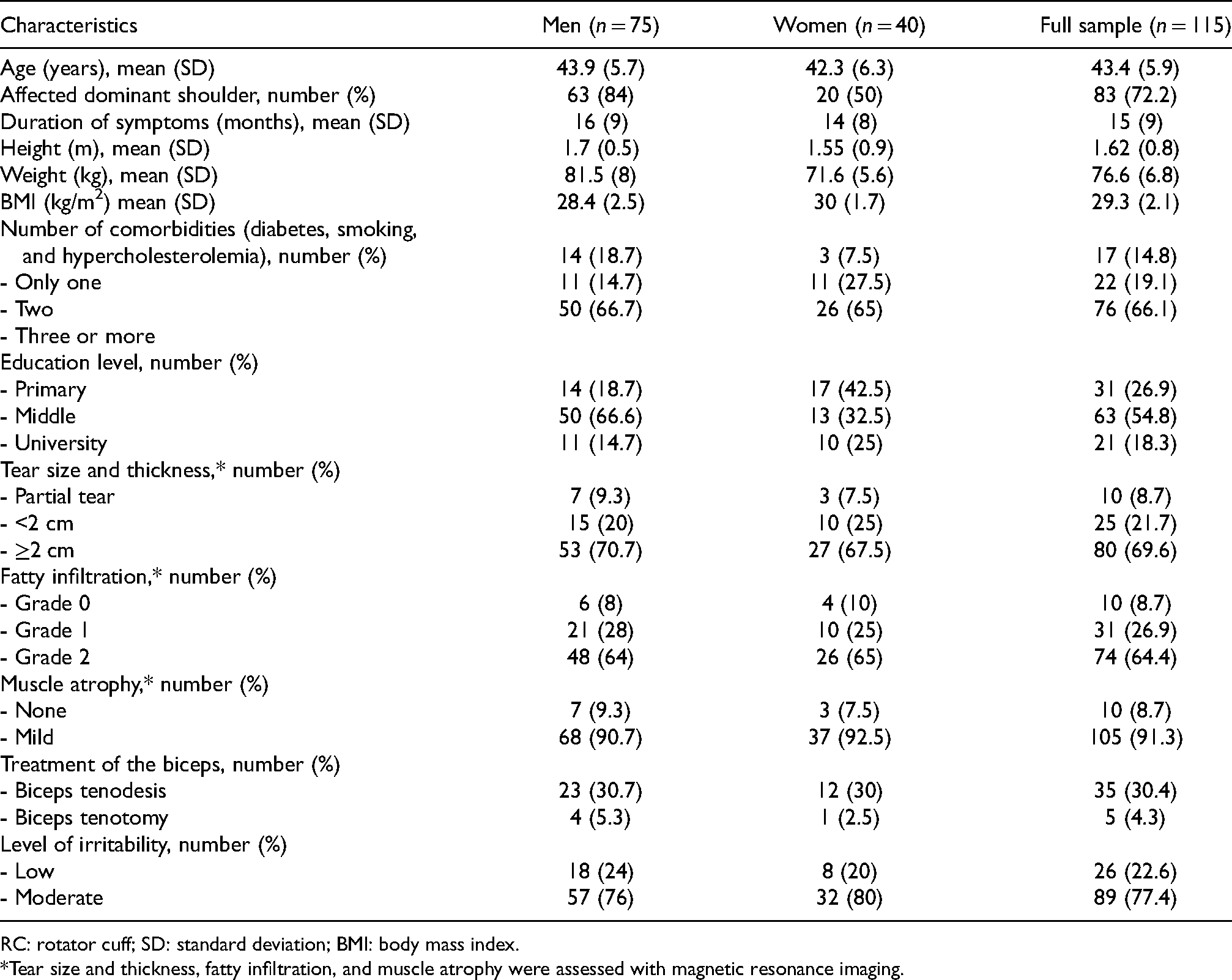
RC: rotator cuff; SD: standard deviation; BMI: body mass index.
*Tear size and thickness, fatty infiltration, and muscle atrophy were assessed with magnetic resonance imaging.
Figure 1 shows the values of the outcomes assessed before and after the postoperative program, as well as the effect of the treatment. After adjusting for confounding factors, such as age at assessment, sex, comorbidities, and level of irritability, the Constant–Murley questionnaire increased by 35.6 points (η2 = 0.29; p<0.001) (Figure 1(a)), DASH questionnaire decreased by 26.2 points (η2 = 0.06; p = 0.005) (Figure 1(b)), VAS at rest decreased by 2.8 cm (η2 = 0.62; p<0.001) (Figure 1(c)), VAS at movement decreased by 2.7 cm (η2 = 0.64; p<0.001) (Figure 1(d)), ROM external rotation increased by 45.9° (η2 = 0.26; p<0.001) (Figure 1(e)), ROM abduction increased by 75.6° (η2 = 0.05; p = 0.012) (Figure 1(f)), ROM scaption increased by 73.2° (η2 = 0.17; p<0.001) (Figure 1(g)), and ROM flexion increased by 67.6° (η2 = 0.00; p = 0.791) Figure 1(h)).
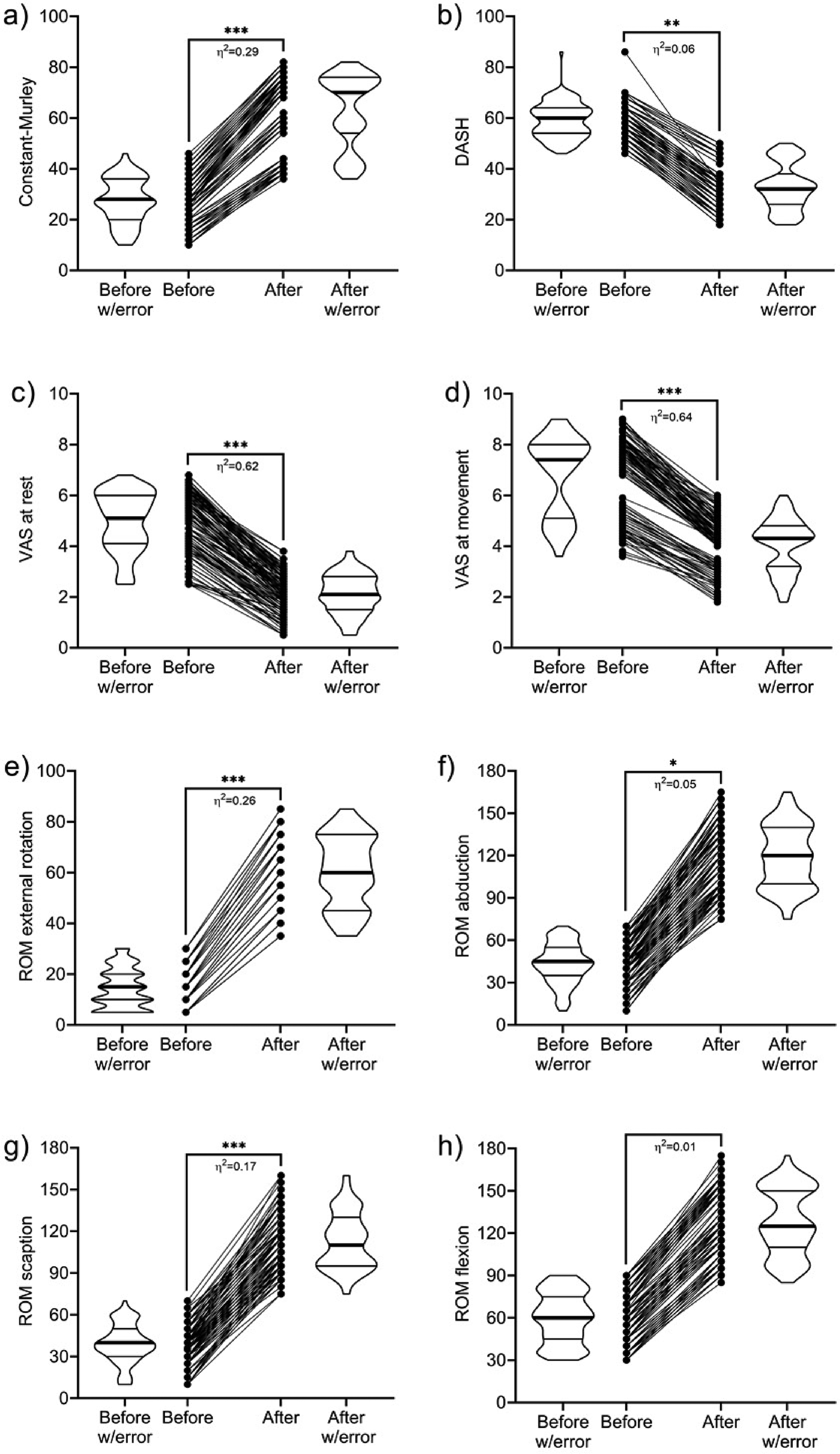
Comparison of the results between baseline and the sixth week of patients with postoperative shoulder stiffness after arthroscopic rotator cuff (RC) repair.
Discussion
The aim of this study was to assess the effects of a postoperative program on functional outcomes in patients with shoulder stiffness who had low to moderate irritability after arthroscopic RC repair. In the short term, patients receiving postoperative interventions showed clinically and statistically significant changes for most of the functional outcomes assessed.
RC tears are a common clinical problem with multifactorial etiology combining age-related degenerative changes and trauma. 2 Their surgical treatment has developed markedly in recent decades, with a significant change toward using arthroscopic procedures. 6 Despite the variability in the diagnostic criteria used, postoperative shoulder stiffness is the main complication of arthroscopic RC repair. 7 Several studies have investigated the effects of physical therapy programs in patients with shoulder stiffness; however, there are no published studies that have considered the level of irritability in the treatment of patients after arthroscopic RC repair. A staged approach to shoulder disorders was proposed, where the categorization of the level of irritability enables the selection of a matched intervention intensity. 11 However, specific details regarding the optimal timing, type, and doses of therapeutic interventions to treat shoulder disorders most effectively have not yet been defined.
From the available evidence, two studies showed significant clinical improvement in functional outcomes after a physical therapy program based on the level of irritability in patients with other shoulder disorders.15,23 Our results support these findings; this could be explained by the combination of some therapeutic interventions in our postoperative program. Although the American Society of Shoulder and Elbow Therapists consensus does not provide treatment guidelines for patients with stiffness after surgery, we included posterior glenohumeral mobilization, scapular mobilization, and self-assisted passive mobilization with isometric handgrip task for external rotation.
Based on the best available evidence, the international consensus statement proposes a specific exercise program that is safe and effective for patients after arthroscopic RC repair. The exercise program used was centered on the principle of the gradual application of controlled stresses to the healing RC. 14 Initially, active and active-assistive ROM exercises with an electromyography activity level <15% were performed. Once the patients tolerate the introduction of active loading, elevation can be progressed to exercises that show electromyography activity levels between 16% and 29%. 14 The general principles of the exercise program were as follows: (1) exercises were performed with optimal scapular positioning and control without abnormal compensatory trunk movement and (2) started with low load/low activation exercises, without pain, emphasizing the quality of the performance of the motor task (performed slowly, consciously, and progressively). We hypothesize that the exercise may induce hypoalgesia by activating a descending pain modulation pathway related to the modulation of nociceptive afferents (i.e. the signal transmission via Aδ and C fibers) and central inhibitory pathway networks (GABAergic mechanisms) of the central nervous system.24,25
Regarding the effects of manual therapy techniques, glenohumeral posterior mobilization is a high-grade technique applied in the final ROM, with the aim to restore arthrokinematics movement through distention and elongation of the periarticular structures. 15 This concept is based on the physical components of the length-tension curve, which studies the behavior of tissues when they are subjected to a load, demonstrating that its properties vary (progressing from an elastic phase to a plastic phase). 15 Several clinical studies have shown an increase in glenohumeral ROM and shoulder function,15,16,26 and its clinical effectiveness increase when scapular mobilization is added. 16
Regarding the isometric handgrip task, some studies have shown a significant increase in the electromyographic activity of the RC muscles.17,27 Some theories mention that the isometric handgrip task could generate an indirect decrease in tissue restriction and for the activation of RC muscles and co-activation between the proximal and distal muscles of the arm upper limb kinetic chain, independent of the shoulder movement. 17 This mechanism could be explained by the changes in the activity of the shoulder muscles and potential changes in the “internal loading” of the shoulder. 28 Probably, this mechanism is mediated by a neural network located in the spinal cord and cortical and subcortical areas of the central nervous system that would increase the motor variability of the agonist and synergistic muscles to execute and sustain a specific task.29,30 Thus, the handgrip can be used to increase the excitability of neural impulses to all muscles in the upper limb, leading to greater shoulder joint stability temporarily and attenuating joint stiffness. 30 In addition to the effects of exercise and manual therapy techniques, it relieves pain, reduces shoulder stiffness, and mainly optimizes the improvement of the glenohumeral ROM of external rotation.26,30
While the results of this study are encouraging, any inference from this study needs to be tempered due to some limitations. First, since we did not include a comparison control group, elements such as the natural history of the condition were likely to have compromised our findings. Second, the lack of control for confounding factors inherent in observational studies, including co-interventions such as consumption of medications among participants during the treatment period, may have produced some overestimation of the treatment effects. Finally, our study aimed to evaluate the immediate effects (without follow-up) of the intervention. Therefore, there is a need to determine if these reported benefits could be sustained in the long term. Future research is needed to overcome these limitations and expand the analysis of the existing evidence regarding the effects of a postoperative program in the management of patients with shoulder stiffness who have low to moderate irritability after arthroscopic RC repair.
Despite its limitations, the results of this study provide an important clinical contribution to the physical therapy area and the management of shoulder stiffness after arthroscopic RC repair. Physical therapy is considered a first-line treatment for shoulder disorders, and this study confirms this notion. In this study, the combination of active common interventions applied by a physiotherapist, such as an exercise and manual therapy, displayed significant and clinically meaningful therapeutic benefits. The results of this study need more in-depth consideration of this postoperative program in the management of this clinical condition.
Conclusions
In the short term, the postoperative program showed clinically and statistically significant benefits in most of the functional outcomes assessed. Additionally, further studies controlling confounders and longer follow-ups are needed to confirm these results.
Supplemental Material
sj-docx-1-otr-10.1177_22104917221116387 - Supplemental material for Effects of a postoperative program in patients with shoulder stiffness following arthroscopic rotator cuff repair
Supplemental material, sj-docx-1-otr-10.1177_22104917221116387 for Effects of a postoperative program in patients with shoulder stiffness following arthroscopic rotator cuff repair by Héctor Gutiérrez-Espinoza, Felipe Araya-Quintanilla, Sebastián Pinto-Concha, Walter Sepúlveda-Loyola, Robinson Ramírez-Vélez and Jorge Fuentes-Contreras in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-docx-2-otr-10.1177_22104917221116387 - Supplemental material for Effects of a postoperative program in patients with shoulder stiffness following arthroscopic rotator cuff repair
Supplemental material, sj-docx-2-otr-10.1177_22104917221116387 for Effects of a postoperative program in patients with shoulder stiffness following arthroscopic rotator cuff repair by Héctor Gutiérrez-Espinoza, Felipe Araya-Quintanilla, Sebastián Pinto-Concha, Walter Sepúlveda-Loyola, Robinson Ramírez-Vélez and Jorge Fuentes-Contreras in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-docx-3-otr-10.1177_22104917221116387 - Supplemental material for Effects of a postoperative program in patients with shoulder stiffness following arthroscopic rotator cuff repair
Supplemental material, sj-docx-3-otr-10.1177_22104917221116387 for Effects of a postoperative program in patients with shoulder stiffness following arthroscopic rotator cuff repair by Héctor Gutiérrez-Espinoza, Felipe Araya-Quintanilla, Sebastián Pinto-Concha, Walter Sepúlveda-Loyola, Robinson Ramírez-Vélez and Jorge Fuentes-Contreras in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Declaration of conflict of interests
The authors declare they do not have any potential conflict of interest regarding the investigation, authorship, and/or publication of this article.
Ethical approval
The Ethics Committee of the Central Metropolitan Health Service in Santiago of Chile approved the study protocol on 8 January 2016.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.