
Abstract
Keywords
Introduction
A giant cell tumor (GCT) of the bone is a benign, locally aggressive tumor. It usually occurs at the meta-epiphysis of the long bone, especially the distal femur, proximal tibia, proximal humerus, and distal radius. The distal ulna is an extremely rare site and the incidence varies from 0.45% to 3.2%. 1 Because of its highly aggressive nature and high chances of recurrence, en bloc resection (wide local excision) is recommended. 2 Various complications have been reported following excision of the distal ulna, including loss of ulnar support, carpal collapse, radioulnar impingement, dorsal displacement of the ulnar stump, and loss of grip strength and wrist instability.3–5 Therefore, after en bloc excision, it is important to restore the function of the distal radioulnar joint (DRUJ) and stabilize the ulnar stump as well. Various options are available after resection of distal ulna GCT such as extensor carpi ulnaris (ECU) tenodesis of the residual ulnar stump, reconstruction of the ulnar head with second metatarsal head or allograft, ulnar head arthroplasty, or the Sauve–Kapandji procedure, which are helpful to preserve wrist function.6–10 To the best of our knowledge, very few case reports have been found, in which the GCT was resected en bloc followed by iliac crest graft fixation to the distal end radius to maintain the ulnar support, and ECU tenodesis for achieving the ulnar stability. We present our series of seven cases of Campanacci grade III GCT distal ulna, managed with en bloc resection along with fixation of tricortical iliac crest graft to the distal end radius with screws for maintaining the ulnar wrist support followed by stabilization of the proximal ulnar stump using ECU tenodesis.
Methods
The study was approved by the Institutional Ethics Committee and informed consent was provided by all participants. Seven patients of Campanacci grade III GCT distal end of the ulna were treated and followed up from 2015 to 2021 at our institution. Patients were categorized using a Campanacci radiological grading method. 11 Histopathologically confirmed (core needle biopsy) cases of GCT of the distal ulna, who were reported to tumor clinic in our hospital and were diagnosed clinically and radiologically as Campanacci Grade III GCT of the distal ulna, were included in the study. Patients with Campanacci Grade I or II GCT of distal ulna and patients with recurrent GCT of distal ulna after successful surgical treatment were excluded. There were three male and four female patients. The average age at presentation was 27 years (range 25–30 years). The average follow-up period was 42 months (range of 30–48 months). Patients were presented with complaints of swelling over the wrist with pain over the involved wrist with radiation up into the arm. Swelling was gradually progressive and tender on palpation. The surrounding tissues such as tendons, vessels, nerves, and skin over the swelling were not involved. Range of motion (ROM) was decreased in all the directions. Provisional diagnosis was done clinico-radiologically with standard x-rays of the wrist (expansile lytic lesion at distal end ulna; Figure 1(a) and (b)). To rule out the metastasis, chest x-rays were also performed. Magnetic resonance imaging (MRI) of the wrist with distal forearm was performed to localize the extent of the tumor and involvement of the soft tissues. Lesions were hypointense in T1W and heterogeneous in T2W image on MRI (Figure 2(a) and (b)). We included only Campanacci Grade III tumors in our study. The diagnosis was confirmed by core needle biopsy in all cases. There was no evidence of metastatic disease in any of the patients at the time of diagnosis. All patients were managed with extra-periosteal resection (wide local excision/en bloc resection) followed by fixation of tricortical iliac crest graft to the distal end radius with two 3 mm cancellous screws for maintaining the ulnar wrist support and stabilizing the proximal ulnar stump using ECU tenodesis. Resected specimen was sent for histopathology in all cases.

Anteroposterior view (a) and lateral view (b) plain radiographs showing expansile lytic lesion at the distal ulna (soapy bubble appearance).

Magnetic resonance imaging (MRI) of the lesion at the distal ulna (a)–(d).
Surgical procedure
All patients were worked up and were taken up for surgery in a supine position under the combined supraclavicular block and general anesthesia. A medial longitudinal incision over the distal ulna was used. The plane was made between ECU and flexor carpi ulnaris. After careful dissection of all the tissues around the tumor and distal ulna (Figure 3), and without injuring the capsule over the tumor with 2 cm of clear margins, the resection of the distal part was performed with preservation of the triangular fibrocartilage fovea insertion together with ulnar head attachment of the volar/dorsal radioulnar ligament and ulnar collateral ligaments. The dorsal sensory branch of the ulnar nerve was isolated and preserved.
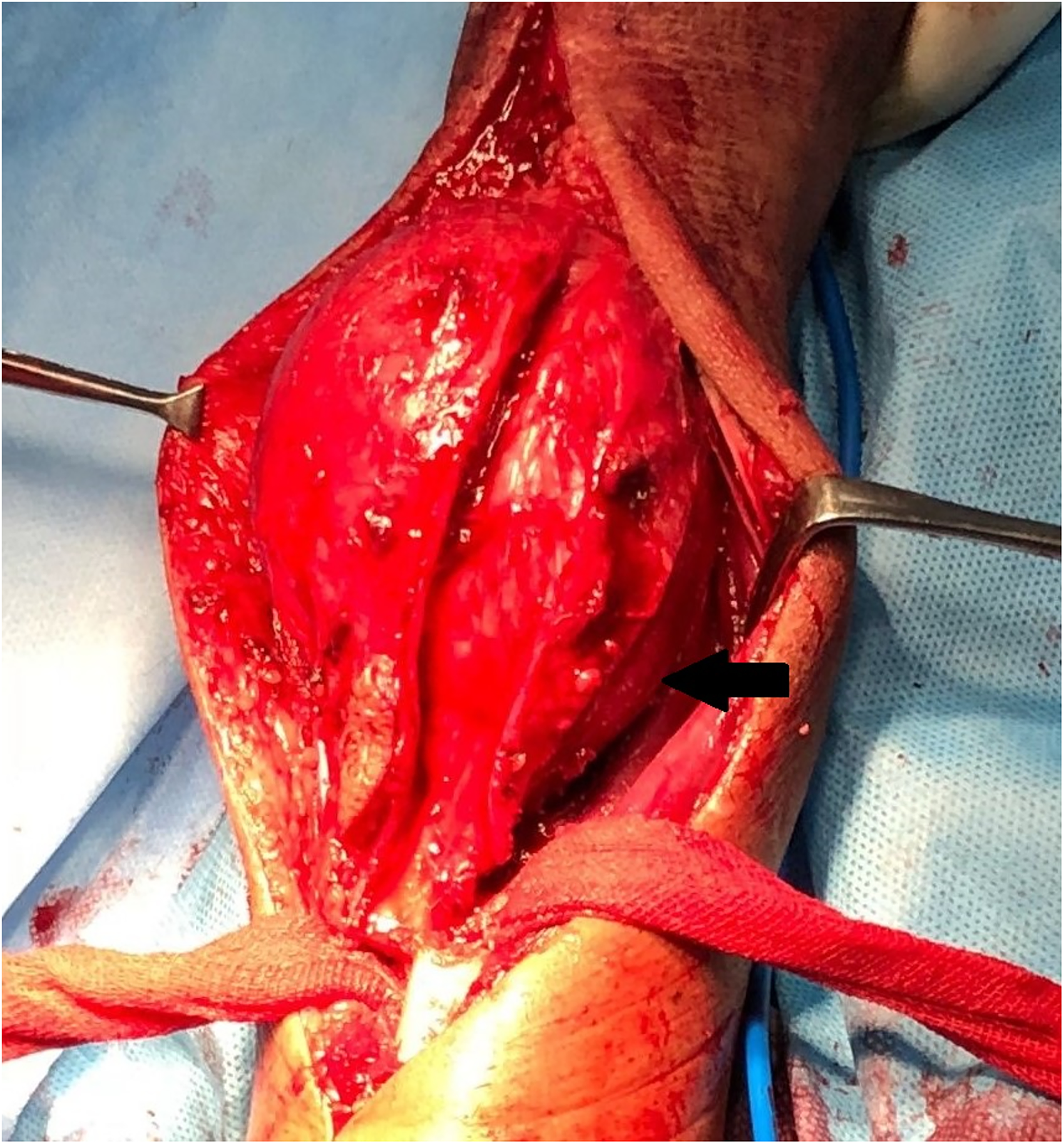
Intraoperative picture of the tumor mass originating from distal ulna.
We harvested the iliac crest bone graft of size 2 cm in length, width, and height. The sigmoid notch was prepared with the removal of the cartilage and was flattened out to fit the bone graft. The graft was set to be at a mild ulnar-minus variance of 1 mm. We fixed this graft with two cancellous screws (3 mm). The triangular fibrocartilage complex (TFCC), volar/dorsal radioulnar ligaments, and ulnar collateral ligament were sutured to the ulnar margin of the bone graft. The ECU tendon was dissected free from the tumor mass and split longitudinally into a slip just proximal to the ulnar stump. The slip of the ECU tendon was then passed through a drill hole, 5 mm above the end of the ulnar stump in a dorsal to volar direction with the forearm held in supination. The tendon was then directed to the ulnar side and sutured back on itself, thus stabilizing the residual ulnar stump. The wound was closed in a routine fashion over a drain. Resected specimens were sent for histopathology. Postoperatively, the forearm and wrist were immobilized in supination with the above elbow slab for a period of 2 weeks following which gentle wrist and forearm exercises were started. All cases were followed up for an average period of 3.5 years. Functional outcomes till the final follow-up were documented using the Visual Analog Score (VAS), modified Musculoskeletal Tumour Society (MSTS) score, Disability of Arm, Shoulder, and Hand (DASH) score, and Modified Mayo Wrist Score (MMWS) at regular interval of 1 year. Patients were monitored for any signs of recurrence both clinically and radiologically. Follow-up X-ray images were compared with the initial baseline postoperative X-ray images for the appearance of any new lucency at the remaining ulnar stump/graft or soft tissue shadow in the distal forearm. Cross-sectional imaging with computed tomography or MRI could be done which allows better evaluation of osteolysis and the presence of a soft-tissue mass. Figure 4(a) and (b) shows the postoperative x-ray after 1 year of follow-up.

Postoperative radiograph (anteroposterior view (a) and lateral view (b)) after 1 year of follow-up clearly shows a union of graft with distal end radius.
Statistical analysis
All quantitative data were expressed as mean ± standard deviation. Analysis between preoperative and postoperative scores was done by paired t-test with a p-value < 0.05 considered as significant.
Results
All seven patients selected for the study had Campanacci grade III GCT distal ulna. There were three men and four women with a male to female ratio of 3:4 (Table 1). The average age at presentation was 27 years (range 24–30 years). Average length of resected tumor was 6.7 cm (Table 1). The histopathological examination of resected specimen reported GCT in every case (Table 1). The mean duration of follow-up was 42 months (range 32–48 months). All patients had limitation of ROM on operated as compared to the normal side at the time of final follow-up. The mean ROM of wrist was 42.1° ± 5.9° of flexion, 72.9° ± 6.4° of extension, 82.1° ± 8.1° of supination, and 85.0° ± 5.8° of pronation at the final follow-up. The mean VAS score at the final follow-up was 0.9 ± 0.9 (Table 2). The mean Mayo Wrist score was 71.4 ± 6.4 with a mean MSTS score of 25.9 ± 0.8 at the final follow-up (Table 2). The mean DASH score at the final follow-up was 17.9 ± 1.6 (Table 2). The average time for the fusion of tricortical iliac crest graft (radiological union) with the distal end radius was 13.3 weeks (Table 1). Common complications such as surgical site infections, bone resorption, or non-union of graft were not noted in any of the cases. None of the cases showed recurrence (Table 1).
Demographic details, tumor findings, follow-up period, union time of graft, and recurrence.
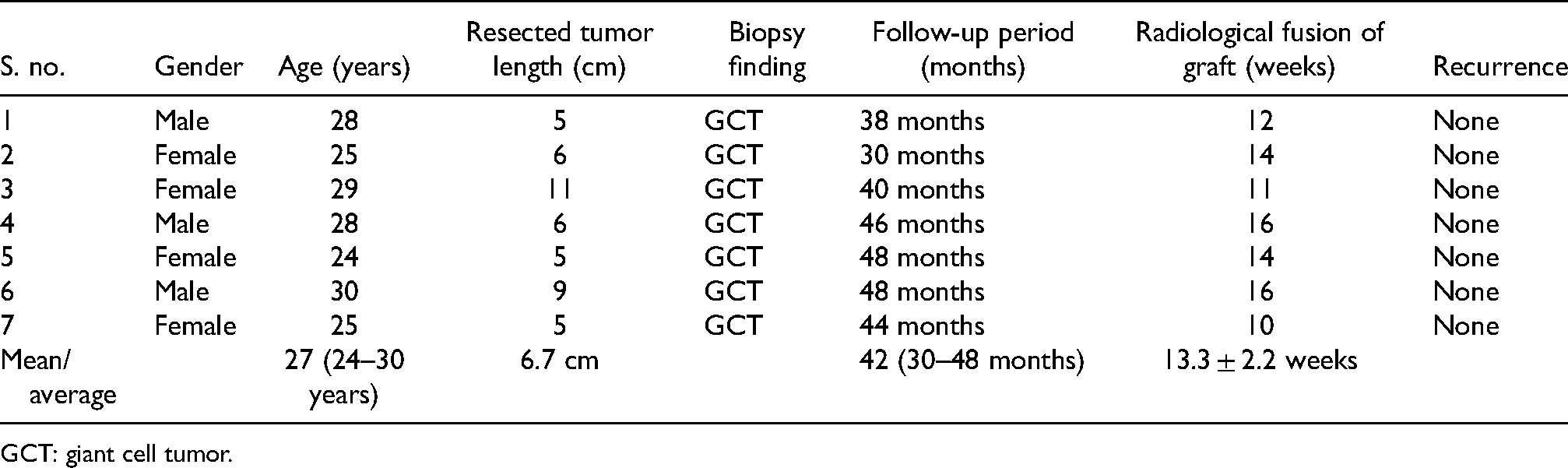
GCT: giant cell tumor.
Functional scores of patients at different follow-ups.
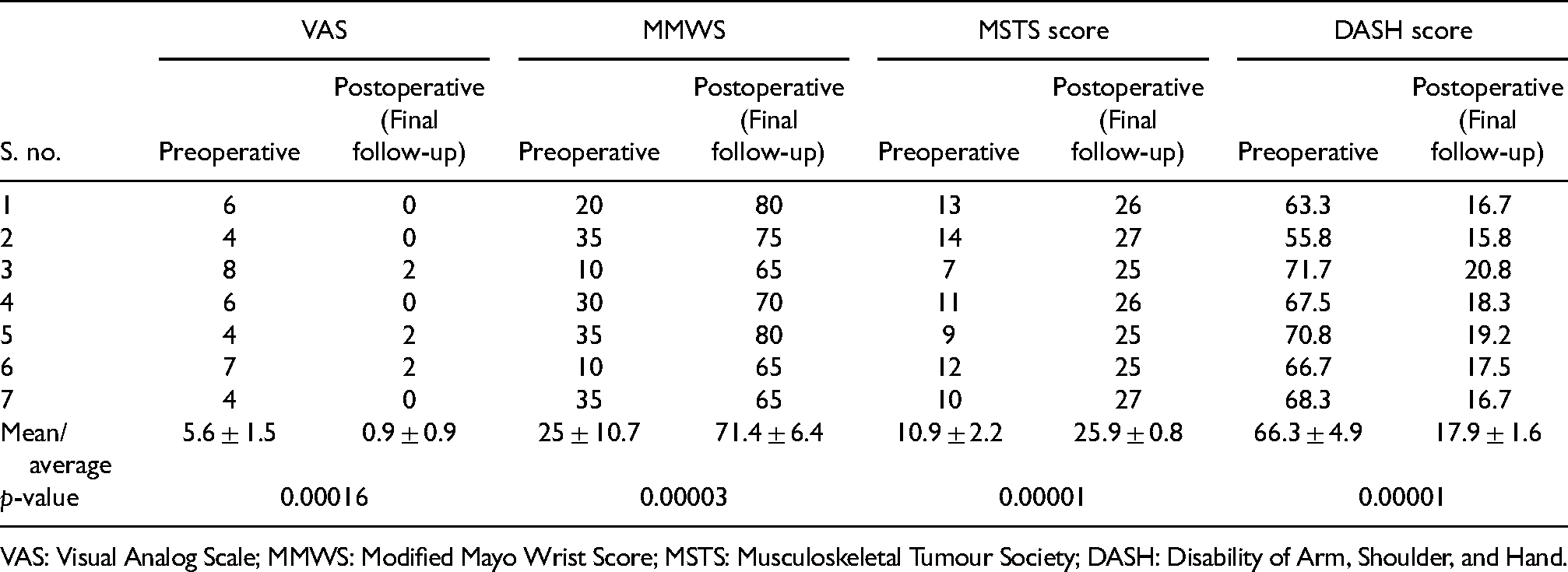
VAS: Visual Analog Scale; MMWS: Modified Mayo Wrist Score; MSTS: Musculoskeletal Tumour Society; DASH: Disability of Arm, Shoulder, and Hand.
Discussion
GCT is essentially a benign tumor that is locally aggressive in nature and has the potential to metastasize to the lungs. 12 GCT at distal ulna although rarer yet more aggressive than GCT of the distal radius.2,13 Therefore, en bloc excision is recommended especially for Campanacci grade III GCT ulna. 14
Traditionally, distal ulna has been considered a dispensable bone, and its resection for degenerative conditions was first described by Darrach and subsequently modified by Dingman. 15 Most of the studies on GCT ulna have focused on wide resection of the distal ulna. Cooney et al. 16 achieved excellent results in 75% of the cases with tumors of GCT ulna after en bloc resection alone and concluded that reconstruction of the osseous defect is not routinely indicated. Similar results have been shown by Wolfe et al. 17
The wide resection in cases of tumors of distal ulna may not be functionally equivalent to that of the excision in Darrach's procedure meant for degenerative conditions, the reason being the significant soft tissue and bone losses encountered during tumor resection leading to instability of residual ulnar stump. The distal end of the ulna plays an important role in forearm rotations (supination and pronation), grip strength, and maintaining the stability of the wrist, because of its relationship with the distal radius, carpus, TFCC, and the ulnar collateral ligament.18,19 Many complications have been described in the literature due to the unstable ulnar stump left after the distal ulnar resection. Common complications include digital extensor tendon ruptures, snapping during forearm rotation, pain, and limitation of activity due to decreased dynamic interosseous space produced by the combined actions of pronator teres and pronator quadratus with ulnar stump impingement on the radius metaphysis.1,4,14,20–23 Newmeyer and Green 21 recommended stabilization of the distal ulna to prevent digital extensor tendon ruptures after distal ulna resection. Similarly, Goldner and Hayes 14 concluded their study that stabilization using one-half of the ECU tendon can prevent the pain arising from the movement of the ulnar stump and hypermobility of the ECU tendon. Kayias et al. 6 also reported an excellent result after resection of the distal ulna for GCT followed by stabilization with ECU. Other procedures such as Lasso tendon graft, 24 ECU, Fascia Lata autograft, or plate arthrodesis have been used for the stabilization of distal ulna in earlier studies. 4 To avoid the complications related to wrist instability and DRUJ after resection of GCT distal ulna, many procedures have been described in the literature. Harness and Mankin 2 recommended iliac bone graft as ulnar buttress which was also performed by Hashizume et al., 25 Naik et al., 26 and Tsai et al. 27 Wurapa and Whipple 28 reconstructed the DRUJ with two-stage allograft. Some authors have combined the ECU tenodesis with iliac crest graft to the distal radius.25,26,29 All of these were case reports of single case only.
We combined the procedure for maintaining the wrist stability and ulnar stump stabilization in our study after en bloc resection in seven cases of Campanacci grade III GCT of the distal ulna and the functional outcome was noted over a follow-up period of 32 to 48 months (average 42 months). The ulnar support was maintained by fixing the tricortical iliac crest graft to the distal radius and the ulnar stabilization was achieved by ECU tenodesis. We used these methods because both are simple to use, requires minimum skill and are cost-effective as compared to others reported in the literature. Patients presented were young adults (24–30 years). The average length of resected specimen was 6.7 cm. Mean VAS score was improved from 5.6 ± 1.5 preoperatively to 0.9 ± 0.9 at final follow-up. The mean MSTS score was also improved from 10.9 ± 2.2 preoperatively to 25.9 ± 0.8 at final follow-up. The mean MMWS was improved from a preoperative value of 25 ± 10.7 to 71.4 ± 6.4 at the final follow-up. The mean DASH score was also improved from 66.3 ± 4.9 (preoperatively) to 17.9 ± 1.6 at most recent follow-up. The ROM of the operated wrist was improved in all cases as compared to a preoperative value. Maximum ROM was achieved in supination (82.1° ± 8.1°) and pronation (85° ± 5.8°) movements. The ROM achieved in flexion was lesser than other movements (42.1° ± 5.9°). All patients had a limitation of ROM on operated as compared to the normal side at the time of final follow-up. All patients made great improvements in ROM and grip strength, and till their last follow-up postoperatively, all had near complete pronation and supination along with excellent wrist and elbow functions. None of the patients had shown any complication or recurrence.
Reconstruction of the distal ulna with metallic prosthesis after complete excision of the tumor is a viable option that helps preserve the function of the wrist including grip strength.5,30 But due to the constraints associated with this method of reconstruction such as high implant costs, non-availability of implant locally, lack of sufficient long-term studies, and anticipated complications associated with any other metallic prosthesis such as loosening, infections, periprosthetic fractures, and so on, our procedure stood better and circumvents all such problems.
To our knowledge, only a few case reports of resection of the ulna GCT with a reconstruction of DRUJ and stabilization of residual ulnar stump with ECU tenodesis, are reported in the literature. Our study of seven cases of GCT distal ulna managed with this method achieved near-normal supination and pronation movements and excellent functional outcomes at final follow-up with no recurrence. The limitation of our study was the small population size, while relative cost-effectiveness, easy to learn and reproducible procedure with good to excellent functional outcomes, and mid-term follow-up were the strengths of our study.
Conclusion
In cases of Campanacci grade III GCT of the distal ulna, wide resection (en bloc resection) is the treatment of choice and after the resection of the distal ulna, reconstruction of DRUJ and stabilization of residual ulnar stump are important adjuncts to achieve good functional outcomes. Hence, we recommend reconstruction of DRUJ using fixation of tricortical iliac crest graft and stabilization of ulnar stump by ECU tenodesis, as a combined procedure after the wide resection of the GCT distal ulna for good to excellent functional outcomes with a good ROM.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.