
Abstract
Purpose
The anterior cruciate ligament in the knee is commonly prone to injuries. Reconstruction of this ligament with hamstring tendon has been time-tested but peroneus longus autograft is also gaining popularity. However, very limited literature is available comparing the two grafts. This study aims to compare the functional outcome and donor site morbidity between hamstrings and peroneus longus autograft in anterior cruciate ligament reconstruction.
Methods
A prospective randomised study was conducted on 45 patients, who underwent anterior cruciate ligament reconstruction. Patients were assigned into Hamstring group and the Peroneus longus group. Functional outcome was assessed using Lysholm score and Modified Cincinnati scores for the knee joint and American Orthopedics Foot and Ankle Scoring for ankle joint. Donor site morbidity was assessed by measuring flexion and extension strength of the knee and plantar flexion and eversion strength of the ankle by handheld dynamometer preoperatively and postoperatively at 6 months and 1 year follow up.
Results
Functional outcome of the knee showed significant improvement in peroneus longus group (p-value 0.002) compared to hamstring group. Even though there was minimal reduction in functional outcome of the ankle at 6 months follow-up in peroneus longus group, it improved at one year follow-up. While assessing the donor site morbidity at the knee joint, knee flexion strength showed improvement in the group (p-value 0.02) but reduced in the hamstring group where the hamstring tendon was harvested. Knee extension strength in the hamstring group scored marginally better than the peroneus longus group, which was not statistically significant (p-value 0.5).
Conclusion
Autologous peroneus longus tendon can be used as a graft of choice in anterior cruciate ligament reconstruction which showed promising results without compromising on the ankle function. Its usage as an alternative source of the graft may be more useful in multi-ligament injuries of the knee joint.
Introduction
The anterior cruciate ligament (ACL) is an important ligamentous structure in the knee joint which helps in maintaining stability. ACL tears contribute to approximately 50% of knee injuries. 1 ACL reconstruction has been the standard surgical procedure in the case of ACL insufficiency. Over decades ACL reconstruction has evolved in terms of technique and graft used.
The patients in whom the Hamstring tendon (HST) is used as an autograft for ACL reconstruction have early recovery of quadriceps strength, good graft uptake, better tensile strength and less joint stiffness with satisfactory results in terms of patient compliance. 2 But it has limitations like random graft size, a probable decrease in knee joint flexion power, infection risk due to inadequate closure of the sartorius fascia and injury to the saphenous nerve during harvesting. 3
Peroneus longus tendon (PL) is being used as an alternative to HST graft in recent years.4,5 Tensile strength of four-strand hamstrings and double-strand peroneus longus was found to be higher than naive ACL which provides provision for the thought of harvesting peroneus longus for ACL reconstruction. 6 Adequate diameter and length of PL have their upper hand over hamstrings autograft. It was found that even the anterior half of the PL tendon has enough length and strength to be effective in ACL reconstruction. 7 Harvesting the entire PL has no effect on the stability of the ankle or gait proven by a biomechanical and kinematic study. 8
In assessing the donor site morbidity, muscle strength has been believed to be a potential factor for physical performance, activities of daily living and sports activities. Hence following ACL reconstruction with HST or PL graft, the motor power of knee and ankle joint performance needs to be assessed.
The purpose of this study is to compare the functional outcome of knee and ankle by using MCS, Lysholm score and AOFAS respectively and donor site morbidity by measuring flexion and extension strength at the knee and eversion and plantar flexion strength at the ankle by HHD after ACL reconstruction using hamstrings and peroneus longus autograft. The outcomes were evaluated in each group preoperatively and at 6 months and 1 year postoperatively and analysed.
Outcomes
Methods
Patients were assigned into 2 groups by computer-generated simple randomisation to HST(N = 22) or the PL(N = 23). (Figure 1)
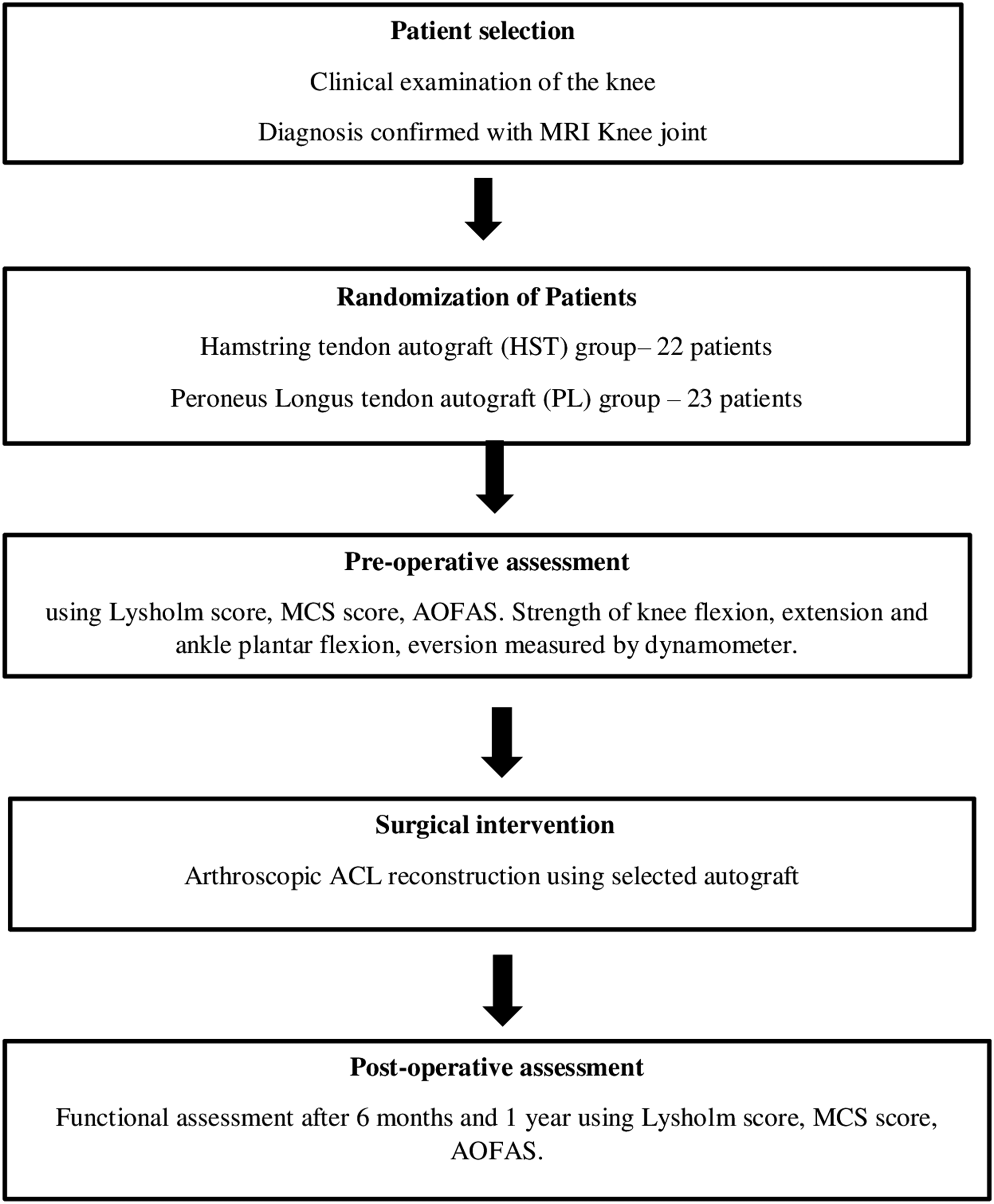
Flow chart of the methodology of the study.
Option of “Random numbers” is selected and proceeded forward by selecting the “Randomly assign subjects to groups”. Enter the number of subjects in each group in tab “Assign” and select the number of the group from tab “Subjects to each group” and keep number 1 in repeat. Randomisation ratio was 1:1 for the study comparing the two groups.
Prior power analysis was done to ensure the sample was adequate for the study.
The study was approved by the institutional ethical committee. The informed consent was taken from the patient before the study.
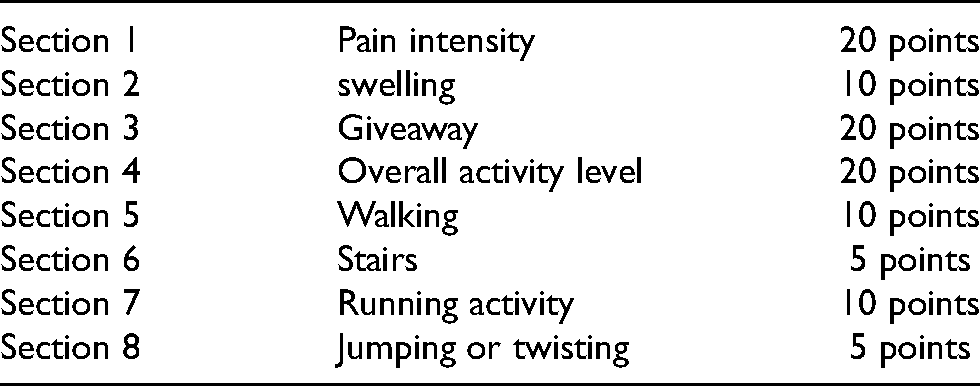
The methodology of the study has been depicted in the form of a flow chart (Figure 1). Functional outcome was analysed using Lysholm score, Modified Cincinnati score (MCS) for the knee joint and American Orthopedic Foot and ankle society score for ankle joint. The Modified Cincinnati Knee score consists of 8 domains. Each domain consists of 5–6 questions which are to be answered by the patient at every follow-up (Table 1).
This table shows sections of modified cincinnati score.
The muscle strength around the knee joint and ankle joints was measured before surgery on both normal and ACL deficient knees. (Figure 2) The unit of measurement of muscle strength was calculated in pounds (lb) in the handheld dynamometer. The normal side is taken as control. This value is compared to the muscle strength of the operated side after 6 months and 1 year postoperatively by MAKE method using an HHD where the machine is held statically and the patient tries to press it with full force and the average of three readings were recorded. 9
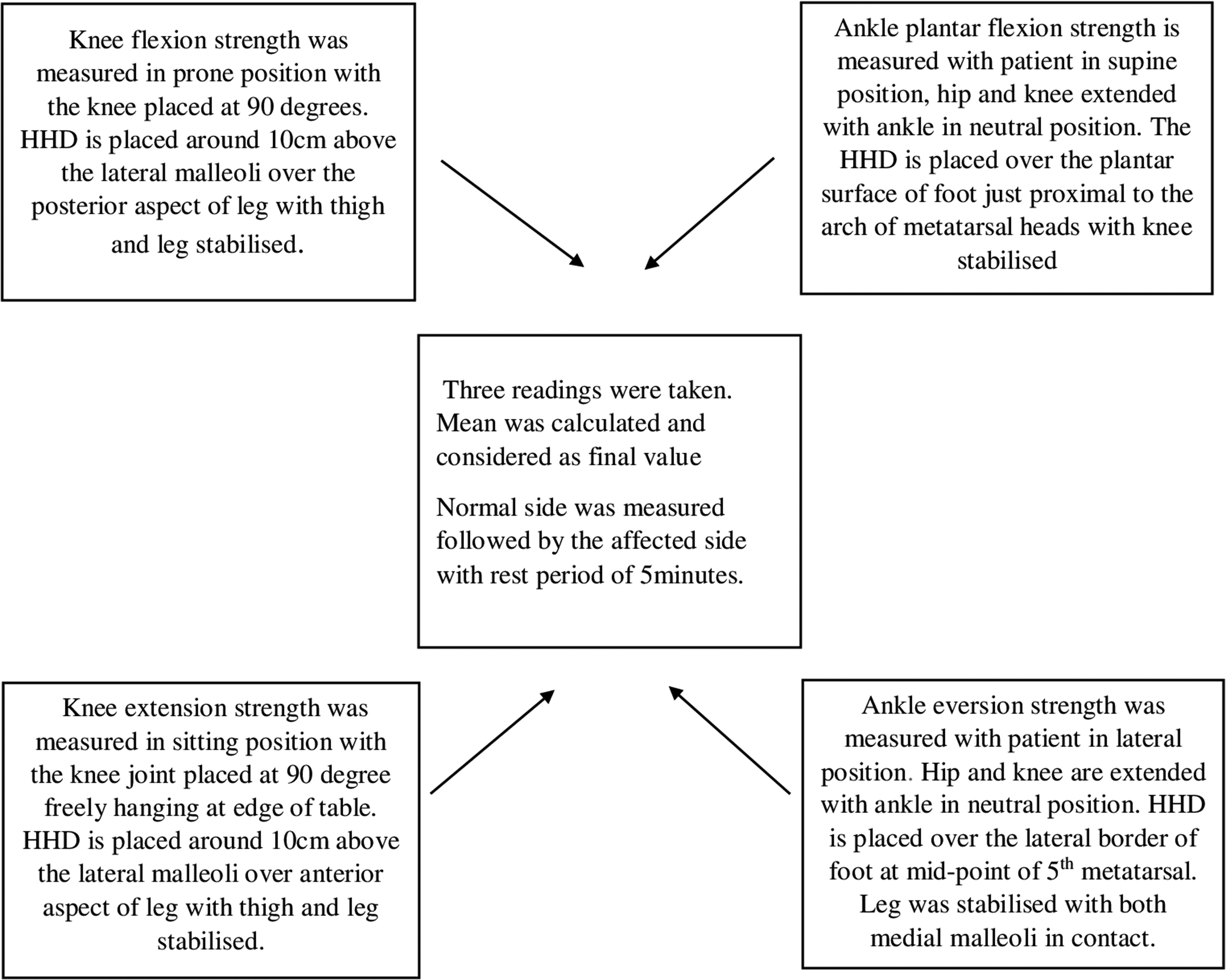
Technique of muscle strength measurement by HHD.
All measurements were taken by a single person to avoid study bias. Placement of HHD and measurement of muscle strength of the knee 10 and ankle 11 and the position of the patient is shown in Figures 2 and 3. The HHD was positioned over the limb in such a way that person measuring has the maximum mechanical advantage.

Testing the muscle power.
Arthroscopic procedure
Standard anterolateral and anteromedial portals were used. Diagnostic arthroscopy was done before harvesting the graft. ACL reconstruction was performed by using the selected autologous graft either HST or PL graft harvested from the ipsilateral limb and fixed by loop endobutton on femur tunnel side and bio-absorbable screw-on tibial tunnel side in both hamstrings and peroneus longus groups.
The technique of ACL reconstruction with peroneus longus tendon autograft
ACL reconstruction using ipsilateral PL autograft was performed by a single senior knee surgeon. The full-thickness PL graft was harvested using an incision of about 2 cm long posterior to the lateral malleolus just above the superior peroneal retinaculum. PL and peroneus brevis tendon (PB) are exposed taking care not to injure the sural nerve. PL and PB are levered out of the skin window. Tenodesis of PL to PB is done. Heavy nonabsorbable Krackow stitches are placed on the PL and later incised. PL is then separated from the surrounding soft tissues. The tendon is harvested proximally using an open long tendon stripper about 4–5 cms from the fibular head to prevent peroneal nerve injury using a long tendon stripper by controlled tension. The point where tendon stripper was halted while harvesting the graft was loss of resistance while simultaneously pulling force on distal end of stump and advancing the tendon stripper forward. The point of loss of resistance was marked on skin and was observed that it was around 4–5 cm on average from the fibula head in the patients. The wound is closed in layers (Figure 4). Graft preparation was done by separating the muscle fibres from the tendon. Krackow-type whipstitches are placed on both ends of each tendon with nonabsorbable sutures. The graft may be doubled, tripled or quadrupled depending on the length of graft obtained to 7 mm to 8mm in thickness. After the preparation of the femoral and tibial tunnels, the tendon is passed and fixed as described earlier. The average length of the peroneus longus harvested was 8.5–9.0 cm and diameter on average was 8.5 cm. Peroneus longus autograft was longer in length and diameter compared to hamstrings autograft.
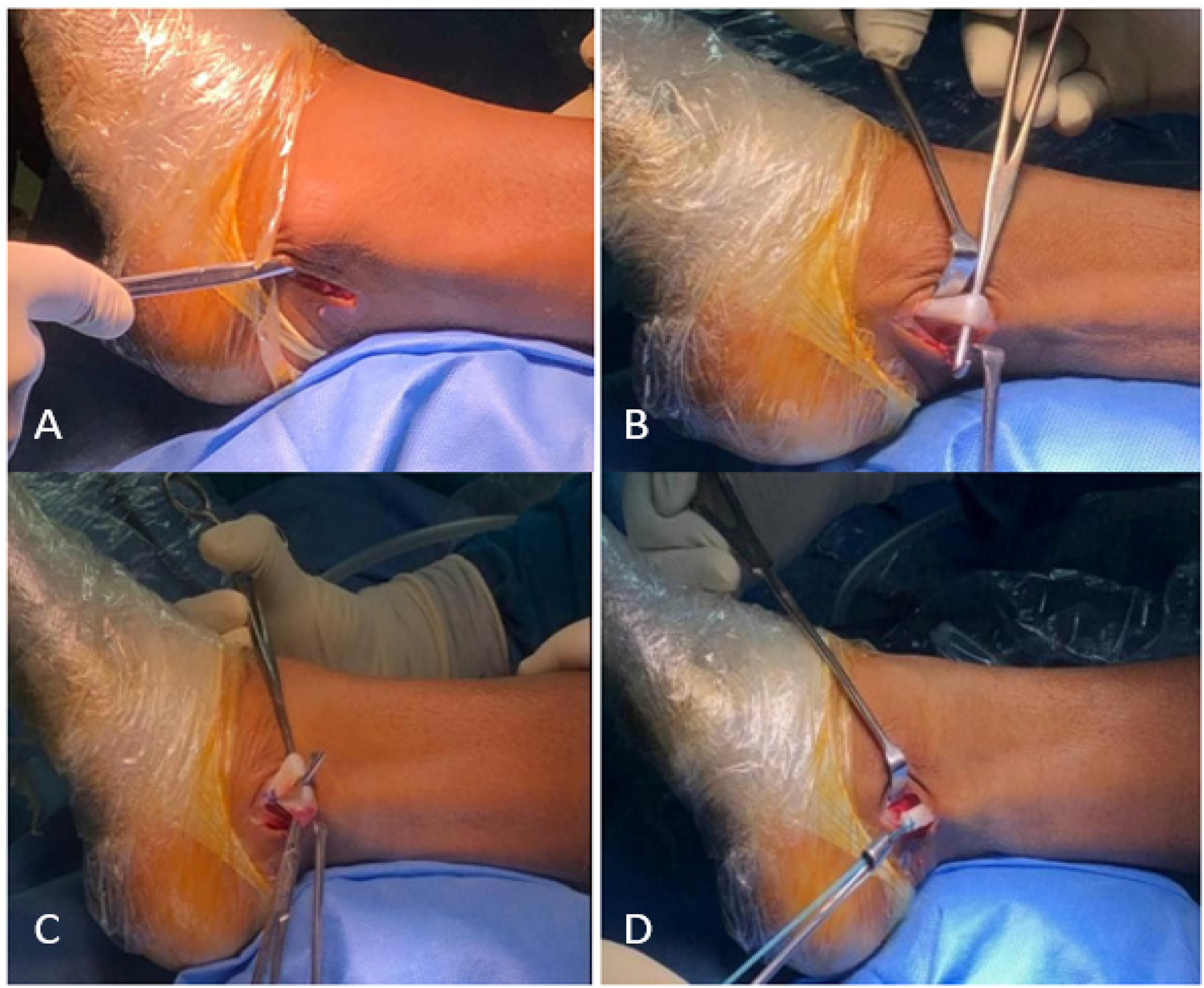
A- skin incision for graft harvest, B-identification of peroneal tendon, C-tenodesis of PLT to PBT, D-tendon stripping.
Rehabilitation
Patients were discharged 5 days post-surgery after two check dressings. Both groups were treated with the same standard physiotherapy protocol.
In the first 2 weeks, knee flexion was started up to 90o along with quadriceps and hamstrings strengthening exercises, ankle pump exercises, active straight leg raising with knee brace with complete extension and toe touch weight-bearing with knee brace in extension supported by a walker. In the following 3–6 weeks, full range of knee flexion, stationary cycling, weight-bearing as tolerated. Walker was weaned off depending on quadriceps strength. Ankle eversion strengthening exercises were advised to patients belonging to the peroneus longus group. By 6–12 weeks, the knee brace was discontinued, and partial squatting was started. After 6 months patients could return to sports activity. Knee band support was advised for contact sports, during jumping and landing activities for 1 year.
Results
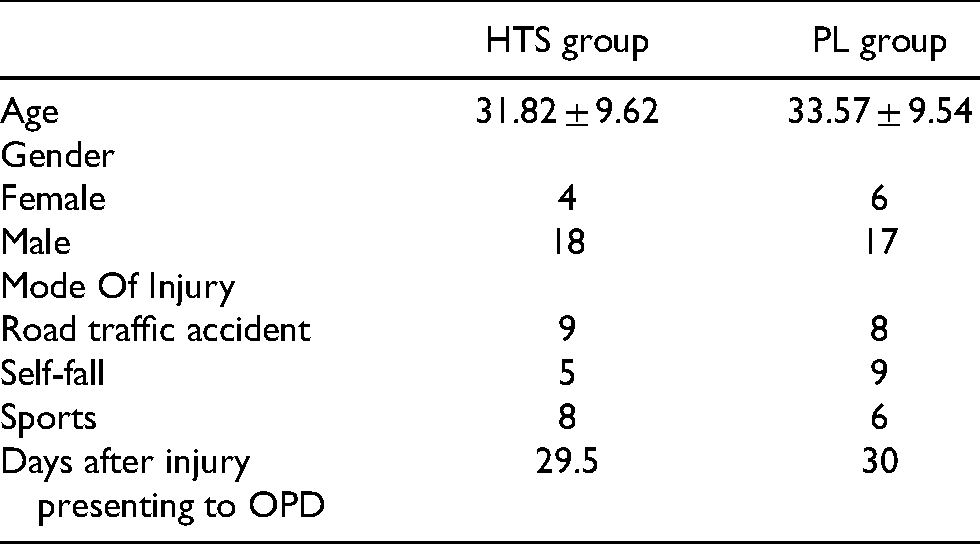
Among the 45 patients selected for this study, 22 patients were included in the HST group and 23 patients in the PL group by simple computer randomisation. Among them 35 were males and 10 were females. Road traffic accidents were the commonest mode of injury followed by self-fall and sports injuries. (Table 2). The surgical site infection rate was more in the HST group (3patients) than in PL group (1 patient). After wound debridement and resuturing, the wound gradually healed. 6 patients developed kneeling pain in the HST group. No patients developed any ankle pain, numbness over the knee joint or ankle joint and limitation of the movement at the ankle joint.
Demographic data of study population.
The important findings in the present study were, PL autograft showed improved Lysholm score and modified Cincinnati functional scores. There was better knee flexion strength improvement at the end of 1 year in the PL group compared to the HST autograft group. AOFAS score also showed significant improvement at the end of 1 year in the PL group.
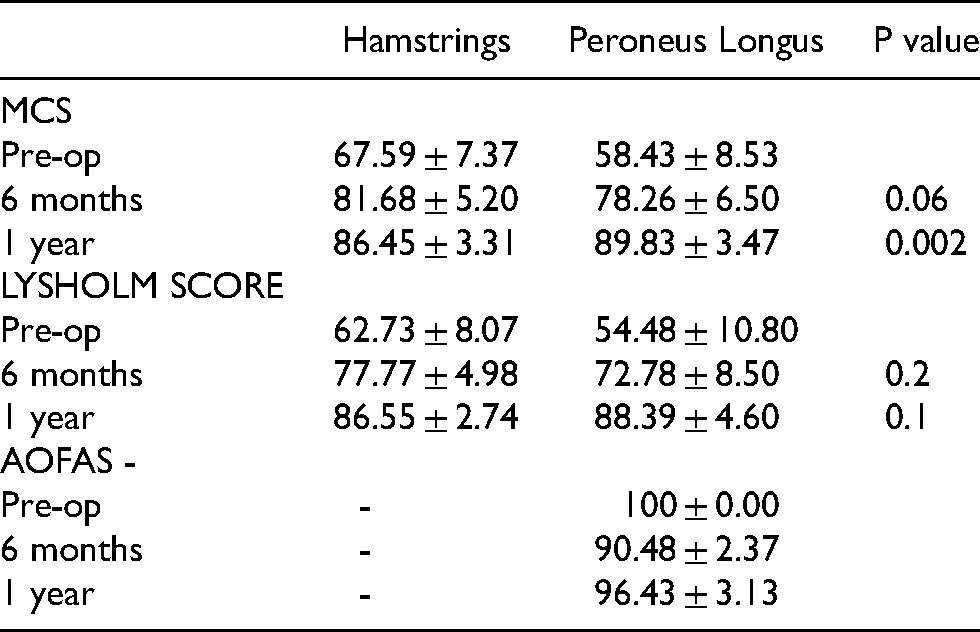
Analysing the functional outcome at 1-year follow-up, substantial functional improvement was seen in MCS score in both HST and PL groups but significant results in the PL group (p-value 0.002). Lysholm's score also improved in both the groups at 1-year follow-up. Whereas slight reduction in AOFAS score was observed at the end of 1 year but did not affect the ankle function. (Table 3)
Functional scores analysis of ACL reconstruction using HTS and PL autograft.
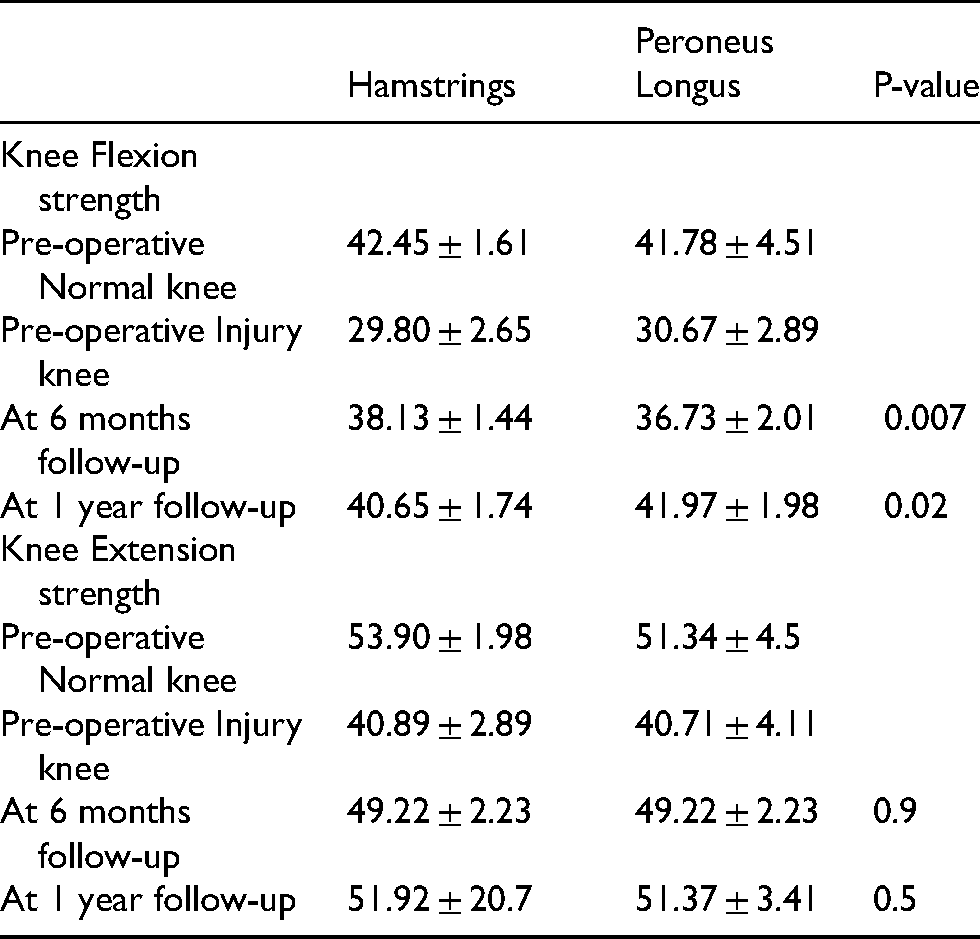
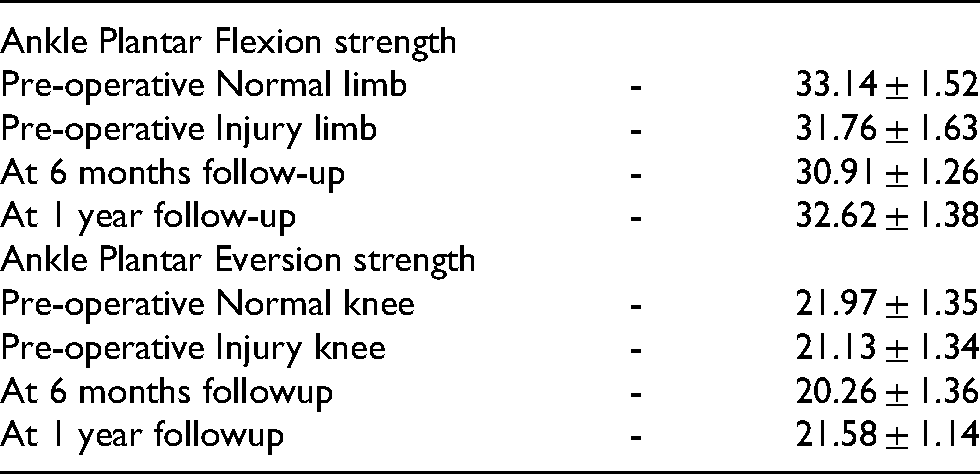
Comparing the donor site morbidity between the HST and PL group, knee flexion strength showed improvement in both the groups by the end of 6 months and 1 year of follow-up. A substantial enhancement was observed in the PL group than the HST group (p-value 0.02) because the hamstring tendon was sacrificed in the HST group giving an advantage of preventing early loss of knee flexion strength and range of movement. Analysing the knee extension strength, there was remarkable improvement at the end of 6 months and 1 year. Here the HST group scored better than the PL group. But when both the groups were compared the results were not significant (p-value 0.5). In the ankle, both plantar flexion and eversion strength were reduced in the PL group at the end of 6 months follow-up, but later improved at the end of 1 year but not up to the strength of the normal side. (Table 4)
Pre- and post-operative donor site morbidity of knee flexion and knee extension between HTS and PL group after 6months and 1 year.
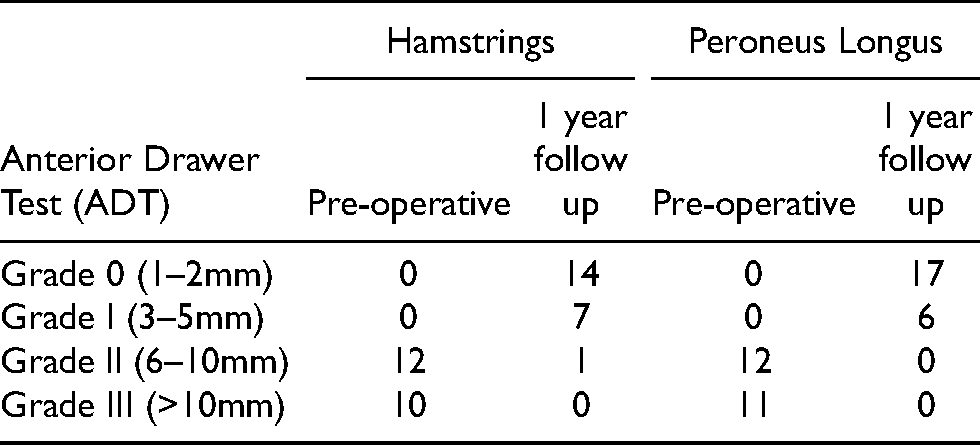
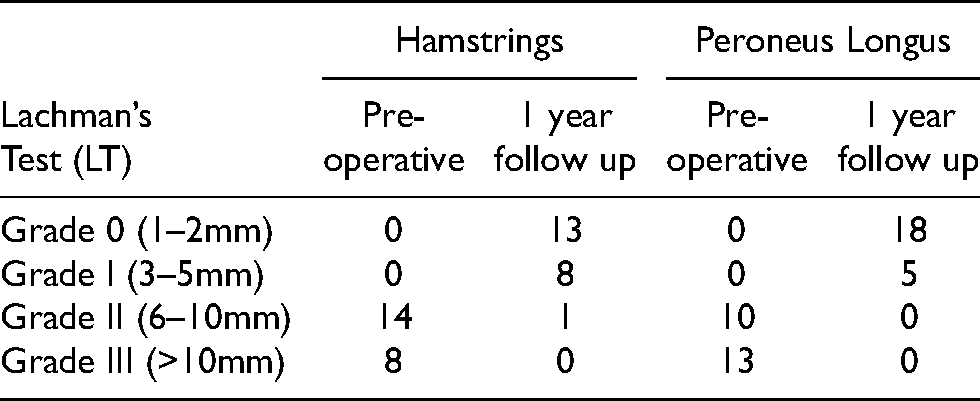
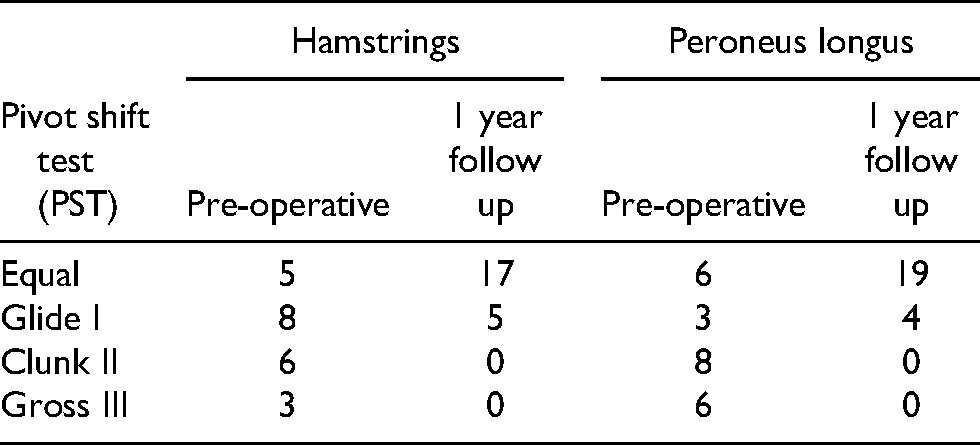
Anterior drawers test, Lachman's test and pivot shift test were done preoperatively during an examination of the knee joint to confirm the diagnosis and assess the amount of translation. postoperatively at 1year follow-up anterior drawers test, Lachman's test and pivot shift test were repeated to check for anterior translation. (Tables 5–8)
Pre and post operative donor site morbidity of ankle plantar flexion and eversion in PL group after 6 months and 1 year.
Anterior drawer test analysis in HTS and PL group pre and post-operative follow-up after 1 year.
Lachman's test analysis in HTS and PL group pre and post-operative follow up after 1 year.
Pivot shift test analysis in HTS and PL group
Discussion
Various studies reported good results after ACL reconstruction with the peroneus longus tendon, in terms of both functional outcome and knee stability.12–14 Our study supports that assertion. In this study functional outcome and donor site morbidity comparing PL and HST tendon autograft were evaluated which showed that the PL tendon can be used in single-bundle ACL reconstruction with good results at 1-year follow up.
Another study by Angthong mentioned donor site morbidities like reduced peak torque eversion and inversion, decreased ankle function and concerns about ankle stability in the PL group. 12 But in our study, the mean ankle eversion strength showed no statistical difference at the donor site compared to contralateral normal ankle eversion. No patients had any ankle instability or reduced ankle movements. The ankle function was good in the PL group (AOFAS mean was 96.43 ± 3.13) at the end of 1 year. A similar study was done by S. Rhatomy et al. also showed similar results in AOFAS score at end of 1 year without significantly affecting the ankle functions. 4
A study by Kerimoglu, PL has a minor effect in carrying the arch of the foot. Usually, PB and abductor digiti minimi maintain lateral longitudinal arch. Abductor hallucis, tibialis posterior and flexor pollicis longus look after medial longitudinal arch. Adductor pollicis and tibialis posterior maintain the transverse arch of the foot. 13 According to the literature, PL has no appreciable influence in maintaining the arch and stability of the foot. In our study, we have observed that none of the patients had ankle instability and loss of arch architecture at the end of 1 year
In our study, Anterior kneeling pain was also found in about 27% of patients after hamstring tendon harvesting. A similar study done by S.Rhatomy et al. observed 6% of patients developed anterior kneeling pain. 4 This symptom can be apprehension in patients where the daily routine includes kneeling on the ground as part of their religious practice which could lead to significant morbidity and reduced quality of life.
A study by Adachi N stated that the patients who underwent HST graft for ACL reconstruction, more loss of active knee flexion angle was observed and more peak torque angle was shifted to a shallow angle, suggesting that the HST strength may be weaker at the deep flexion angle. 15 In this study, we have seen that knee flexion strength reduced in the HST group at the end of 1 year compared to the normal contralateral knee which could be attributed to sacrificing the HST knee flexion component. But in the PT group, there was no decrease in knee flexion strength but instead, knee flexion improved.
Rhatomy et al. used a hand dynamometer for measuring plantar flexion and eversion in patients who underwent PL tendon usage for ACL reconstruction. They observed that at end of 6 months there was no difference in the plantar flexion and eversion strength compared to the normal contralateral side. 11 In this study, there was no statistical difference in plantar flexion and eversion strength of the donor side ankle compared to the normal contralateral ankle at the end of 1-year follow-up. This evidence shows that PL can be used as a promising graft with no effect on ankle eversion and plantar flexion power.
PL tendon along with PB tends to dispense pressure over the forefoot. 11 Karanikas found no difference in isokinetic strength for first ray plantar flexion of donor versus contralateral normal ankle. 16 In this study, similar observations were noted. This could be probably because of intact PB and tenodesis of distal stump of PL to PB. Otis et al. stated that PB is a more efficient evertor at the ankle joint and continues to be even after PL is harvested, and supports the usage of PL as a graft for ACL reconstruction. 17
A study on 25 patients to evaluate functional outcomes after ACL reconstruction using a triple-layered PL graft. Khajotia observed that there was an improvement in IKDC score with no patients having ankle dysfunction but 2 patients had pressure pain at the graft harvest site at the end of 6 months. 18
A systematic review and meta-analysis of functional outcome following hamstrings and peroneus longus autograft in ACL reconstruction in 925 patients. Jinshen et al. observed that Lysholm and IKDC score has improved better in peroneus longus group than hamstrings group. There was no difference in FADI but minimally reduced AOFAS score in peroneus longus group. He concluded that peroneus longus can be an ideal graft and can circumvent the complication of imbalance between quadriceps-hamstrings which happens following harvesting the hamstrings tendon. 19
There was no limitation of ankle eversion and first ray plantar flexion with good ankle motor strength. AOFAS analysis was 100% at end of 1 year and Wiradiputra et al. concluded that peroneus longus can be used as the first option in ACL reconstruction. 20
A 2 year follow-up of patients who underwent peroneus longus graft for ACL reconstruction by Sholahuddin observed that excellent IKDC, MCS, Tegner-Lysholm score, AOFAS, FADI scores. Good graft diameter was harvested, thigh hypotrophy was less, with excellent ankle function and a better serial hop test result was achieved. 21
Kusumastutia have done an observational analytical study retrospectively in 75 patients for 1 year. There was an improvement in mean IKDC, MCS, Tegner-Lysholm score, KSS (function), AOFAS and FADI scores at the end of 1 year compared to pre-operative. Eversion and plantar flexion strength were not significantly different between contralateral normal ankle and donor site. 3 patients had neuropraxia in the HST group and concluded that peroneus longus can be used as a promising graft for ACL reconstruction. 22
Various studies have shown the ability of peroneus longus usage in ACL reconstruction as an alternative promising graft with minimal or no donor site morbidity apart from other available grafts. However, further studies could focus on measurements of ankle stability and strength and correlate them with functional scores after harvesting the peroneus longus tendon.
Limitations of the study include, ligament laxity was checked manually which can have inter-observer bias. Instead, a KT1000 arthrometer could be used. Muscle strength measurement with an isokinetic dynamometer would have been more accurate.
Conclusion
PLT has a greater ultimate tensile load, more thickness and length, less graft harvesting time, and almost no donor site morbidity and has a good functional outcome of the knee, making it an effective and safe autograft option. So, PL autograft can be a promising graft of choice in the reconstruction of the ACL and can be much more beneficial in simultaneous multi-ligament injury repair in the knee joint.
Footnotes
Abbreviations
Author’s contribution
V and S were responsible for enrolling the patients generating the research question and analysing the scores.
AC was responsible for patient's follow-up, calculation of scores and statistical analysis.
A contributed in analysing the scores and final preparation of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.