
Abstract
Introduction
Anterior cruciate ligament (ACL) reconstruction is the frequent arthroscopic surgery with more than 100,000 cases per year in The United States 1 and about 12,000 cases annually in Thailand. 2
Although surgeons widely agreed that the most important factors affecting successful ACL reconstruction are position of both femoral and tibial tunnels, strength and size of graft should not be ignored. There are many graft options for anterior cruciate ligament reconstruction with the most common choices being bone patellar tendon bone graft and hamstring tendon graft. 3 Hamstring tendon is easy to harvest, less morbidity, but may reduce hamstring power and may cause thigh hypotrophy. 4 Bone patellar tendon bone graft may allow faster return to sport, while may cause kneeling pain and knee stiffness. 5 In some situations which need several grafts for reconstruction as in multiple ligament injury, there are options like quadriceps tendon graft, peroneus longus tendon graft, allograft, or contralateral grafts can be used. The ideal graft should have enough strength, easy and safe to harvest, and dispensable. Peroneus longus tendon can be easily harvested therefore it can be used as an alternate graft choice. Several studies demonstrated acceptable biomechanics of peroneus tendon as graft choice in anterior cruciate ligament reconstruction. 4 Concerns about donor site morbidity are controversial, some studies reported no clinically significant donor site morbidity,4,6 while others reported some morbidity after entire peroneus tendon graft removal. 2
Peroneus longus plays an important role in foot and ankle biomechanics, entire removal of the graft may possibly affect function in some way. Recently, anterior half of peroneus longus tendon (AHPLT) was suggested as an alternate choice to whole peroneus tendon with acceptable length, sizes, and quality. 3 Size of tendon is another concern regarding graft choice. It is widely accepted that a graft of minimum diameter of 7 mm is recommended. 7 In general, Asian population have smaller stature compared to Caucasians, 8 we hypothesize that this may contribute to smaller AHPLT graft diameter which affect its longevity and functional results.
This study aimed to compare physical examination and functional outcome using The International Knee Documentation Committee (IKDC) subjective score between AHPLT graft and conventional hamstring graft for ACL reconstruction.
Methods
This retrospective cohort study was approved by the hospital ethic committee and included patients age 15–55 years and body mass index (BMI) between 18–35 kg/m2 who underwent anterior cruciate ligament reconstruction with anterior half peroneus longus tendon and hamstring tendon from January 2015 to December 2016 in the provincial hospital. The exclusion criteria were patients with collateral ligament instability grade II or above, previous ligament reconstruction, previous knee osteoarthritis Kellgren-Lawrence; KL-II or above and patient loss to follow-up before 3 years. Preoperative physical examinations including Lachman test, anterior drawer test, and pivot shift test were performed. Self-administration of the IKDC subjective score (Thai version) was collected. 9
All patients were operated with standard anatomic single bundle ACL reconstruction by single experienced orthopedic surgeon. Anterior half peroneus longus tendon was harvested using 3 cm long skin incision starting 2 cm proximal from distal tip of lateral malleolus extending in proximal direction. The peroneus tendon can be identified under the skin, the sheath was opened along its fibers, and the peroneus longus was separated from the peroneus brevis. A stab incision was performed in the middle of the peroneus longus tendon, separated anterior and posterior portion along its fiber, then a suture loop was used to sling around anterior half of the peroneus longus tendon. The ankle was placed in plantar flexion and eversion, anterior half of the peroneus longus tendon was released about 1 cm proximal from the distal tip of lateral malleolus. The free end of the tendon was sutured, the tendon harvester was moved proximally and the free graft was retrieved through distal incision. The sheath around the peroneus tendon was closed, subcutaneous and skin closure was done afterwards (Figure 1).
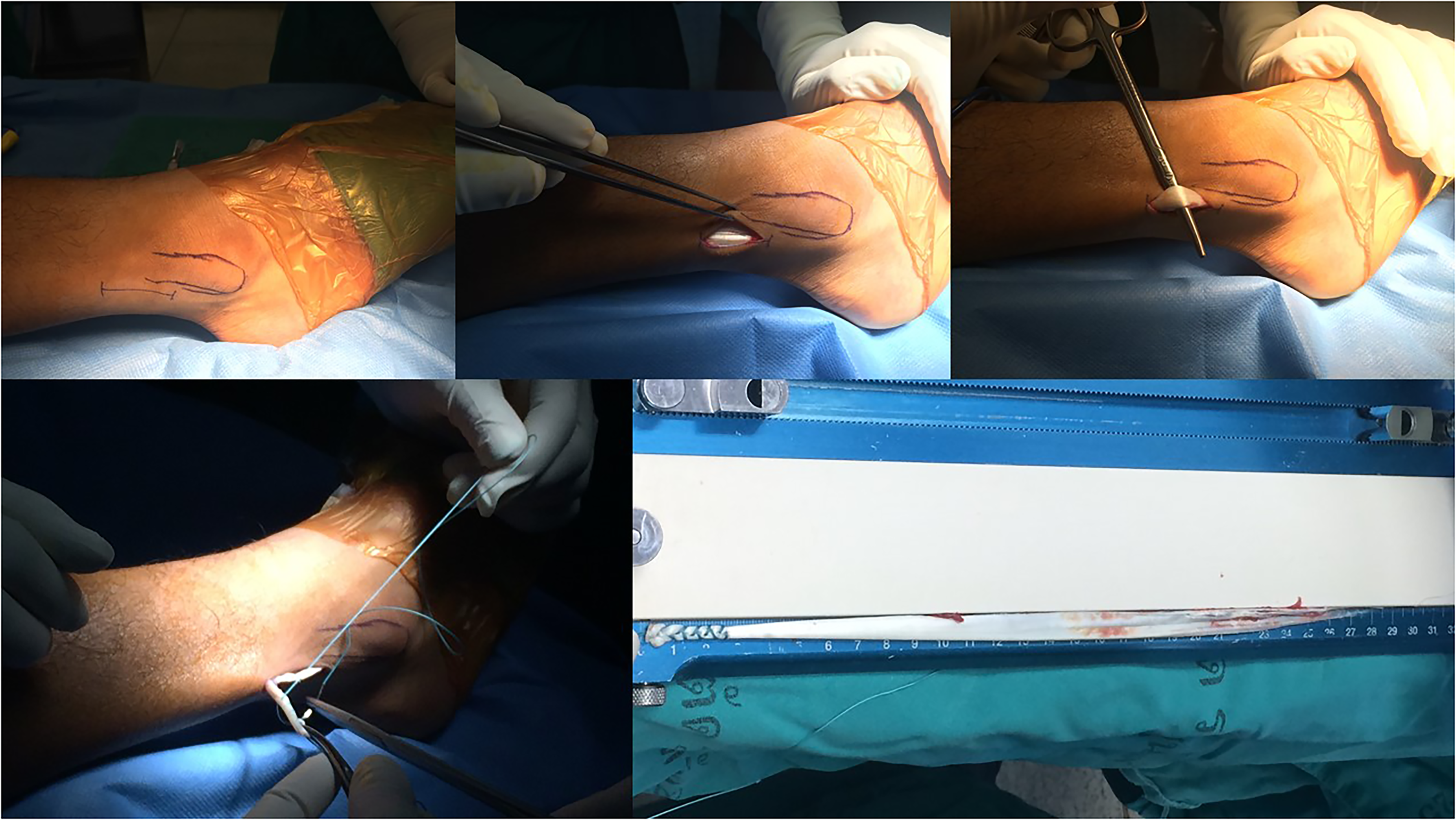
The anterior half of peroneus longus tendon graft harvesting.
Hamstring graft was harvested in standard fashion, the semitendinosus tendon was used as single graft if applicable. The gracilis tendon was harvested as an additional graft if quadruple semitendinosus tendon graft size was less than 7 mm in diameter. Standard anterolateral and anteromedial arthroscopic portals were created. Meniscus and cartilage surgery were done as necessary. All patients were operated with standard anatomic single bundle ACL reconstruction. The femoral tunnel was created based on the identified anatomic footprint, with the center placed at the lateral bifurcate ridge and below the lateral intercondylar ridge. The tibial tunnel was based on the anterior horn of lateral meniscus and ACL stump insertion site. The femoral fixation of the graft was done with suspension device (XO button, Conmed Linvatec, FL, USA), while the tibial fixation was done with interference screw (Genesys Matryx, Conmed Linvatec, FL, USA).
All patients received the same rehabilitation protocol, an adjustable frame with four-point fixation knee brace was applied for a month, 0–60 degree flexion for two weeks and unlocked afterward. Partial weight bearing was allowed after two weeks and full weight bearing was allowed after a month. All patients were scheduled for follow-up at 2 weeks, 2, 4, 6, 12 months, 2, 3 years post operatively and IKDC at 3 years were collected to determine the functional outcome. Complications such as paresthesia, ankle instability were collected at immediate postoperative time and along with the follow-up periods.
Data were analyzed using mean and standard deviation for continuous variables, and using frequency with percentage for categorical data. The unpaired t-test, and Fisher's exact test were used to compare each factor between groups. For non-normally distributed continuous variables, median (range), and Mann Whitney U test was applied. Regression analysis was done to identify factors related with IKDC, and binary regression (relative risk and 95% confidence interval; CI) for those associated with postoperative anterior drawer test. Factors that had p-value < 0.1 were considered as potential confounding factors and were brought into multivariate analysis. The parsimonious final model was selected. All statistical analysis was performed using STATA 16.0, StataCorp, College Station, Texas, USA. Significant p-value was < 0.05.
Results
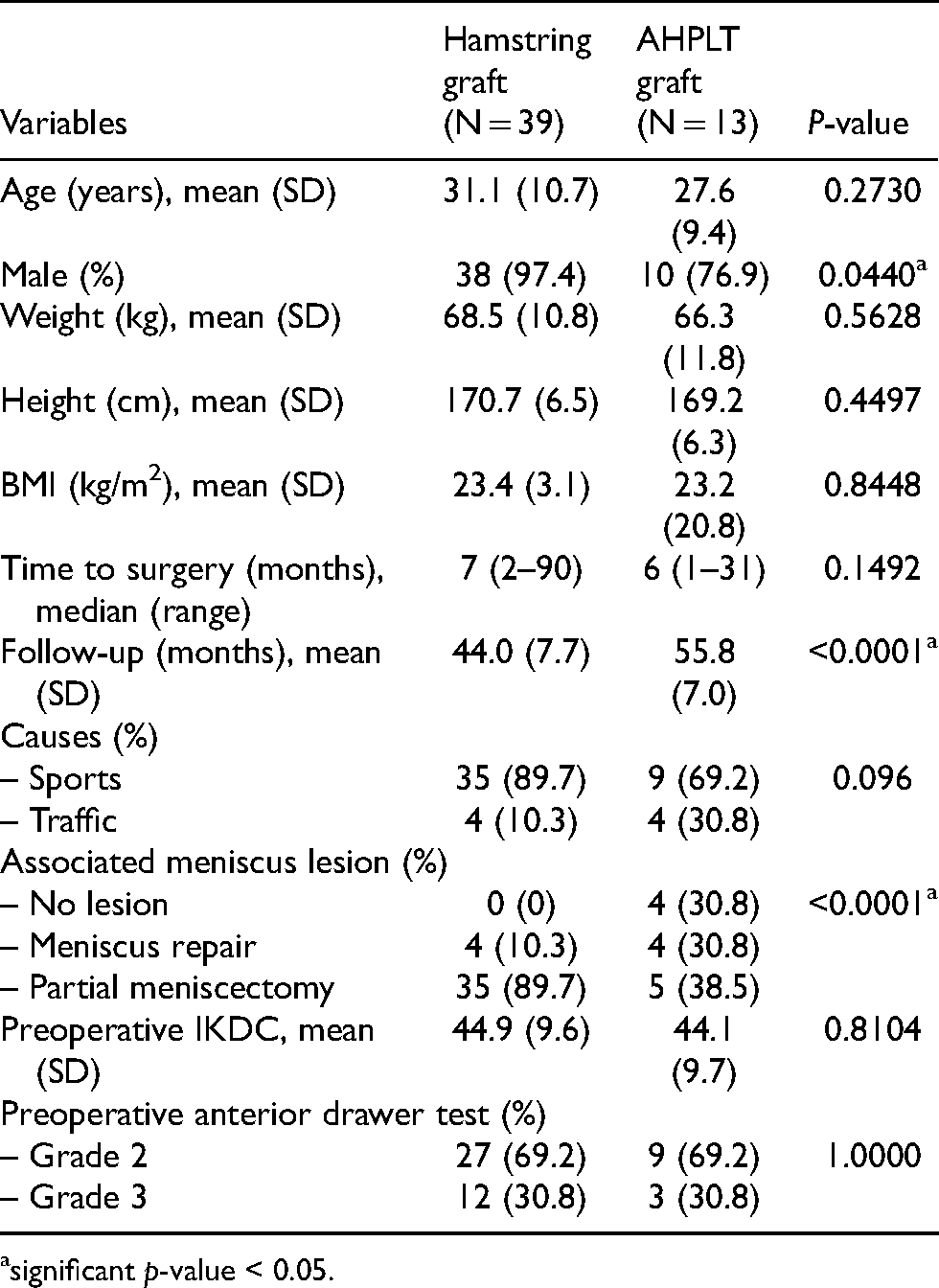
Fifty-two patients met the inclusion and exclusion criteria were included in the study (13 in AHPLT group and 39 in hamstring group). Mean age was 27.6 ± 9.4 years in AHPLT group and 31.1 ± 10.7 years in hamstring group. Ten patients [76.9%] were male in AHPLT group while 38 patients [97.4%] were male in hamstring group. Weight, height, body mass index, and time to surgery were not statistically significant between groups. Sports injuries were the most common cause of ACL torn in this study. Preoperative IKDC score was 44.1 ± 9.7 in AHPLT group and 44.9 ± 9.6 in hamstring group. Preoperative physical examinations were comparable in both groups (Table 1).
Demographic data.
significant p-value < 0.05.
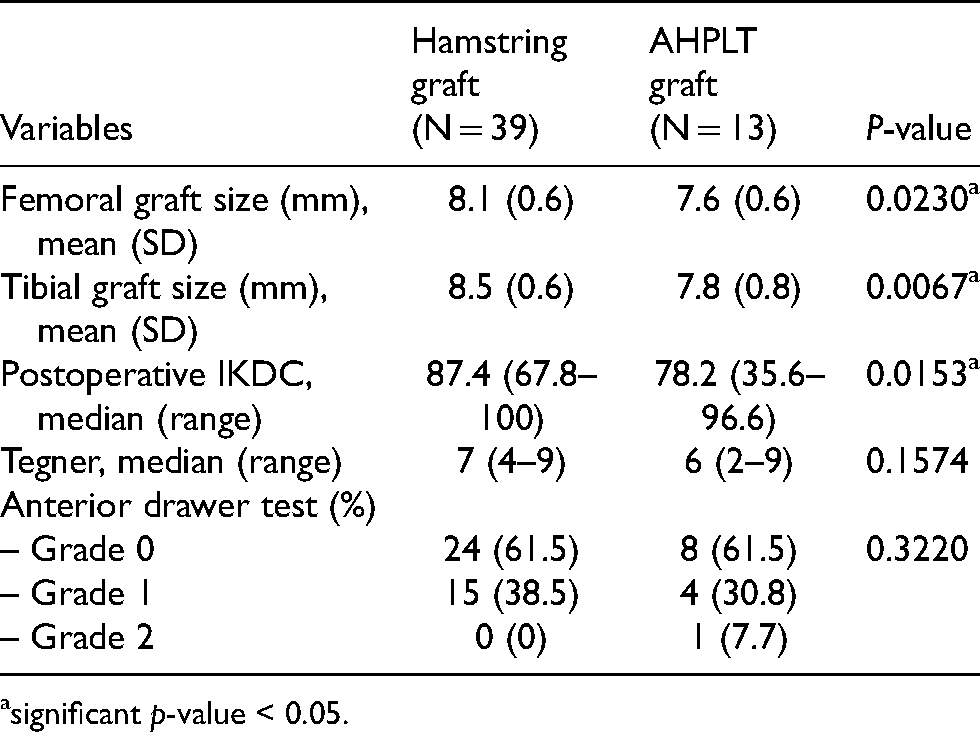
Associated meniscus lesions were found in the majority of both groups and partial meniscectomy were done mostly. Femoral graft size was 7.6 ± 0.6 mm in AHPLT group and 8.1 ± 0.6 mm in hamstring group, while tibial graft size was 7.8 ± 0.8 mm in AHPLT group and 8.5 ± 0.6 mm in hamstring group respectively.
Postoperatively, one patient in the AHPLT group underwent revision ACL reconstruction with hamstring graft after two years due to re-rupture. A patient was needed to harvest hamstring tendon after small AHPLT harvest and was included in the hamstring group and a patient in the hamstring group underwent another meniscus repair after 1 year postoperatively. There was no significant complication or morbidity in the foot and ankle functions in any of the patients.
Mean follow-up time was 55.8 ± 7.0 months in the AHPLT group and 44.0 ± 7.7 in the hamstring group. At final follow-up, Tegner activity level was comparable in both groups, physical examinations regarding anterior drawer tests were also comparable. On the other hand, IKDC score at 3 years postoperatively was statistically better in the hamstring group; 87.4 (67.8–100) compared with 78.2 (35.6–96.6) in AHPLT group (Table 2).
The comparison of outcomes between groups.
significant p-value < 0.05.
Regression analysis of each factor associated with postoperative IKDC score was shown in Table 3 and all of the potential confounding factors were brought in the multiple regression analysis as shown in Table 4. The parsimonious model revealed graft types and gender were the most optimal variables that explained postoperative IKDC score.
Regression analysis of each factor associated with postoperative IKDC score.
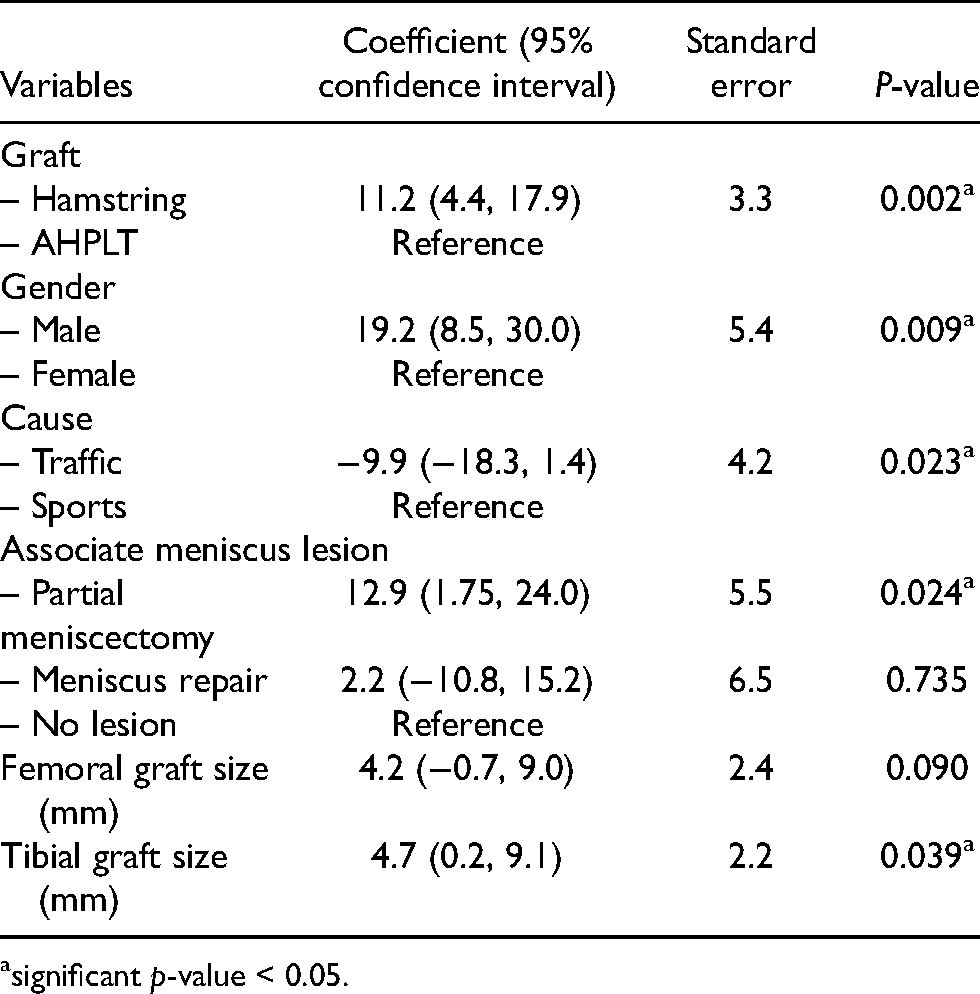
significant p-value < 0.05.
Multiple regression analysis of factors associated with postoperative IKDC score.
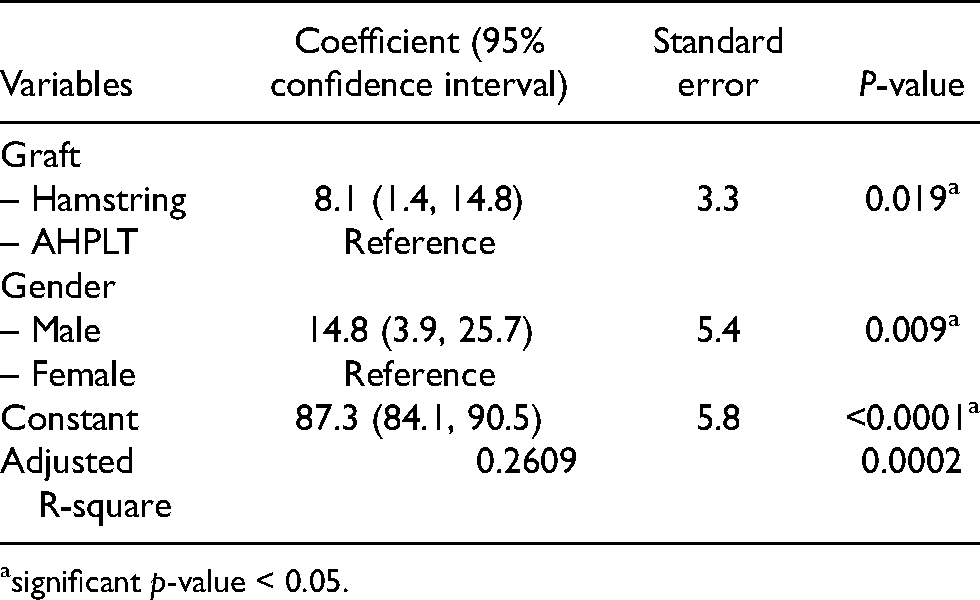
significant p-value < 0.05.
Discussion
Recently anatomic ACL reconstruction has become more popular as it is thought to restore normal knee function, however a single or double anatomic bundle is to be considered. Some studies found benefit of double bundle ACL reconstruction as it showed better result controlling anterior and rotational stability. 5 But some studies found that there is no differences between both groups in terms of knee stability, function or patient satisfaction.10,11 In this study we performed single anatomic ACL reconstruction creating femoral tunnel based on previous footprint according to lateral bifurcate ridge and lateral intercondylar ridge, while tibial tunnel was created based on previous stump site. We found that AHPLT group had lower IKDC score at 3 years when compared to the standard hamstring graft. Graft types and gender were significant factors contributed to the functional score.
Previous studies have confirmed that peroneus longus tendon graft can be used as an alternative graft in ACL reconstruction.4,12 Although it is still controversial regarding possible donor site morbidity after harvesting entire tendon, peroneus longus has a major role in foot and ankle function. It is one of the main evertors of the ankle which participates in all three planes, full thickness harvest of the graft may possibly affect functions in some way.2,13,14
Zhao and Huangfu proposed the use of AHPLT as an alternative to entire tendon, studied biomechanical properties and found that it is acceptable for use as autograft with respect to its strength, safety, and donor site morbidity. 3 Park et al. found that partial harvesting of peroneus tendon did not cause significant impairment of tendon strength in the isokinetic test or loss of ankle joint motion. 6 Furthermore, after partial thickness harvesting, peroneus longus tendon was found to regenerate according to MRI study and regenerated tissue signal characteristics were nearly indistinguishable from those of the normal tendon. The quality of regenerated tendon from partial thickness harvest was better than that of full thickness harvest. 15 Average load of failure of AHPLT was comparable with that of semitendinosus tendon and about 1.5 times that of gracilis tendon. 3 It can be easily harvested from superficial location of distal leg and it has no juncturae tendinum and adherence to surrounding structure like semitendinosus and gracilis tendons. Unlike previous literatures, although physical examinations at the end of the follow-ups show no differences between two groups, the most significant finding of our study was that anatomic single bundle ACL reconstruction using AHPLT graft had lower postoperative IKDC functional score compared to hamstring graft at 3-year follow-up. Our study used anterior half of peroneus longus tendon and found that the graft size was significantly smaller than that of hamstrings. Although we did not collect postoperative foot and ankle functional scores, the complications according to donor sites were unremarkable.
Graft diameter affects re-rupture and revision rate after ACL reconstruction. Reduction in hamstring diameter is related to a higher revision rate especially in young patients. 16 Smaller hamstring autograft size is a predictor of poorer 2 years after primary ACL reconstruction and higher revision rate with graft size less than 8 mm. 17 Many studies tried to establish correlation between anthropometric parameters and graft diameter of peroneus longus. Short and thin patients were more likely to have smaller graft diameter (<8 mm), especially who ruptured their ACL more than 3 months. 18 The study of Sakti et al. propose that patients with body weight less than 44 kg, less than 153 cm in height, or less than 72 cm of true leg length should be considered as high risk for having a PL tendon diameter less than 7 mm, which reflected to higher failure rate of ACL reconstruction. 19 We found that postoperative IKDC score was associated with gender and tunnel sizes (Table 3). Multiple regression analysis demonstrated the smaller stature in female gender and AHPLT graft sizes may lead to unfavorable postoperative score (Table 4). Females were shorter and had smaller graft sizes than males. Four included females had average height 164.2 ± 4.4 cm and weight 71 ± 12.9 kg, while 48 included males had average height 170.8 ± 6.3 cm and weight 67.7 ± 10.9 kg. Averaged AHPLT graft at femoral size was documented as female 7.0 ± 0 mm versus male 7.8 ± 0.6 mm, and tibial size as female 7.2 ± 0.3 mm versus male 8.0 ± 0.7 mm. Averaged hamstring graft at femoral size was revealed as female 7.5 ± 0 mm versus male 8.1 ± 0.6 mm, and tibial size as female 8.0 ± 0 mm versus male 8.5 ± 0.6 mm. Overall graft size among males was larger than 7.5 mm, therefore, we did not find any failure of ACL reconstruction at 3 years of follow-up.
There were some limitations in this study. The main weakness of this study is small number of participants in the AHPLT group. We used only physical examination to determine the knee stability, though no differences were found, these examinations which are subjective test, may prone to error. We did not report donor site morbidity due to lack of sufficient data but we believed there were minimal and insignificance as shown in all previous literatures. However, the findings in this study may raise concern regarding use of AHPLT graft in small stature patients. Further study should collect more factors affecting results, the rate of return to sports, donor site morbidity for both groups, and include larger number of patients.
In conclusion, AHPLT graft can be an alternative choice to conventional graft for single anatomic ACL reconstruction with less donor site morbidity, however there must be concern for smaller graft in short and thin female patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.