
Abstract
Background
Although participation in sports and exercise is promoted widely due to its health benefits, sports-related injuries can also be a detriment to an individual's health and a burden for the healthcare system. Herein, the aim of this study is to provide a comprehensive review on the epidemiological profile and the risk for surgery of athletes presented to a sports injuries clinic in Hong Kong.
Methods
A total of 566 patients attending the sports injuries clinic at a local hospital between October 2017 and September 2018 were reviewed. Only 271 patients sustaining injuries from sports activities were included. These patients attended a survey-based data collection session, which recorded their demographic, injury site, events leading to injury, exercise details (type, level-of-play, frequency, experience), and functional score according to the injury site.
Results
The highest proportion of injuries was observed in amateur athletes (45.4%) than in recreational (28.8%) and professional (25.8%). Those patients aged between 18–29 years old (50.2%) had the most injuries. Both soccer (25.1%) and basketball (25.1%) were the two most common sports to incurred injuries. Whereas, the lower extremities being the most common injured sites. Based on our logistic model, athletes with less experience were more prone to required surgeries with injuries in the lower extremities.
Conclusion
Preventive measures should be targeted at less experience athletes, focusing on strengthening the knee region, to reduce sports-related injuries and surgeries. Importantly, this study demonstrates the need to further identify factors to develop effective sports injury prevention programmes for tailoring athletes at different levels-of-play.
Background
Sports participation has become increasing popular in modern society. To encourage public well-being, the local government in Hong Kong has actively promoted sports participation. Although the facilities and recreational areas for sports have increased dramatically these few years, the education on safety and awareness toward sports injuries remains limited. And in 2004, the Hong Kong Sports Institute Limited (HKSI) was established to provide an environment in which sports talent can be identified, nurtured, and developed to pursue excellence in sport. Other than sports facilities, the support given to athletes includes elite coaching and training, sports science, sports medicine, strength and conditioning, athlete affairs and education, applied research, and sports information.
It has been well established that exercise is known to be beneficial to one's health. However, the risk of injury is somehow inevitable. In the United States alone, there are nearly 2 million people every year who suffer from sports injuries and require immediate treatments. 1 While in Hong Kong, a survey indicated that 9% of the respondents who participated in sports activities in the last 12 months had been injured at least once and the injury episode was serious enough to limit their normal activities. 2 With such embodiment, this inevitably creates a massive burden towards the treatment from the local healthcare system.
Recent studies of changes in sports participation found that general participation in sports has increased in the past two to three decades, especially participation in non-club organised sports. 3 Most often, when recreational sports players and athletes sustained injuries, they may choose very different choices of treatment. In addition, often, the untimely treatment could result in the need for surgery and delay their recovery for return-to-play. Treatment at a sports medicine clinic would incur a better outcome owing to the range of practitioners that can be jointly involved at the same time and location.
In the early 2000's, an epidemiological study on the amount of sports-related injuries attending the Accident & Emergency at a local hospital in Hong Kong was conducted. 4 As reported, during the 1-year period, those sustained sports injuries accounted for 12% of all Accident & Emergency attendances. 4 Upon the increase in sports participation for the past 20 years, the newest consensus showed that more than 5000 sports injury cases (with over 500 new cases) were needed to be managed annually at a local sports injuries clinic in Hong Kong. 5
Multiple theories have been produced to analyse sports injury prevention by identifying risk factors 6 and defining the relationship between workload and injury. 7 Although previous studies have performed such sports injuries epidemiology, these findings were over a decade ago and did not highlight the surgical rate or severity.4,8–10 As the timing of return-to-sports after surgery for a sporting injury varies across the type of sport and injury, 11 this is a common challenge for orthopaedic surgeons ranging from the choice of treatment to the design of the rehabilitation programme. And with advances and changes in the sporting culture, we would like to provide an update on the sports injuries data in terms of incidence, diagnosis, severity, high-risk groups, and those requiring surgical management to produce effective preventive measures. As Hong Kong remains one of the most influential cities in Asia, the finding may help to facilitate sport injury prevention programme in other Asian countries. Herein, the aim of this study was to provide a comprehensive review on the epidemiological data of sports injuries on patients attended a local hospital's sports clinic across one year.
Methods
Participants
The study design was approved by the local institutional review board (IRB), and informed consent was obtained from each patient or from parents/guardians of minors prior to the start of this study. All 566 patients attending the sports clinic in Hong Kong from the period October 2017 to September 2018 were invited to participate in this study (Figure 1). The patients, who attended the sports injuries clinic, following a referral from another doctor, have all claimed to be injured during sports participation. Exclusion criteria will include (1) the patient's inability to communicate or read English and Chinese and (2) the lack of consent being obtained.
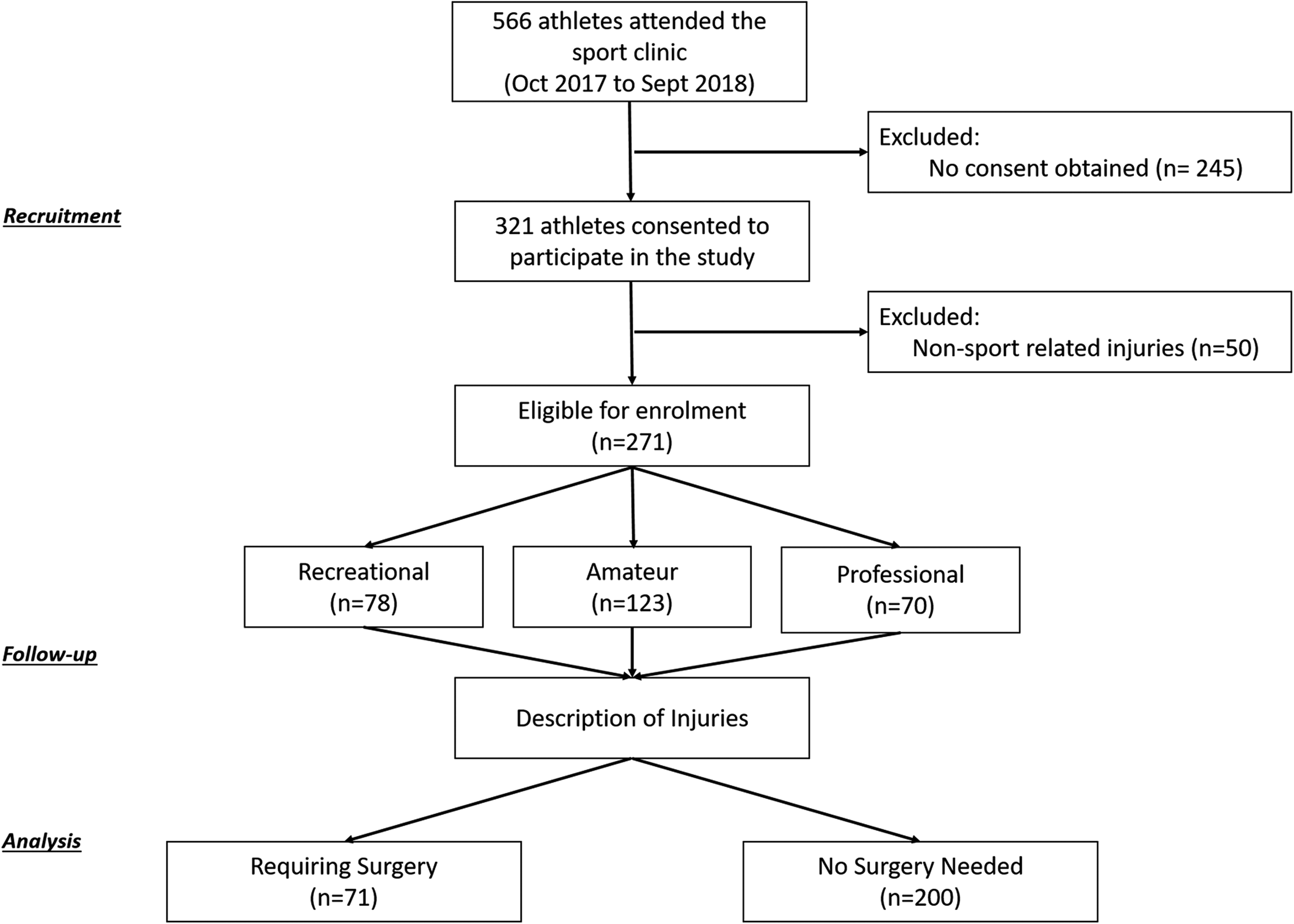
CONSORT for patient recruitment.
Measures
A sports injury reporting form was filled by patients or their accompanying guardian (Supplementary 1). The following variables were collected: age at presentation, gender, anatomical location of injury, type and severity of injury, cause of injury, type of sports played, level (recreational, mid-level amateur, and high-level amateur), injuries afflicted during training or competition, and initial management of the injury.
These patients were then grouped as recreational, mid-level amateur, or high-level amateur athletes. High-level amateur athletes were defined as those receiving elite training from the HKSI and competing regularly in competitions and local sports clubs. Whereas mid-level amateur athletes are defined as those remaining athletes receiving regular training from the HKSI and competes in the mid-level amateur level of sports. Finally, the recreational participants performed some form of non-competitive physical activity on a regular basis.
In addition, once the anatomical location of injury has been identified, additional information was collected on assessing the symptoms of injuries from the following questionnaires: the International Knee Documentation Committee (IKDC) Subjective Knee Form (Supplementary 2) for assessing the knee injuries and the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire (Supplementary 3) for assessing upper limb injuries. The IKDC is a patient-oriented questionnaire that assesses symptoms and function in activities of daily living. The DASH questionnaire is a 30-item questionnaire that looks at the ability of a patient to perform certain upper extremity activities.
Statistical analysis
Descriptive data were presented as means ± standard deviations, medians [interquartile ranges], and frequencies (proportions). Overall prevalence and characteristics of injuries occurring in the recreational, mid-level amateur, and high-level amateur levels were then assessed. Means of outcome measures were compared using Chi-square test and analysis of variance (ANOVA). Data analysis was performed by SPSS (version 23.0, IBM). A p-value < 0.05 was considered to be statistically significant.
Results
Demographics
Of the 566 patients attending the sports clinic, 321 patients were consented to participate (response rate 56.7%). Among these consented patients, 271 were found eligible to participate in this study. The majority of the participants were male (64.6%), aged between 18–29 years old (50.2%), and were amateur athletes (45.4%). The full demographic details can be found in Table 1.
Participant characteristics for recreational, amateur and professional athletes visiting the sport clinic.
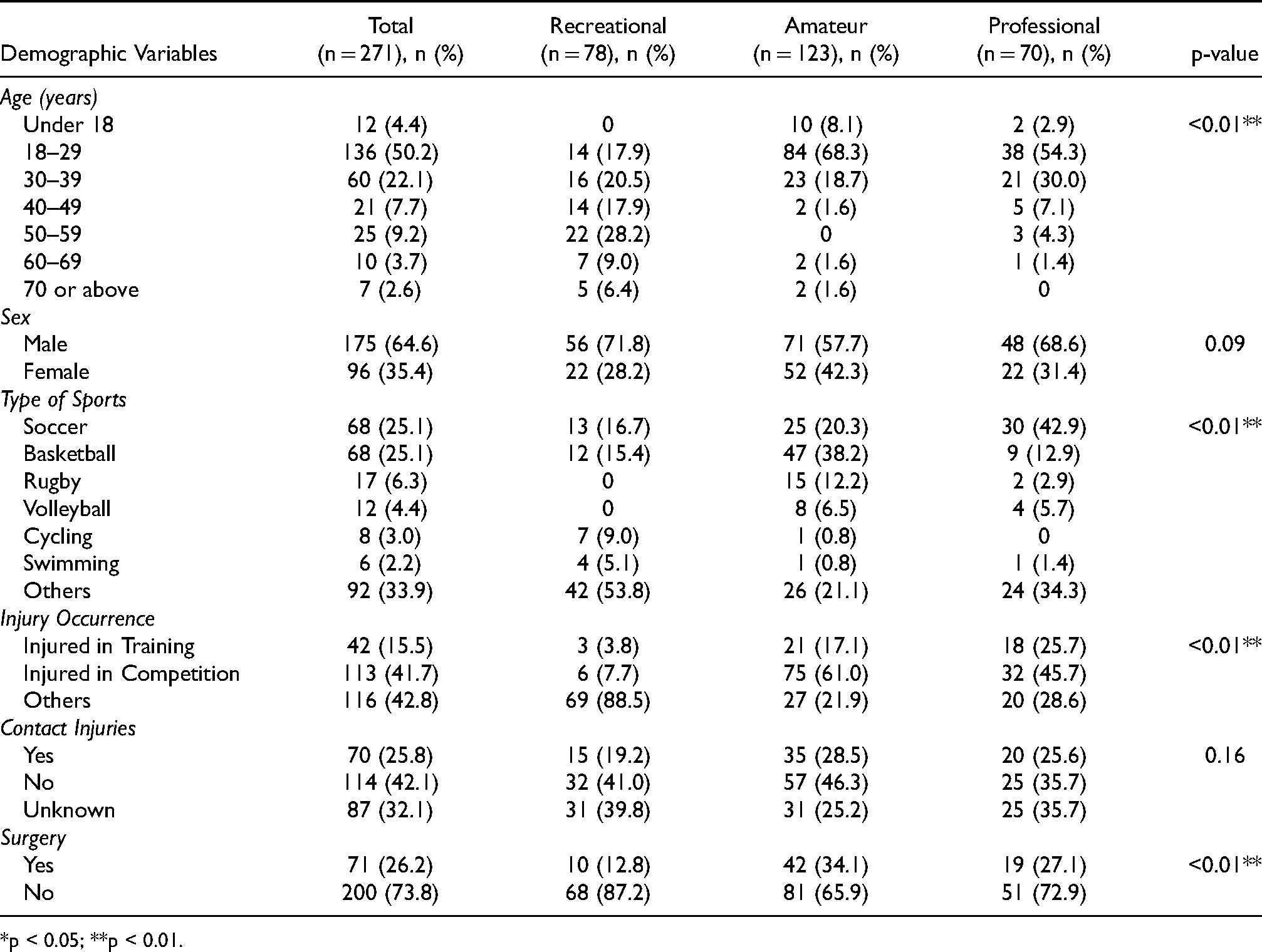
*p < 0.05; **p < 0.01.
Clinical diagnoses and sports
In general, soccer (25.1%) and basketball (25.1%) were the most common sports to have injuries (Table 1). As found, male athletes were more likely to be injured during soccer (35.4%) and basketball (28.6%), while female athletes have more injuries in basketball (18.8%) and rugby (12.5%).
The knee was predominantly the most common site of injury (55.5%) and shoulder injuries were second (17.7%) (Figure 2). As the knee and shoulder injuries were the two most common injured sites, we further analysed in depth by evaluating their severity with functional scores. The IKDC and DASH were used to assess the severity of knee injuries and upper limb extremities injuries, respectively. Knee injuries in the recreational setting were found to have the lowest level of function and highest symptoms (Figure 2A). Similarly, upper limb extremities injuries in the recreational setting were found to have the highest disabilities (Figure 2B). The correlation between age and severity, as measured by the functional scores of IKDC and DASH (Figure 3). There was a statistically significant correlation between older age and lower level of function with knee injuries (R = –0.16, p = 0.04) and increased disabilities with shoulder injuries (R = 0.34, p < 0.01).
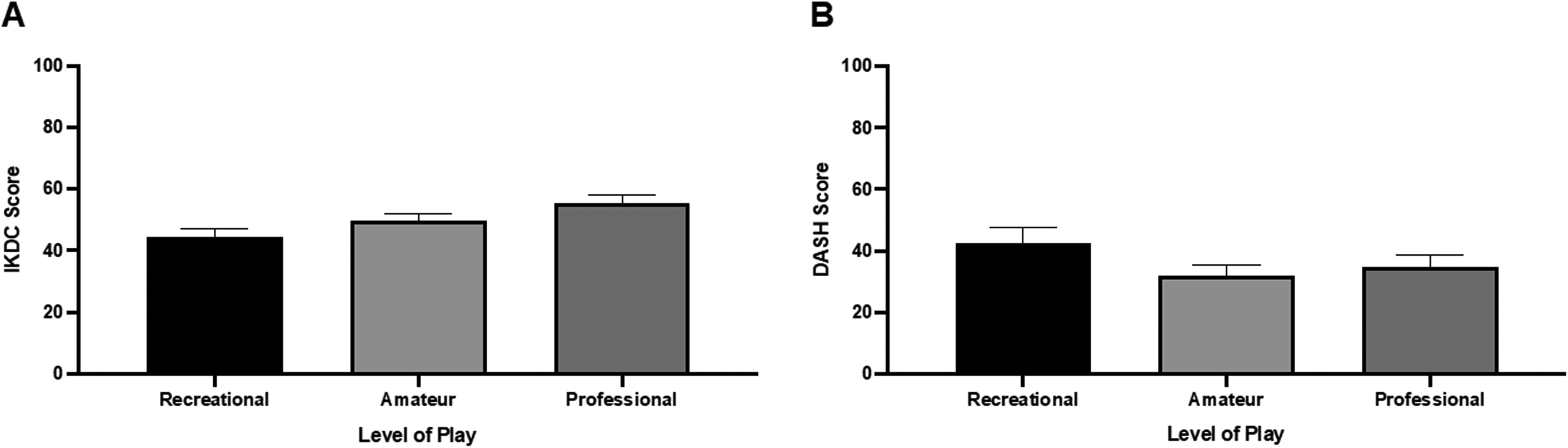
Additional evaluations on the severity in patients with knee injuries and upper limb extremities injuries. (A) International Knee Documentation Committee (IKDC) Subjective Knee Form was used to evaluate the level of function and symptoms in patients with knee injuries. When presented at our sports clinic, recreational athletes have shown the lowest level of function and the highest level of symptoms than mid-level amateur athletes and high-level amateur athletes. (B) Disabilities of the Arm, Shoulder, and Hand (DASH) Form was used to evaluate the level of disabilities in the patients with injuries in the upper limb extremities. Similarly, when being presented to our sports clinic, recreational athletes showed the most severe disability than mid-level and high-level amateur athletes.
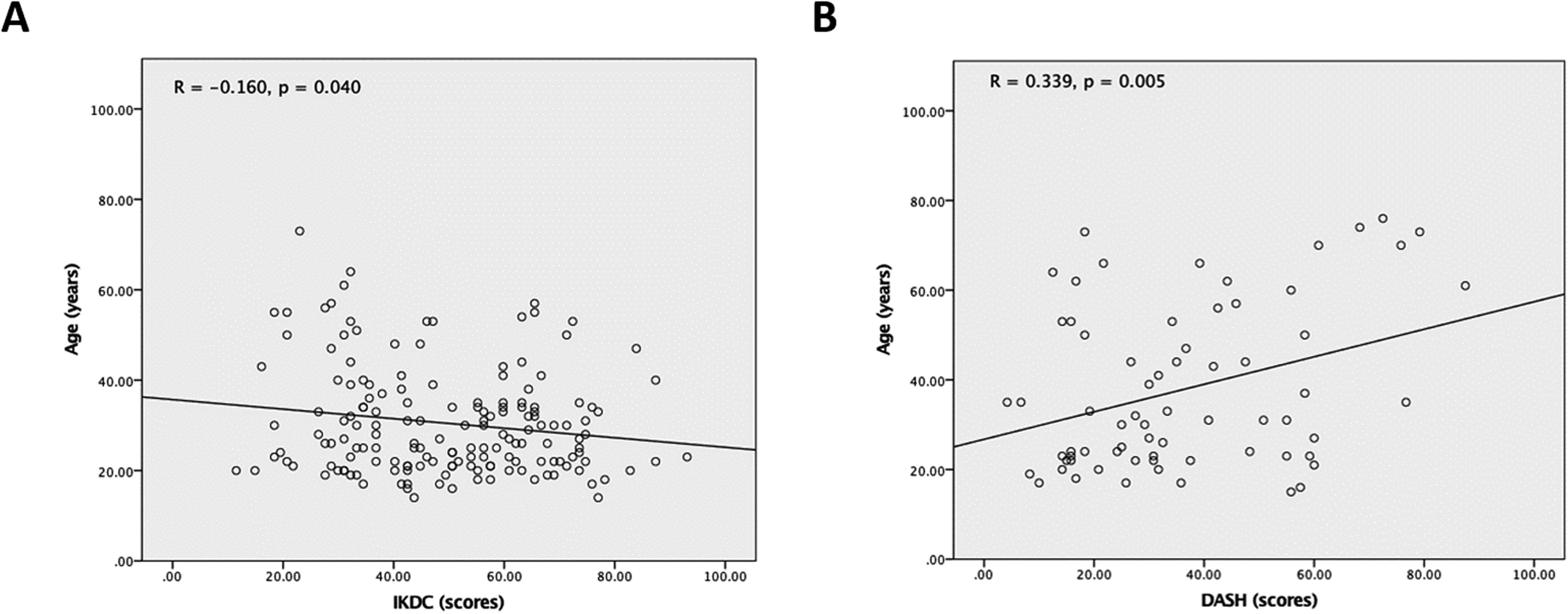
Correlation with age on severity and disability toward injuries to the knee and upper extremities. (A) A significant negative correlation between age and IKDC scores was found. This indicated that injuries in older athletes would result in the lowest level of function and the highest level of symptoms when presented with injuries in the knee. (B) A significant positive correlation between age and DASH scores was found. This indicated injuries in older athletes would result in more disabilities upon injuries to the upper extremities.
Whereas, most of these injuries were sustained during competition (41.7%) rather than during training (15.5%) (Table 1). Non-contact injuries (42.1%), such as pivoting imbalance and awkward landing, were the main cause for their visit to the sports clinic. Among the 271 patients attending this clinic, only 71 patients (26.2%) required surgical operation for treatment of the injury. Among those injuries that required surgical operation for treatment, these occurred the most in basketball (24 cases; 33.8%) and soccer (18 cases; 25.3%) injuries, especially during competitions (45 cases; 63.4%). The lower extremities of the knee region received the most operations (65 cases; 91.5%) and the age group of 18–25 years old received the most operations (47 cases; 66.2%).
The difference in injuries sustained from level of play
Recreational
Of those, completing the survey, 78 recreational athletes (28.8%) attended the sports clinic (Table 1). The majority of respondents were male (71.8%) and older than 30 years of age (82.0%). The main sites of injuries are the knee (55.8%) and shoulder (27.9%) (Table 2). As recreational athletes seldom need to participate in intense training and competition, they sustained injuries mainly from other non-collision reasons (e.g. fall, hit by obstacles, etc.) (88.5%) (Table 1). Only 10 injuries (26.2%) would require surgical attention.
Injury characteristics a .
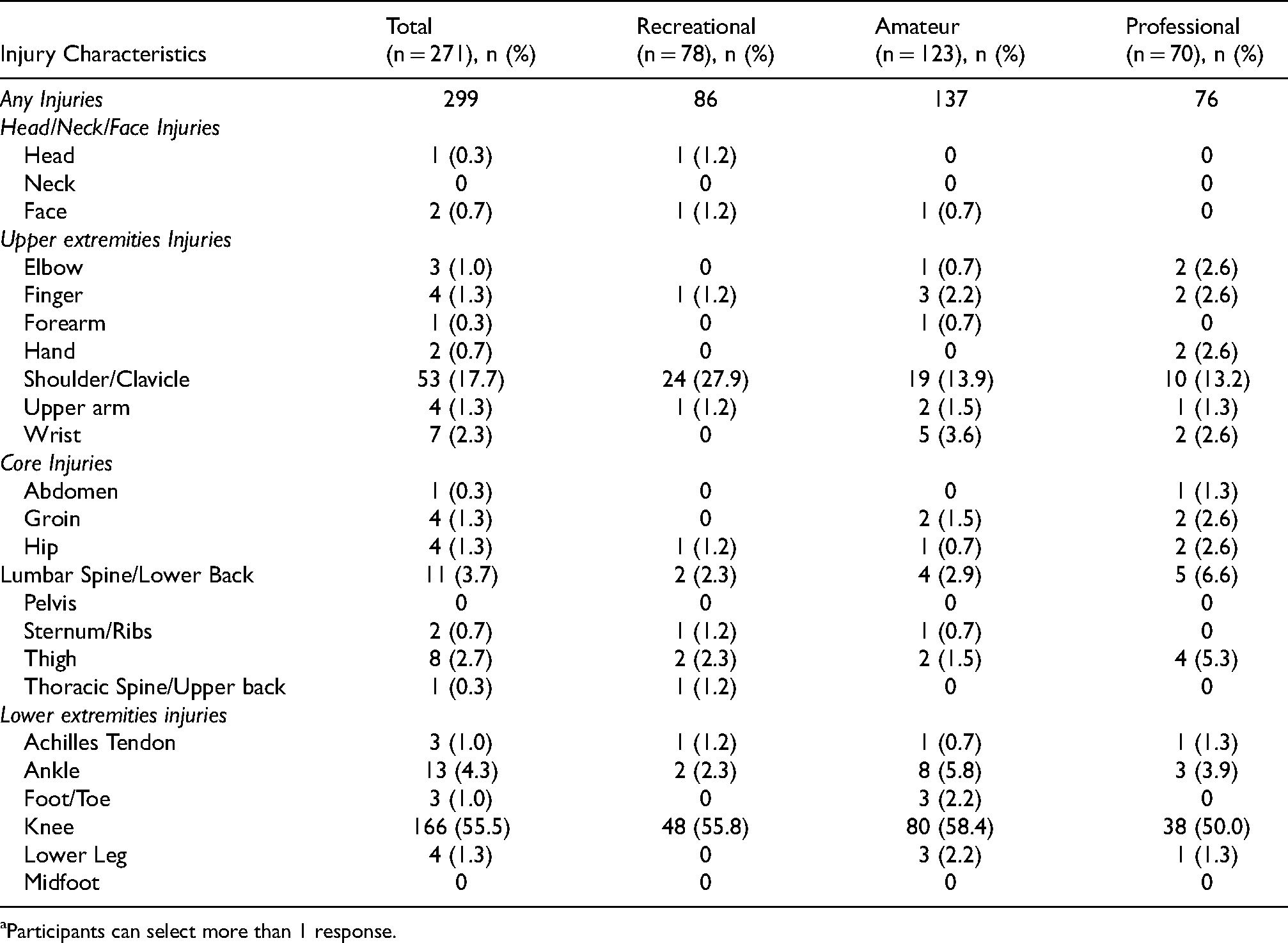
Participants can select more than 1 response.
Mid-level amateur
Of those, completing the survey, 123 mid-level amateur athletes (45.4%) attended the sports clinic (Table 1). The majority of respondents were male (47.7%) and younger than 30 years of age (76.4%). Basketball (38.2%) was the main sport resulting in these injuries. The main site of injuries is the knee (58.4%), followed by shoulder injuries (13.9%) (Table 2). They sustained injuries mainly during competition (61.0%) from non-contact reasons (e.g. sprained knee, improper landing, etc.). In addition, among these injuries, 42 injuries (34.1%) would require surgeries.
High-level amateur
Of those, completing the survey, 70 high-level amateur athletes (25.8%) attended the sports clinic (Table 1). The majority of respondents were male (68.6%) and younger than 30 years of age (56.3%). Soccer (42.9%) was the main sport resulting in these injuries. Similarly, the main sites of injuries are the knee (50.0%) and shoulder (13.2%) (Table 2). They sustained injuries mainly during competition (45.7%) from non-contact reasons (e.g. sprained knee, improper landing, etc.). Only 19 injuries (27.1%) require surgical correction.
Previous consultations
A majority of the injuries were referred by the Accident & Emergency Department (25.3%), which is followed by referral from physiotherapists (22.8%) and orthopaedics specialists (22.0%) (Table 3). When we further evaluated these referrals based on the level of play, 40 out of the 116 injuries in recreational athletes were referred from the Accident & Emergency Department to the sports clinic for follow-up. In mid-level and high-level amateur athletes, injuries were mainly referred to our sports clinic by physiotherapists. Surprisingly, 37 of these injuries received no previous consultation when arriving at the sports clinic for treatment. As it can be seen, a majority of these injuries without previous consultations were from the mid-level amateur (15 cases) and high-level amateur athletes (16 cases). As our centre also serves as the main consultation for the local sports institute, these injuries arising from mid-level amateur and high-level amateur athletes can come directly to our sports clinic for treatment without needing referral.
Previous consultations a .
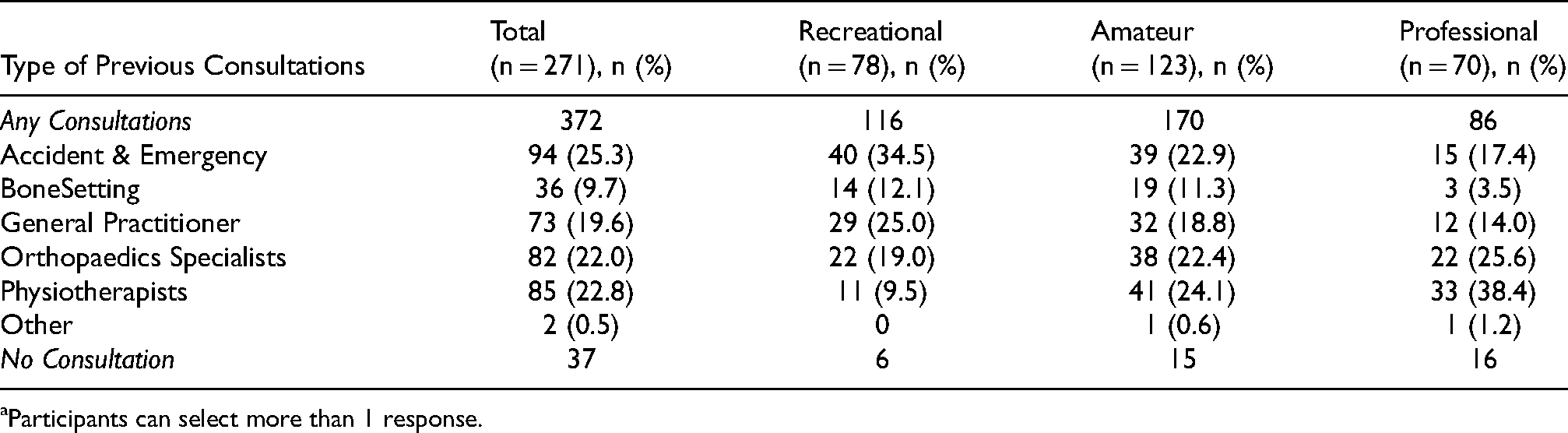
Participants can select more than 1 response.
Factors associated with requiring surgical treatment after injury
Recreational athletes were significantly less likely to have had surgical intervention than those in athletes with amateur (OR, 3.37; 95% CI, 1.01–11.25) and professional (OR, 4.96; 95% CI, 1.34–18.41) levels of play. Similarly, we found that the chance for requiring surgery following injuries in an athlete is 1.083 times higher with 1 year less experience in that sport. Similarly, the injuries in the lower extremities (mainly the knee) have a higher likelihood to result in surgical attention (OR, 9.84; 95% CI, 3.09–31.34). On the contrary, we did not find evidence that gender, age, weeks after injury, training versus competition injury, or whether the presence of contact collision was significantly associated with requiring surgery. However, this analysis was exploratory in nature (Table 4). Based on our logistic model, amateur and professional athletes with less experience were more prone to required surgical treatment after inflicting lower extremities injuries.
Binary logistic regression of characteristic associated with surgery outcome (unadjusted).
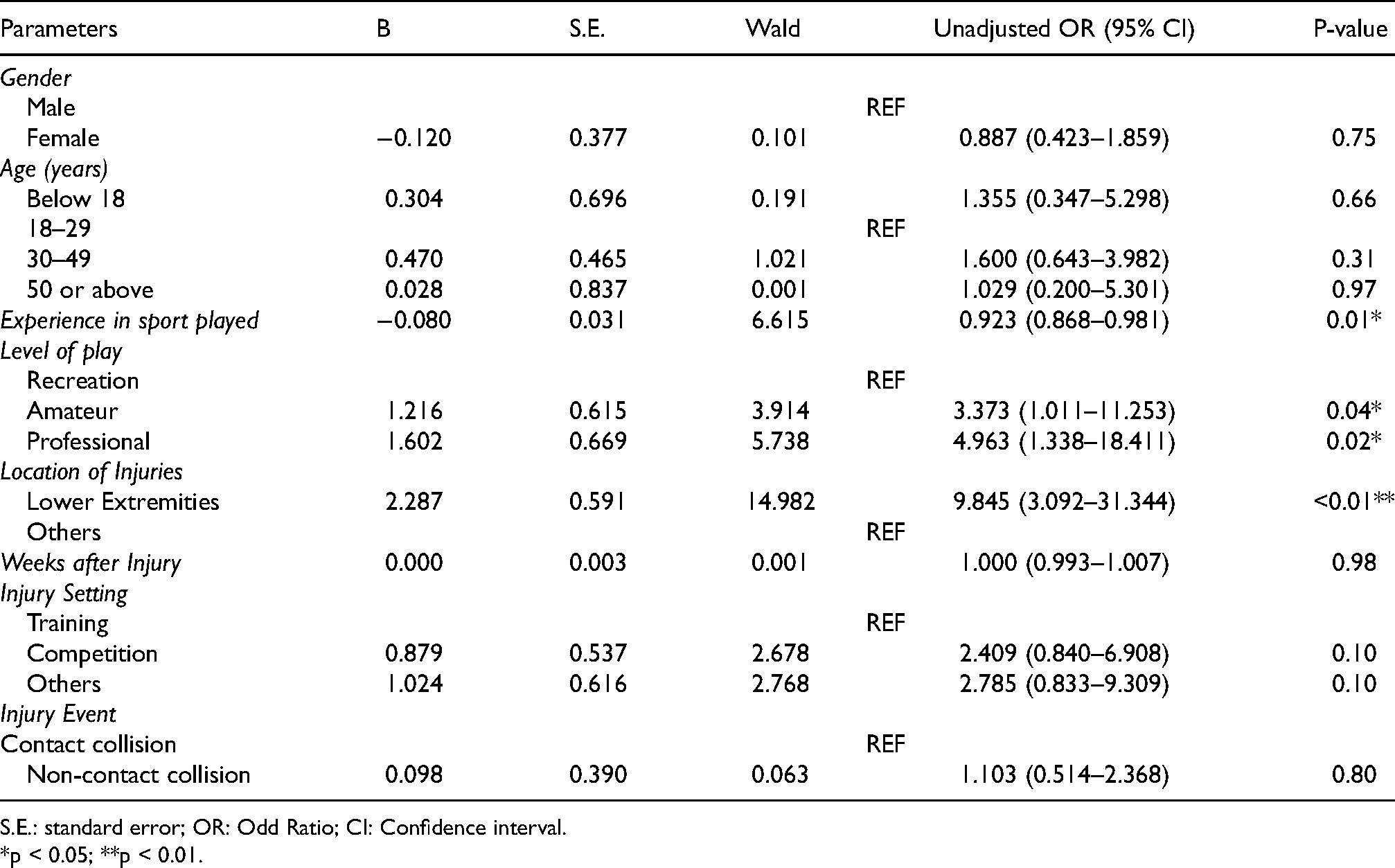
S.E.: standard error; OR: Odd Ratio; CI: Confidence interval.
*p < 0.05; **p < 0.01.
Discussion
To allow participation in sports to be beneficial rather than detrimental, effective measures to prevent sports injuries would be crucial. Sports injuries can be presented and interpreted in various directions, such as sport discipline (team or individual), body region, and type of injury (acute or chronic). 12 As first described by van Mechelen's model, the aetiology and mechanism of sports injuries can be highlighted by addressing the risk factors of the causation of sports injuries. 6 These risk factors can be classified into intrinsic versus extrinsic factors and modifiable versus non-modifiable factors. 12 Whereas, the epidemiological results generated from our current study highlight the non-modifiable risk factors leading to sports injuries. This may enable us to identify the high-risk groups that are prone to sports injuries for generating effective preventive measures.
In general, the majority of respondents attending our sports injuries clinics are male young adults (18–29 years old), which is consistent with previous studies.4,9,13,14 Similar to our earlier reports, it showed that soccer and basketball still remained as the main sports to incur the most sports-related injuries needing medical attention in the athletes. 9 In terms of the site of injuries, the knee and shoulder were the most prevalent among the three levels of athletes. Further analysis on the relationship on the severity with age was conducted. Our findings showed that older patients were significantly correlated with more disability and pain in knee and shoulder injuries (Figure 3). This may be a normal physiological response, as age is known to be a risk factor for sports injuries.15,16 Likewise, older athletes have been associated with a higher probability of reoccurring old injuries than younger athletes. 17 Hence, sports prevention programmes should be developed to target older athletes to reduce the likelihood of incurring sporting injuries.
In terms of finance, personnel, and resources, surgical management is the main burden to the healthcare system. Our data revealed that injuries from basketball and soccer players during competitions in young adults (aged 18–25) required surgical management of the knee region. To further investigate the factors that influence the need for surgical treatment, our logistic model revealed that amateur athletes were significantly more likely to receive knee surgeries than recreational or professional athletes. This was also compatible with the result of the most severe injuries being in the amateur group and in the knee region. Although surgery can relieve the patient's immediate concern, it may bring upon a negative long-term sequalae toward the patient's health. Additionally, certain knee surgeries can increase the risk of osteoarthritis. 18
In our study, it seemed amateur athletes generally resulted in more patients requiring surgical attention. Based on our logistic model, amateur and professional athletes with less experience were actually more prone to required surgical treatment after injuries in the lower extremities. It has been shown that appropriate high levels of training have a protective effect against sports injuries. 19 Our study offers a preliminary overview of the relation between the level of the specific sport and the severity of the injuries to raise awareness in a specific cohort in the public. Previous studies on the epidemiology of sports injuries only highlighted the type of sports or the injury profile of a specific sport. Both knee and shoulder injuries were the most severe in the recreational setting. However, the majority of all the injuries occurred during competition rather than training. This phenomenon may be the result of the lack of proper warm-up and stretching prior to amateur competitions in comparison to the professional cohort as warm-up and stretching are known to prevent sports-related injuries. 20 In addition to the epidemiological model used to highlight the intrinsic and extrinsic factors, 21 a recent model has been established on highlighting the physiological and psychological factors that influence the athlete and addressed that proper physical training may have a positive effect on sports injury tolerance. 22 To further appreciate the complete picture, a comprehensive model of injury causation was developed. 23 It hypothesised that the stress and load on the susceptible joint may not directly lead to injury but exposes the joint to a vulnerable situation, especially in athletes with reduced neuromuscular control. Thus, specific biomechanical training and prevention programmes aiming to improve neuromuscular control will reduce sporting injuries.
Sports prevention programmes can be broadly classified into active and passive strategies. 12 Passive strategies include the modifiable extrinsic factors that do not require active participation by the athlete, such as, but are not limited to new safety rules, regulations, and equipment. Specific prevention programmes, such as neuromuscular training and correction of endangering movement patterns, are known to be effective.24,25 A well-known comprehensive active prevention programme, “The 11 + ” developed by the International Federation of Association Football (FIFA) has been successfully applied to young female soccer players. 26 The FIFA 11 + has also been proven to effectively reduce the rate of anterior cruciate ligament (ACL) injuries in male soccer players. 27 A meta-analysis found that various types of neuromuscular and educational interventions appear to reduce ACL injuries by half. 28 The efficacy can also be improved by adding visual feedback to regular training regimes, especially for male athletes. 29 Therefore, effective sports prevention programmes in our locality should be targeted in less experienced professional athletes in strengthening their lower extremities, especially the knee region, and by applying the aforementioned programmes.
The findings of our study should be interpreted with the following limitations. Firstly, this study was limited from the respondent sample that mainly came from a single local hospital from our sports injuries clinic. Another concern would be on the consistency and accuracy of the information collected from a patient's self-reported survey, e.g., type of injury, type of surgery, time missed (competition/training), and specifics regarding frequency of play. Despite these limitations, this study has shown the importance on the need for clinicians and physiotherapists to identify potential risk factors on developing effective sports injury prevention programmes for different levels of athletes.
Conclusion
This study is a valuable start to a potential sports registry for sports injury prevention in Hong Kong. The data concluded that soccer and basketball were still consistently the most common type of sports to result in injury. Knee injuries were the most prevalent site for injuries requiring clinic attendance. Based on our logistic modelling, the injuries in lower extremities in amateur and professional level of sports with less experience would generally result in a higher likelihood for surgery when injured than in other parameters. Nevertheless, all sport participants should be informed regarding the significant risk of injury in the lower extremities. Importantly, proper instruction regarding appropriate precautions and safety protocols should be addressed.
Supplemental Material
sj-pdf-1-otr-10.1177_22104917221082314 - Supplemental material for Risk of surgery and epidemiological profile of athletes presenting to a single sports injury clinic in Hong Kong
Supplemental material, sj-pdf-1-otr-10.1177_22104917221082314 for Risk of surgery and epidemiological profile of athletes presenting to a single sports injury clinic in Hong Kong by Ashley Ying-Ying Wong, Gene Chi-Wai Man, Yuen-Man Wu, Hiu-Wun Wong, Michael Tim-Yun Ong and Patrick Shu-Hang Yung in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-pdf-2-otr-10.1177_22104917221082314 - Supplemental material for Risk of surgery and epidemiological profile of athletes presenting to a single sports injury clinic in Hong Kong
Supplemental material, sj-pdf-2-otr-10.1177_22104917221082314 for Risk of surgery and epidemiological profile of athletes presenting to a single sports injury clinic in Hong Kong by Ashley Ying-Ying Wong, Gene Chi-Wai Man, Yuen-Man Wu, Hiu-Wun Wong, Michael Tim-Yun Ong and Patrick Shu-Hang Yung in Journal of Orthopaedics, Trauma and Rehabilitation
Supplemental Material
sj-pdf-3-otr-10.1177_22104917221082314 - Supplemental material for Risk of surgery and epidemiological profile of athletes presenting to a single sports injury clinic in Hong Kong
Supplemental material, sj-pdf-3-otr-10.1177_22104917221082314 for Risk of surgery and epidemiological profile of athletes presenting to a single sports injury clinic in Hong Kong by Ashley Ying-Ying Wong, Gene Chi-Wai Man, Yuen-Man Wu, Hiu-Wun Wong, Michael Tim-Yun Ong and Patrick Shu-Hang Yung in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Acknowledgements
The author would like to thank the patients and staff at the Prince of Wales hospital for their participation in this study. We would also like to thank Mr CHAU Wai Wang for his technical assistance.
Authors’ contributions
AYYW, GCWM, MTYO and PSHY conceived, designed and coordinated the study, and critically reviewed the manuscript. AYYW, YMW, HWW, and MTYP helped with clinical assessments and patients’ follow-up. GCWM and AYYW collected the data, analyzed the data, and drafted the manuscript. MTYO and PSHY supervised the overall study. All authors were involved in writing the paper and had final approval of the submitted and published versions.
Ethics approval and consent to participate
Survey and behaviral research ethical approval was obtained and conducted in accordance to guidelines approved by the institutional clinical research ethics committee (The Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (Joint CUHK-NTEC CREC). All study procedures were conducted in accordance with the guidelines approved by the ethics committee and the Declaration of Helsinki. Written informed consent was obtained for all subjects or from parents/guardians of minors before participating in this study.
Consent for publication
Written informed consent was obtained for all subjects or from parents/guardians of minors before participating in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.