
Abstract
Introduction
Hip replacement surgery is currently the most successful orthopaedic operation worldwide. It was chosen by the WHO to be the “operation of the century” due to the enormous pain relief and successful mobilization it offers. 1 The outcome of this operation is, however, dependent on the quality of postoperative rehabilitation following it and the patient's dedication and performance during it. 2 The aim of multidisciplinary postoperative rehabilitation after total hip replacement is to improve hip function and patient's mobility and enable faster convalescence.
Fast track surgery has been introduced more than 20 years ago by Henrik Kehlet in Denmark as a coordinated multimodal approach to decrease the postoperative patho-physiological stress reaction after colorectal surgery. 3 In the new millennium, many Scandinavian countries started this enhanced recovery after surgery (ERAS) program in the early postoperative period after total hip and knee replacement in order to allow a shorter hospital stay and rapid ambulation of patients.4–11 The achieved socioeconomic gains have encouraged surgeons in Western Europe to establish new pathways including a fast track multidisciplinary rehabilitation with excellent short term outcomes.12–17 Even in England and Ireland there have been reports in this decade showing reduced morbidity and mortality following enhanced recovery hip and knee arthroplasty.18–20 Furthermore, new reports have been published on ambulatory (outpatient) and one-day hip and knee replacement surgery.21–26 In Germany, 261.000 hip replacement surgeries (175.000 elective total hip arthroplasties) were done in 2017 with increasing tendency. 27 Several patients undergoing joint replacement nowadays are young and need to be rapidly and adequately integrated back into work life. Furthermore, with an aging population, health care systems may not be able to afford a long hospital stay postoperatively or offer complex rehabilitation program. Therefore, the implementation of such a fast track pathway in Germany would allow socioeconomic benefits for the patient and cost reduction for the hospital and health care providers. However, a multi-disciplinary approach has yet to be standardized and its evidence-based acceptance has to be increased in order to have the desired widespread application of this fast track rehabilitation program. As the literature is deficient in high-quality studies comparing conventional and fast track hip replacement, this work was initiated.
Materials & methods
In a randomized controlled trial (RCT), 60 patients undergoing total hip replacement (THR) for the treatment of osteoarthritis (OA) of the hip joint were treated either with a conventional 3 to 4 week-rehabilitation program after a normal hospital stay (8–12 days), or with a fast track program that starts at the operative day with early discharge after 3–5 days. The study was done at the orthopaedic department of a university teaching hospital, certified as an arthroplasty center of maximum service. The study was approved by the local ethical committee (KEK_02_2019) and registered in the German clinical trial registry (DRKS00020954). There were 32 Females and 28 males who ranged in age between 47 and 80 years (average age: 68.4 years). A simple randomization method was used (flipping a coin). Exclusion criteria were: age above 80 years, morbid obesity (BMI >40 kg/m2), hemiarthroplasty or bipolar prostheses, femoral neck fractures, posttraumatic arthritis, inflammatory arthritis or patients’ incompliance.
All cases were operated upon under general anesthesia in a standard operation room (OR) with laminar flow by two surgeons. The approach used was the minimally invasive posterior approach in the lateral decubitus position. Surgical incisions were 6–10 cm long. All patients received preoperative single-shot antibiotic prophylaxis (Cefuroxime 1.5 gm) and 1 gm of intravenous Tranexamic acid at induction of anesthesia. All acetabular cups were implanted in a cementless technique. All Inlays were made of highly cross-linked polyethylene (XLPE) with 20° posterolateral elevation to reduce the risk of dislocation. Femoral shafts were either cementless (n = 39) or cemented (n = 21). As regards head size, we used 36 heads starting with an acetabular cup size of 52 mm. Local infiltration analgesia (LIA) was given in all cases except in cases with known allergy to local anesthetics. No surgical drains were used and urinary catheters were avoided. C-Arm Images of the newly implanted hip arthroplasty were done before leaving the OR.
Mobilization started in the fast track group on the day of surgery (day zero) 3–5 h after leaving the OR and being transferred to the normal orthopaedic ward. Patients in the conventional group were mobilized 1–3 days (mean 1.1 days) after surgery according to the general condition and pain tolerance. The postoperative pain therapy was identical in both groups. After successful verticalisation and mobilization, patients in both groups had daily physiotherapy, gait training on crutches, range of motion exercises for the hip joint (between 0 and 90 degrees of flexion) and group exercises as tolerated. Hip adduction and rotation movements were avoided to prevent prosthetic dislocation. Postoperative x-rays were done on the third postoperative day. Patients were regularly assessed by the operating surgeon for their eligibility for discharge. Discharge criteria were: ability to stand and walk safely with or without aids, ability to walk up and down stairs without assistance, ability to perform personal care, hip joint flexion of 90 degrees, knowledge of restrictions, dry wound, satisfactory oral pain control and acceptance of discharge. For all patients but one patient in each group, a multidisciplinary orthopaedic rehabilitation program was started after discharge.
Hip function was evaluated using two different patient reported outcome measures (PROMs): the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and the Harris Hip Score (HHS) preoperatively, 6 weeks and 12 weeks after surgery respectively. The non-parametric Mann-Whitney U test was used to compare both groups. A p-value of <0.05 was considered significant. Complications were documented and the 90-day readmission rate was recorded for both groups (Figure 1).
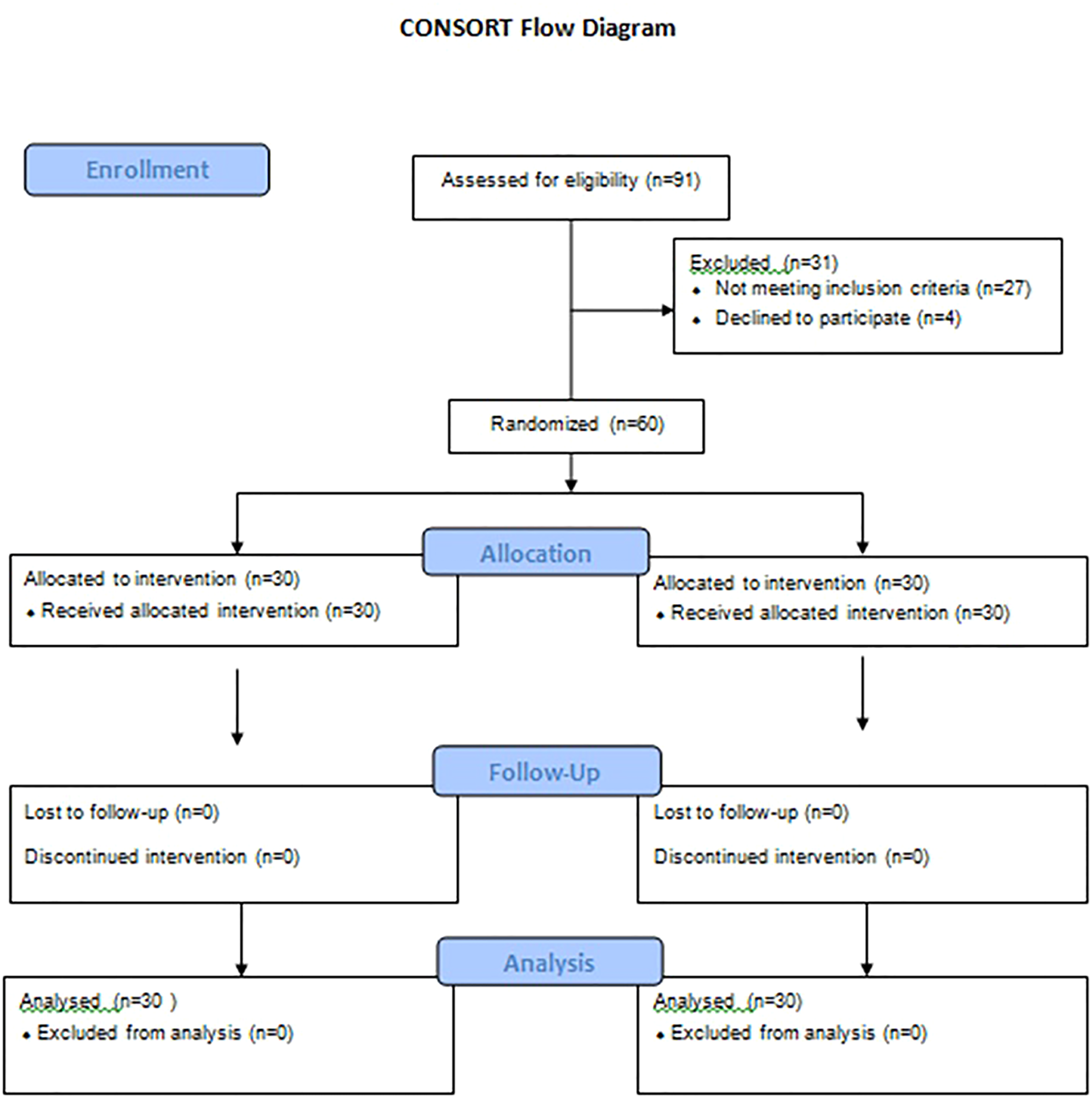
CONSORT Flow Chart
Results
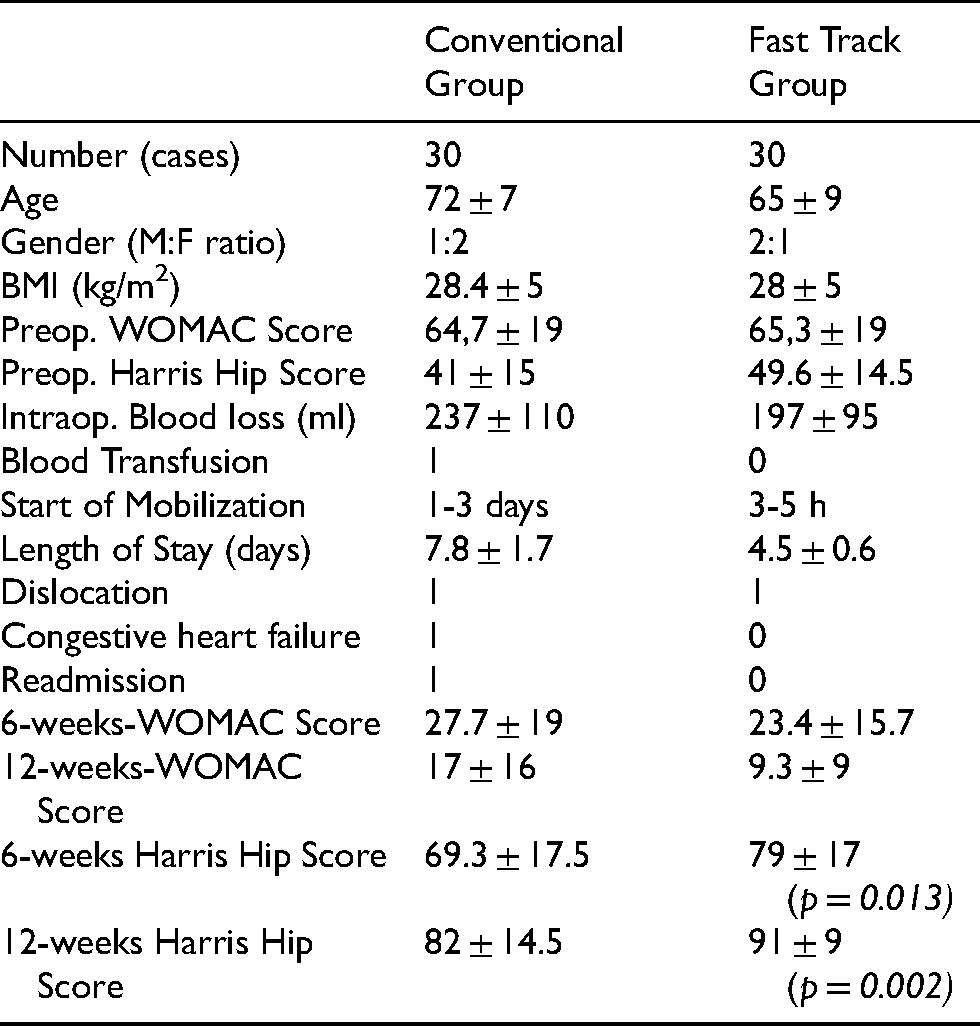
The mean BMI was 28 (range: 19–40) kg/m2 in both groups with 8 patients with a BMI of more than 30 in the conventional group and 7 patients in the fast track group. The indication for surgery was primary hip arthritis in all but 8 cases (5 dysplastic hip arthritis and 3 cases with secondary arthritis due to atraumatic avascular necrosis of the femoral head). The mean preoperative WOMAC Score was 65 (range: 23–99) for all patients in this study with a mean of 64.7 (range: 30–99) in the conventional group and 65.3 (range: 23–93) in the fast track group. The preoperative HSS score for all patients ranged between 10 and 89 (mean: 45.4). It averaged 41 (range: 10–76) in patients of the conventional group and 49.6 (range: 17–89) in patients of the fast track group.
Sixteen patients in the conventional group and five patients in the fast track group had a cemented shaft (hybrid fixation). The rest had cementless femoral and acetabular components. The intraoperative blood loss averaged 237 ml in the conventional group compared to 197 ml in the fast track group. Only one patient in the conventional group needed postoperative blood transfusion (two erythrocyte concentrates) compared to none in the fast track group. The average length of stay (LOS) in the fast track group was 4.5 (range 3–5 days) compared to 7.8 (range: 6–11) days in the conventional group (p = <0.001). Patient's discharge in less than three days was intentionally avoided because of the German DRG (diagnosis related groups) System that dictates financial reductions in such a short LOS.
Complications included one posterior hip dislocation in either group as well as a case of decompensated heart failure in the conventional group. Apart from this, there was one additional readmission in the conventional group due to dyspnea at rest with fear of pulmonary embolism compared to none in the fast track group. No cases of intraoperative fractures or periprosthetic femoral fractures (PPFF) were encountered. Only one patient in the fast track group was not satisfied with the procedure. None of the operated patients had prosthetic joint infection (PJI). Also no patients developed postoperative deep venous thrombosis (DVT) in either group.
The mean WOMAC Score six weeks after THR was 27.7 (range: 3–67) in the conventional group and 23.4 (range: 5–82) in the fast track group (p = 0.49). Twelve weeks postoperatively, the WOMAC score averaged 17 (range: 0–59) in the conventional group and 9.3 (range: 0–40) in the fast track group (p = 0.08).
As regards the HSS, patients in the conventional group had a mean score of 69.3 (range 28–94) in comparison to 79 (range: 19–96) in the fast track group six weeks after surgery. The difference was statistically significant (p = 0.013). After twelve weeks, the mean HHS was 82 (range 41–99) in the conventional group and 91 (range: 64–100) in the fast track group. The difference was again statistically significant (p = 0.002) (Table 1).
Comparative results between both groups.
Discussion
Total hip replacement is the treatment of choice for advanced osteoarthritis of the hip joint. 1 As an integral component in the postoperative management, early and intensive physical therapy has been shown to reduce swelling, increase range of motion, improve hip muscle strength and regain function after total joint arthroplasty.14,28–31 Historically, hospital stay after total hip replacement has been several weeks 21 and mostly consisted of bed rest during hospitalization. 16 The introduction of fast track rehabilitation and its implementation in joint replacement surgery has been shown to reduce perioperative morbidity and mortality and result in shorter reconvalescence.12–18 Such optimized patient treatment through well-described evidence-based clinical pathways with multimodal opioid sparing anesthesia, early mobilization with full weight bearing and modern surgical technique has led to a worldwide decrease in length of stay after joint surgery in the last decade. Furthermore, total hip arthroplasty in an outpatient setting (hip in a day) is currently feasible for selected21–23 or even unselected patients.24–26 This prospective randomized study compared 30 patients undergoing total hip replacement with a conventional postoperative rehabilitation program after a normal hospital stay to 30 cases with fast track rehabilitation program that started 3–5 h after surgery ending in patients discharge after 3–5 days. The complication rate was less in the fast track group as compared to the conventional group. There were no readmissions within three months after surgery in the fast track group apart from a single case of prosthetic dislocation due to a fall in the rehabilitation clinic. This compares favorably to other studies that demonstrated no increase in procedure-specific complications, readmissions or reoperations up to 3 months after primary THR.4–6,21,24 Only a report from Finland demonstrated an increase in the 42-day readmission rate (from 3.1% to 8.3%) after the implementation of fast track surgery despite reducing the mean length of hospital stay (LOS) from 5 to 2 days. 17 These good results have been confirmed by a recent metaanalysis by Zhu et al. that showed a significant reduction in the LOS and the complication rate after total hip and knee replacement using fast track rehabilitation without impact on the 30-day readmission rates. 32
Fast track surgery in patients with special needs or high comorbidity is still debatable. 33 Jørgensen et al. identified age ≥ 80 years, anticoagulant therapy, pulmonary disease, pharmacologically treated psychiatric disorder, anemia and walking aids as at high risk of preventable medical complications following fast track joint arthroplasty. 34 Husted et al. identified a higher BMI (very obese and morbidly obese patients) as associated with a longer hospital stay over 4 days after total hip replacement with no difference found in patients with total knee replacement. 35 That is why we excluded patients over 80 years and morbidly obese patients (BMI above 40 kg/m2) from our study.
In both study groups, there were no cases of postoperative DVT or pulmonary embolism encountered in our patients. The risk of thromboembolic complications after fast-track joint arthroplasty with early mobilization, short hospitalization and even a short duration of DVT prophylaxis (until discharge) has been shown by Husted et al. to compare favorably with published regimens with extended prophylaxis (up to 36 days) and hospitalization up to 11 days. 36
The study is limited by its low number of cases. Nevertheless, patients in the fast track group demonstrated a superior functional outcome with consistently better PROMs 6 weeks and 3 months after surgery compared to the conventional approach. This stands in agreement with the results demonstrated by Specht et al. 15 and Klapwijk et al. 16 and confirms that fast track rehabilitation aims primarily at enhancing patient's recovery and early convalescence rather than early discharge (first better then faster 26 ). The associated social, psychological and occupational gains for the patient are undisputable. Furthermore, the economic impact of this multidisciplinary standardized pathway through decreasing costs without compromising results is inevitable. In our hospital, each day of in-patient treatment after THA costs 300 euros on the average. Reducing the LOS by 3.3 days in our study comprises a cost reduction by 1000 euros per patient (30.000 euros in the whole group). Reilly et al. also described a cost saving of 27% and significantly reduced hospital bed occupancy after fast track unicompartmental knee replacement. 37 Similarly, Andereasen et al. demonstrated a low cost of around US $ 2500 for a 2-day stay after THA. 38 Such an early discharge (< 3 days) is however still being sanctioned in Germany. These and other peculiarities of the German health system have been shown by Nöth and colleagues to be a possible obstacle against the widespread use of fast track hip replacement surgery in Germany. 39 However, the overall resonance for this approach in Germany is very encouraging.39,40 The, implementation of such an approach in Germany with approximately 450.000 joint replacement surgeries in a year would be much more a revolutionary step as compared to Denmark, the mother country of fast track surgery, where just 12.000 hip and knee replacements are being performed per year. 5
In conclusion, fast track rehabilitation after total hip replacement is associated with early patient's mobilization and rapid functional recovery with better outcome and less risk of complications or readmissions. This approach needs careful implementation and dedicated patients and staff to maintain a satisfactory care throughout the treatment process.
Footnotes
Data availability statement
Data presented in part in the 20th German Arthroplasty Association (AE) Congress, December 2018, Düsseldorf – Germany and in the 40th SICOT Orthopaedic World Congress (OWC), December 2019, Muscat – Oman
Declaration of conflicting interests
The authors have no conflicts of interest to disclose. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The authors certify that their institution has approved or waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.