
Abstract

Introduction
The success of a total knee arthroplasty (TKA) is closely related to the correct position of the prosthetic components. Malalignment in the coronal and sagittal planes are the most important cause of mechanical imbalance and patellofemoral (PF) complications. It is also a cause of early failure due to polyethylene wear and stability problems. Neutral posterior tibial slope (PTS) contributes to stability in the sagittal plane. The change in tibial inclination plays a significant role in knee kinematics.1–3 Previous cadaveric and biomechanical studies have shown that kinematics and force distribution are altered by inclination changes. In a study by Kang et al., finite element knee prosthesis models showed that the maximum contact load at the PF joint, quadriceps force, and collateral ligament forces decrease when the PTS is increased. 4 In the mobile-bearing TKA, the rotation of the polyethylene liner and anterior translation provide better compliance with changes in tibial inclination than in the fixed-bearing TKA.5–7 Biomechanical studies show the changes caused by the angle change on knee kinematics. However, the impact of PTS changes on the outcomes of mobile-bearing TKA and patient satisfaction is not yet clear. The aim of this study was to investigate the effects of PTS changes on knee range of motion, knee scores, and overall satisfaction in patients who underwent mobile-bearing posterior cruciate ligament retaining (CR) TKA.
Material and methods
The study design was a retrospective analysis of prospectively collected data from the hospital database TKA registry. Patients who were followed up and treated at our hospital between January 2016 and January 2020 were included in the study. The authors’ institution ethics committee approved this study, and informed consent was obtained from all patients. This study was conducted in accordance with the Declaration of Helsinki. Sixty-three knees of sixty-two patients (including one patient bilaterally) who underwent primary mobile-bearing TKA were examined in this study. Fifty-six out of 118 cases with tibial slope outside our study range were excluded. All patients used a mobile-bearing, cruciate-retaining cemented modular prosthesis (The Lima MULTIGEN Plus CR, Italy). The study included patients treated for end-stage primary osteoarthritis with TKA and who had at least one year of follow-up. Patients who had undergone revision surgery, secondary knee osteoarthritis (patients with valgus deformities, previous resection or incision, fracture sequelae and associated with neurological disorders), complications during follow-up (periprosthetic fracture, infection) and patients who could not be followed up were excluded from the study.
Surgery was performed with a standard midline incision and a medial parapatellar arthrotomy. After soft tissue release, a distal femoral resection with an intramedullary guide was performed, followed by a proximal tibial resection at 90 degrees to the longitudinal axis of the tibia in the coronal plane. The femoral component was oriented perpendicular to the mechanical axis of the femur and parallel to the clinical epicondylar axis in the transverse plane. The tibial cutting was made using the extramedullary guide with spike. The extramedullary guide rotation was adjusted by aligning it over the medial third of the tibial tuberosity and over the second toe. The proximal tibial cutting was performed by surgeons’ preference using adjustable cutting blocks referenced to the anterior tibial cortex in the sagittal plane, which corresponds to approximately 7–10°, neutral (0–6°) or preoperative slope angle degrees. A spacer block can be inserted into the extension gap to assess adequate extension gap symmetry. After resection of the extension gap and removal of the osteophyte, gap symmetry, soft tissue balance, and alignment of the lower extremity with respect to the mechanical axis are assessed by inserting a spacer block into the extension gap. After accurate balance in extension, attention is directed to the flexion gap. Implant-specific laminar spacers can be used to evenly tension the collateral ligaments when the knee is in 90 degrees of flexion. Once a symmetrical flexion and extension gap is achieved, a spacer block is inserted into the extension gap to verify symmetry of the extension gap and equality with the flexion gap. After implantation of the femoral and tibial components with polymethyl methacrylate (PMMA) cement, the patellar osteophytes were excised.
No implantation was performed on the patella. All surgeries were performed by the same surgical team. At least one year postoperatively, patients were monitored clinically and radiologically. In all patients, Knee Injury and Osteoarthritis Outcome Score (KOOS), Kujala Anterior Knee Pain Scale (K-AKPS), and knee joint range of motion parameters (ROM) were evaluated at the last follow-up. Measurements were based on radiographic evaluations at the last follow-up visit. Caton-Deschamps Patellar height ratio, Blackburne-Peel ratio, mechanical axis angle, and posterior tibial component inclination angle were measured by lateral knee radiography and orthoroentgenography. (Figure 1.) Patients were divided into two groups with respect to the angle of the posterior tibial component. Those with an PTS angle of less than 5 degrees were assigned Group I, and those with an PTS angle of more than 10 degrees were assigned Group II. Patients with in-between slope values were not evaluated. In addition, SF −36 and Oxford Knee scores (OKS) were included in the study to specifically evaluate overall patient satisfaction and patient outcome after arthroplasty.

The posterior inclination angle of the tibial plateau determined on lateral radiographs. The intramedullary alignment line (thin line) was drawn from midpoint of the medullary canal. A line tangential to the tibial plateau (thick line) was second drawn. A dotted line perpendicular to the thin line was drawn and the angle value between the dotted line was measured.
Radiological assessment of tibial slope
Tibial slope measurements were taken from the full lateral radiographs obtained during the postoperative follow-up period. In the lateral radiographs, the tangential line connecting the anterior and posterior highest points of the tibial component was determined to be the line for tibial slope. The tibial proximal anatomic axis (TPAA) line was determined as the connection of the midpoints of the tibial diaphyseal segment between the point 15 cm distal to the highest point of the knee joint and the point 5 cm distal to the most protruding tibial tuberosity. Values for tibial slope were determined by subtracting the angle between the tangential line and the vertical line (TPAA) from 90 degrees. Slope angle was measured using the software PACS angle measurement tools used by our institution with Picture Archiving and Communication System (PACS). 8 PTS measurements were taken by two different surgeons at different times five days apart and recorded as two separate measurements. Interobserver and intraobserver reliabilities were estimated using intraclass correlation coefficients (ICCs) for the two observers. (Tables 1 and 2)
Independent interobserver reliability evaluation of tibial slope measurement.

*ICC: Intra-Class Correlation Coefficient CI: Confidence Interval **p ≤ 0.01.
Independent intraobserver reliability evaluation of tibial slope measurement.

*ICC: Intra-Class Correlation Coefficient CI: Confidence Interval **p ≤ 0.01.
Statistical analysis
The SPSS software (Statistical Package for Social Sciences) version 21.0 was used for statistical analysis. The Shapiro-Wilk test was used to determine if the variables were normally distributed. Data are presented as mean ± standard deviation for continuous variables and frequency (percentage) for categorical variables. Normally distributed variables were analyzed using the t-test for independent samples. Results were analyzed with a 95% confidence interval and significance at the p <0.05 level. Relationships between groups were examined using linear regression analysis. Post-hoc power analysis was used to estimate the minimum sample size needed to observe a significant difference between groups. This level of power would be achieved if the study groups included at least 17 patients. The effect size is between medium and large values and the type two error values are within the appropriate limits. The interobserver and intraobserver reliability was estimated using ICCs for the 2 observers.
Results
A total of 64 knee findings from 10 male and 53 female patients were included in the study. The mean age was 68 ± 9.2 years and the follow-up time was 20.5 ± 4.1 months. There was no statistical difference between the groups in terms of age, body mass index, demographic patterns and follow-up duration (p < 0.05). (Table 3)
Demographic characteristics of the patients analyzed according to the groups.
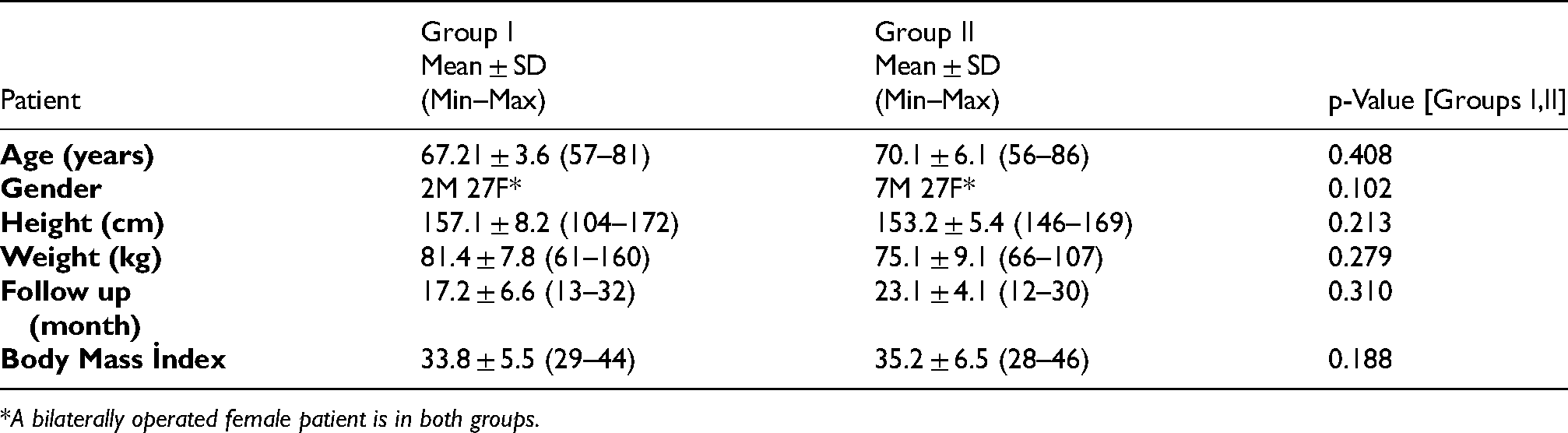
*A bilaterally operated female patient is in both groups.
In patients with a PTS angle of less than 5 degrees [Group I], a mean mechanical axis angle of 4.11 ± 4.1, a Caton-Deschamps index of 1.09 ± 0.7, and a Blackburne-Peel ratio of 1.17 ± 0.6 were measured. In patients with a PTS angle greater than 10 degrees [group II], a mean mechanical axis angle of 4.37 ± 3.30, a Caton-Deschamps -index of 1.16 ± 0.42, and a Blackburne-Peel -ratio of 0.6 ± 0.2 were measured. According to the results of radiological evaluation, there was no statistical difference between the groups in terms of Caton-Deschamps patella height ratio and mechanical axis. However, there was a significant difference between the groups in terms of Blackburne-Peel ratio results (p < 0.05). (Table 4)
Distribution of data according to groups.

The KOOS mean values in group I were 21.36 ± 3.4 and knee ROM was 102.65 ± 6 degrees, in group II KOOS was 32.22 ± 2.5 and knee ROM was 105.5 ± 6.5 degrees. Based on the results of clinical evaluation, there was no significant statistical difference between the KOOS and knee ROM of the patients according to the groups. In the analysis, no significant relationship was found between the tibial inclination and ROM within both groups. (Figure 2.) However, there was a significant difference between the results of Kujala PF knee score between the groups (p <0.05). The K-AKPS was 53.15 ± 5.5 in group I patients and 75.1 ± 5.5 in group II.

Distribution between the posterior tibial slope angle (y dependent) versus joint range of motion (x independent) in both groups was not correlated in the regression analysis curve.
The changes in SF-36 and Oxford knee score before and after surgery in both groups were statistically significant (p < 0.05). However, there was no significant statistical difference between the distribution of patients’ general health and satisfaction scores [SF 36 and Oxford Knee Score] by group. For group I patients, the mean values of SF-36 scores were 63 ± 2 and OKS were 36.69 ± 3.5. For group II patients, the mean values of OKS and SF-36 were 37.4 ± 2.5 and 64 ± 3.5, respectively.
Discussion
Modular polyethylene designs in mobile bearing total knee prostheses provide a greater range of motion and reduced contact stress on the polyethylene surfaces.9–11 This provides greater compliance in the triaxial planes of motion during normal knee gait cycles. The effects of changing the PTS angle on joint range of motion in fixed total knee prostheses have been investigated in several studies.1,3,5 A cadaver study by Chambers et al. found that a gradual increase in tibial inclination up to 10 degrees produced a gradual increase in degrees of flexion up to 10.6 degrees. 12 Other biomechanical studies also showed that increasing tibial inclination increased joint range of motion.13,14 From a biomechanical aspect, the mobile-bearing design has differences that affect postoperative range of motion compared with the fixed-bearing TKA. The effect of kinematic features such as posterior femoral translation and axial rotation in mobile-bearing knee prostheses makes a difference in PTS changes. There are few studies showing the effect of changing PTS on ROM in mobile bearing total knee prostheses. Kastner et al. investigated the effect of PTS on ROM after low contact motion bearing TKA and found that there was no relationship between tibial inclination and ROM. 6 In our study based on the clinical data of the patients, no statistical difference was found between the groups with respect to ROM.
The change in PTS angle alters the femur-tibia contact point in the sagittal plane and affects the biomechanics of the patella and quadriceps. 14 The change in the joint line after knee arthroplasty causes a change in the height of the patella in the resting position, and the mechanical axis changes in the coronal plane also cause changes in the patella-Q angle. Depending on the change in patellar height, there may be signs of patellar malalignment, subluxation, patellar chondromalacia, and anterior knee pain. In knee arthroplasty, patella alta or baja findings are clinically encountered due to the change in joint line. Caton-Deschamps Index or Blackburne Peel index measurements and evaluation of mechanical axis angles exclude factors that may be influential in anterior knee pain. When we examined the effect of this change on the position of the patella, it was found that there was no difference between two groups. Two different methods of measurement were used to assess the position of the patella. While there was no statistical difference in the Caton-Deschamps patella height measurement, it was observed that there was a difference between groups when measured using the Blackburne-Peel method. We realized that this difference with the Blackburne-Peel method is due to the fact that the measurement method is affected by the tibial inclination. 15 (Figure 3.) The Blackburne-Peel method measures the ratio of the joint surface length of the patella to the height of the inferior pole of the joint surface above the tibial plateau line. Classen et al. suggested that the modified Blackburne-Peel method is more accurate because it eliminates measurement error in polyethylene insert height, tibial component inclination, and patellar joint line overlap. 16 The lack of a significant difference in Caton-Deschamps patella height ratio between groups suggests that anterior knee pain is not related to the change in patella height.

A) Caton-Deschamps patella height ratio: y/x measurement values do not change with PTS angle change. b) Blackburne-Peel ratio: y/x values are measured as y*/x depending on the PTS angle change.
When evaluated in the coronal plane, it was found that there was no difference in the angle of alignment of the mechanical axis between the groups and the values in both groups were close to the normal mechanical axis (0 ± 4°). The change in coronal alignment affects the quadriceps angle (Q angle), the biomechanics of the PF joint, and the contact pressure of the patella surface, resulting in changes in knee scores. The design of the mobile insert has biomechanical properties close to those of the normal knee joint. Both anterior-posterior translation and internal-external rotation occur at the interface of the insert with the tibial shell.
The larger contact area and load distribution in these designs result in better compensation for mechanical axis changes.17,18 In the clinical evaluation we performed using two different knee scores (KOOS and OKS), it was found that the knee scores made no significant difference between the groups. SF−36 scoring reviewed for general health and patient satisfaction scores showed that the difference in tibial inclination made no significant difference. Only the Kujala PF knee score showed a significant difference between groups. An overall low score distribution was observed for issues such as excessive squatting, long bent knees, hamstring atrophy, inability to bend the knees, and swelling in the Kujala knee score.
In this study, an angle of 5 degrees or less was accepted as a low tibial angle. There may be differences in normal posterior tibial tilt and lateral and medial tibial plateau tilt depending on race and gender. The mean medial and lateral tibial inclination in female patients was 10.7° ± 3.8° and 8.8° ± 3.8°, while the mean medial and lateral tibial inclination in male patients was 8.9° ± 4.8° and 7.9° ± 4.7°, respectively, as noted by Yong-Gon Koh et al. 19 In another study, Jade Pei Yuik Ho et al. showed that in Asian knees, the average PTS is 11°, with a reference range of 5°-17° (mean ± 2 standard deviation). 20 In the study by K.Y Chiu et al. it was found that the average posterior tilt of the medial plateau was 14.8 ° and the posterior tilt of the lateral plateau was 11.8 °. 21 Those outside the range of 5–10 degrees were included in the study by considering the average reference values of the PTS angle. For tibial implants, a tibial slope of 5 and 10 degrees has been accepted as lower and upper limits in literature. Ken Okazaki et al. accepted the inclination angle of 5 degrees as a reference value. Wittenberg et al. stated that 0–10 degrees can be considered normal. In our study, a radiological difference of 5 degrees would contribute to potential clinical difference. Keong-Hwan Kim et al. found that a difference of 4 degrees was significant in his study. Wittenberg et al. also used measurements with a difference of 5 degrees in their studies.22–26
The positive aspect of this study is the possibility of subjective measurements regarding reflections on overall performance and patient activities. In vitro and finite element studies provide limited insight into loading conditions or angle changes with respect to the overall biomechanical status of patients. To our knowledge, this is the first study to demonstrate a relationship between PTS angle and knee scores in mobile-bearing CR -TKA. The effects of slope angles below 5 degrees and above 10 degrees on clinical measurements and questionnaire scores were investigated. The limitations of our study are that there are differences in the practice, skills and preferences of surgeons. In addition, the lack of PTS comparison in posterior cruciate ligament sacrificing mobile-bearing TKA led to the inability to obtain more comprehensive results.
Conclusions
PTS angle changes in mobile bearing CR -TKA do not affect ROM, general health status, and patient satisfaction. The Kujala anterior knee pain score was significantly different, but made no difference in overall patient satisfaction scores.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Study conception and design: Adıyeke, Erdogan.
Acquisition of data: Gunduz, Kafadar.
Analysis and interpretation of data: Adıyeke.
Critical revision: Adıyeke, Erdogan.