
Abstract
Background:
Venous thromboembolism (VTE) is a clinically relevant complication of major orthopedic surgeries. The prevalence of VTE and the indications for VTE thromboprophylaxis in Asian patients undergoing arthroscopic anterior cruciate ligament (ACL) reconstruction are not clear. This study aims to evaluate the prevalence of clinically significant venous thromboembolic events (VTE) in Asian patients undergoing arthroscopic ACL reconstruction without mechanical or chemical thromboprophylaxis.
Methods:
All patients who underwent ACL reconstruction by a single surgeon from 2006 to 2018 in a single tertiary institution were reviewed. The inclusion criteria for the study included Asian patients of common ethnic groups in Singapore (Chinese, Malay, Indian) and underwent primary or revision ACL reconstruction, or ACL reconstruction combined with meniscal surgery. The exclusion criteria were patients with incomplete medical records, pre-existing anticoagulant treatment within 1 year prior to the surgery and additional procedures that altered the standard rehabilitation protocol, less than 6 months of follow-up duration. All patients received general anesthesia. The single-bundle ACL technique with autologous hamstring tendon reconstruction was performed. No chemical DVT prophylaxis was given. The patients were screened for clinically for VTE. Symptomatic patients were referred for ultrasonography.
Results:
Of the 581 patients reviewed, 3 patients had a clinical suspicion of deep vein thrombosis, but subsequent ultrasonography showed no thrombosis. Hence, the prevalence of clinically significant VTE was 0%.
Conclusion:
Given the low prevalence of clinically significant VTE, there is no need for routine mechanical or chemical thromboprophylaxis or radiologic screening in Asian patients undergoing arthroscopic ACL reconstruction.
Keywords
Introduction
The advent of arthroscopic surgery has led to smaller skin incisions, less postoperative pain, and faster postoperative rehabilitation. However, venous thromboembolism (VTE) and its sequelae following arthroscopic surgery remain a concern. VTE is a common and clinically relevant complication of major orthopedic surgery and could potentially lead to mortality. 1 Arthroscopic anterior cruciate ligament (ACL) reconstruction is more invasive and takes longer time than routine arthroscopic surgeries, and therefore might potentially be more predisposed to VTE. There is limited and conflicting data on the prevalence and effective management of VTE. In the Western population, the prevalence reported in literature ranged from 1.5% to 17.9%. 2 –11
Furthermore, there have been studies to show that the prevalence of VTE is relatively lower in Asians as compared to the Westen population in lower limb surgery. 2,3,12 –15 However, with the adoption of Western dietary and lifestyle patterns in recent years, this understanding is debatable. Do Asians truly have a lower prevalence of VTE following ACL reconstruction, and is there a need for routine prophylaxis in the Asian population?
With such varied reported prevalence of VTE and ambiguity regarding prophylactic protocols, we conducted a retrospective review of patients who underwent ACL reconstruction without routine thromboprophylaxis to find out prevalence of VTE.
Material and methods
Data of patients from a single tertiary hospital who underwent ACL reconstruction performed by a single surgeon between February 2006 to December 2017 were collected from hospital medical records and databases. A single surgeon was selected for consistency of surgical technique and postoperative care. The study was approved by the institutional review board.
The inclusion criteria for the study included Asian patients of common ethnic groups in Singapore (Chinese, Malay, Indian) and underwent primary or revision ACL reconstruction, or ACL reconstruction combined with meniscal surgery. The exclusion criteria were patients with incomplete medical records, pre-existing anticoagulant treatment within 1 year prior to the surgery and additional procedures that altered the standard rehabilitation protocol, less than 6 months of follow-up duration.
All patients received general anesthesia. After a knee examination was performed under general anesthesia, a thigh tourniquet was used on the operated limb throughout the of the surgery. Surgical incisions were made immediately after tourniquet inflation. The single-bundle ACL technique with autologous hamstring tendon reconstruction was performed. In revision cases where the hamstring tendons on the ipsilateral limb were not available, hamstring tendons from the contralateral limb were harvested. No routine chemical or mechanical thromboprophylaxis was used.
A standard postoperative rehabilitation protocol was used for all patients. Patients were either discharged on the same day or had an overnight stay in the hospital. A hinged knee brace was used for 6 weeks that allowed the motion of 0 to 90 degrees for 2 weeks and followed by progression to a full range of motion. The full-weight bearing was allowed unless meniscal repair was done. Strengthening exercises were commenced at 6 weeks and return to competitive sports at 6 months. Patients were reviewed in the outpatient clinic postoperatively at 2 weeks, 6 weeks, 3 months, 6 months, 9 months, 12 and 24 months. Patients were asked and examined for symptoms and signs of deep vein thrombosis (DVT) such as calf swelling, erythema, tenderness, fever and symptoms of pulmonary embolism such as shortness of breath and tachycardia.
Results
There were a total number of 657 patients who underwent ACL reconstruction between 2006 and 2017, and 581 patients were included in this study based on the inclusion and exclusion criterion (Table 1). The mean age (±standard deviation) of patients was 29.7 ± 9.4 years (range 16 to 52 years), and mean BMI is 25.9 ± 4.1. The racial distribution of the patients closely resembles that of the Singaporean population: Chinese 75%, Malay 16%, Indian 9%. There were 476 male patients (82%). Only one patient is known to have a previous history of VTE.
Demographic data and clinical details for patients in this study.
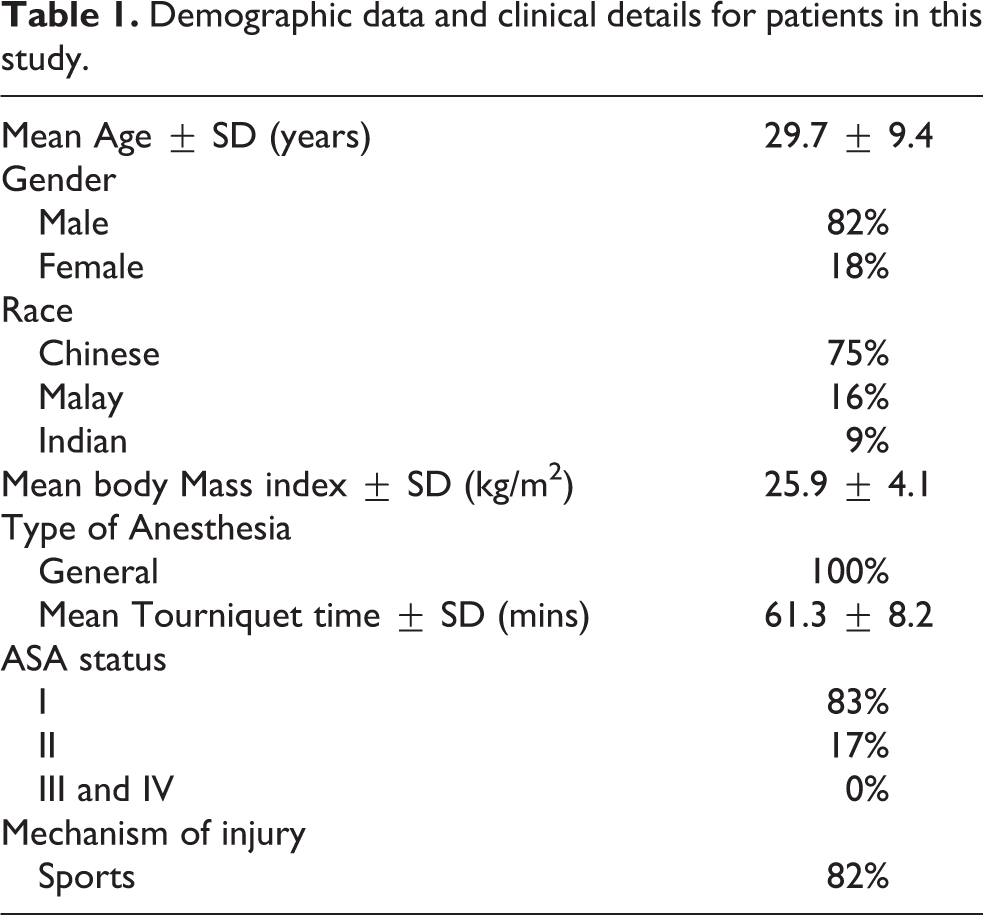
The mean tourniquet time was 61.3 ± 8.2 mins. Thirty-two percent of the patients were discharged on the same day of surgery, while the rest of the patients had an average hospital stay of 1.4 days. The average follow-up duration was 21 months. The follow-up percentage at 6 weeks is 99%, and the follow-up percentage at 24 months is 83%.
None required re-admission due to VTE related symptoms. Three patients had a high clinical suspicion of VTE and were referred for ultrasonographic assessment, which, however, did not show thrombosis.
One patient was readmitted for septic arthritis and underwent revision surgery. No death was detected during the follow-up.
Discussion
The prevalence of VTE after ACL reconstruction without thromboprophylaxis varies from 1.5%–17.9%. 2,3,5,6,8,10,11,15 –17 Hetsroni et al. 18 analyzed 418,323 arthroscopic knee procedures and found an incidence of 0.03% for symptomatic PE without available data on thromboprophylaxis. Janssen et al. 1 found an incidence of fatal PE of 0.2% in a consecutive series of 625 arthroscopic ACL reconstructions. The variable incidence of VTE after ACL reconstruction depends on the diagnostic methods of DVT (clinical parameters, venography, ultrasound or magnetic resonance venography) and the heterogeneity of patient demographics (age, risk factors, surgical time, concomitant surgery, tourniquet time and postoperative mobilization). Our study revealed no prevalence of VTE in patients who underwent ACL reconstruction without prophylaxis. We only performed a radiological evaluation for symptomatic patients who may benefit from the medical intervention in view of the potential complications associated with DVT, such as poorer postsurgical rehabilitation and surgical outcome. 19,20 This would likely account for our prevalence being relatively lower than previous studies. 16,21,22 Furthermore, a relatively younger patient population, low BMI and the exclusion criteria could have led to our study group being a low-risk population.
Kim et al. 23 suggested that genetic factors and dietary patterns could contribute to a low incidence of DVT and PE in Asian patients. Some data support genetic differences as a partial cause of a lower risk of VTE in Asians. Of the known genetic traits, the most prevalent is activated protein C, a mutation known as factor V Leiden 24,25 that increases VTE risk about 7 times in heterozygotes and about 80 times in homozygotes. It is found in approximately 5% of Westerners but is rare in Asian. 26,27 We could not confirm the prevalence of factor V Leiden in the study population but believe that it may be an important reason for the low prevalence of VTE in Asians.
Thromboprophylaxis after ACL reconstruction remains controversial. 8,9,14,19,28 –30 There is no accepted norm regarding thromboprophylaxis in patients undergoing arthroscopic ACL reconstruction. Geerts et al. 9 reviewed the evidence-based literature for thromboprophylaxis in knee arthroscopy. They recommended prophylaxis with low molecular weight heparin only in patients with risk factors for VTE (Grade 2B level of evidence). Risk factors in their study were a history of DVT, age ≥ 40 years, surgical time > 60 minutes and a complicated/prolonged procedure. 9 However, this was not specific for ACL reconstruction. Additional risk factors for VTE after ACL reconstruction in other studies on VTE were smoking, oral contraceptive use, hormone replacement, BMI > 30 kg/m2, chronic venous insufficiency, cancer and thrombophilic conditions. 3,9,11,18,21,30,31 A Cochrane systematic review on interventions for preventing VTE in adults undergoing knee arthroscopy reported that no strong evidence was found to conclude that thromboprophylaxis is effective in preventing VTE in people with unknown risk factors for thrombosis. 19 Routine anticoagulation is not without its risks. Aside from cost considerations, thromboprophylaxis carries with its potential risks, including bleeding, wound complications and systemic complications. 13,32 Although mechanical prophylaxis is a safe method, it adds additional cost to the procedure and may require a prolonged hospital stay to utilize the device. A detailed evaluation of the possible low-risk factors for VTE was not possible in this study due to the nature of the study as well as the low prevalence rate. However, we believe that relatively shorter operation times, shorter tourniquet times, low BMI could have been factors that led to low prevalence, apart from genetic factors.
A routine postoperative radiologic evaluation was not performed for the patients in this study but only on symptomatic patients with clinically significant DVT. Due to the extremely low prevalence of DVT, the use of radiological screening does not appear to be cost-effective. It is the reason only three patients were referred for radiological evaluation. The true prevalence of DVT could be under-reported as asymptomatic patients may be missed out. However, as such patients, including those with distal DVT with thrombi in the calf, regardless of size, do not usually require anticoagulation, 33,34 we do not see the need for routine radiologic evaluation. This study did not identify any cases of symptomatic DVT or VTE post-surgery, and as such, the authors feel that based on risk-benefit analysis, the routine use of thromboprophylaxis and radiographic screening for DVT in ACL reconstruction should not be recommended.
The strength of our study is a large number of a homogenous (eastern Asian) group of patients and a high follow-up rate of patients. The study is, however, limited by its retrospective nature. Furthermore, identification of risk factors was not possible because of the rare prevalence of VTE.
Conclusion
Venous thromboembolism is rare in Asian patients undergoing ACL reconstruction. We do not recommend routine use of thromboprophylaxis and radiological screening for VTE in our local population patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.