
Abstract
Jamu is commonly used to treat a variety of health conditions in South East Asia due to its efficacy, affordability and ease of access. Despite its effectiveness, little is known regarding its contents and adverse effects. Recent studies have found evidence of steroids within jamu preparations. Chronic jamu consumption may inadvertently manifest with adverse effects associated with long-term steroid intake. We describe a case of neck of femur fracture due to secondary osteoporosis with underlying hip osteonecrosis resulting from chronic jamu consumption hoping to increase awareness regarding the devastating effects of these preparations.
Introduction
Osteonecrosis is defined as bone death caused by insufficient blood supply. Due to its tenuous circulation, the hip is vulnerable to this condition. Vascular disruption secondary to chronic steroid therapy is a well-known cause of osteonecrosis. Unbeknown to many; certain jamu (a generic term used to describe traditional medication formulations in South East Asia) preparations contain steroids. These preparations are a popular form of analgesic due to their ease of access, relative affordability and effectiveness. Unfortunately, the side effects of these preparations are vague and rarely reported. A case of neck of femur fracture due to secondary osteoporosis with underlying hip osteonecrosis resulting from chronic jamu consumption is described, hoping to increase awareness regarding the condition.
Case report
A 34-year-old gentleman presented complaining of right hip pain for 2 weeks. He developed sudden severe sharp pain in his right hip after attempting to lift a 5-liter petrol tank off the floor. The pain gradually worsened, necessitating the need for a walking frame to assist his ambulation. To control his pain and aid his mobility, he resorted to off-the-counter analgesics but noticed with time, amelioration of pain upon weight bearing was no longer possible.
Prior to this incident, he was community ambulant but had gout, which was managed with Allopurinol. Further questioning revealed that he had been consuming bi-weekly doses (two capsules per intake) of a traditional medication preparation (Montalin, PJ Air Madu, Magelang, a steroid containing traditional medication preparation) (Figure 1) that was purchased illegally over 5 months, believing it would help in management of his gout symptoms. He refuted history of steroid intake and denied history of constitutional symptoms such as loss of weight or appetite prior to this. An extensive review to rule out other possible causes of hip osteonecrosis and possible causes of a pathological fracture was done and found unremarkable. There were no constitutional symptoms, congenital hip problems, trauma or infections involving his right hip before this.
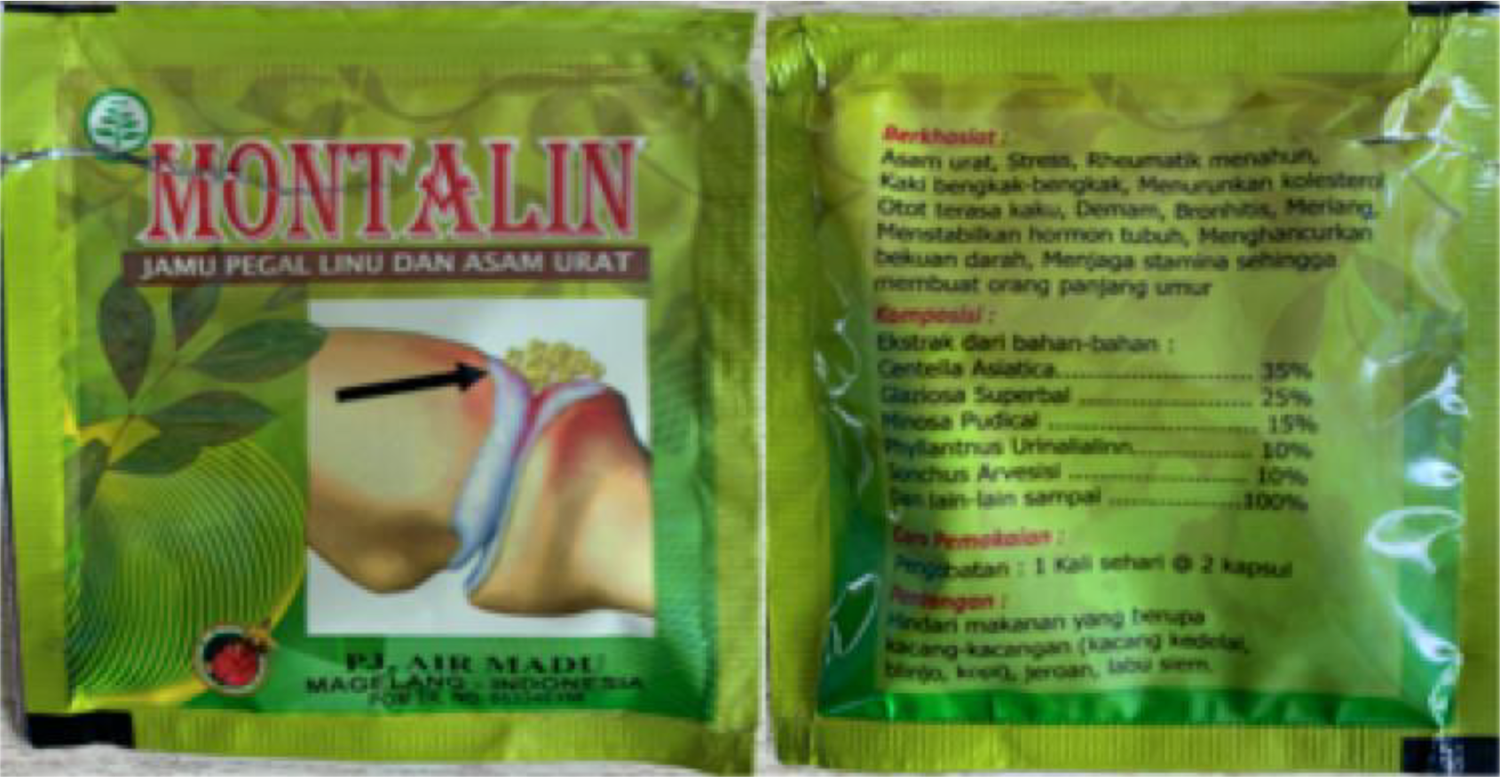
“Montalin” packaging containing 500 mg capsules.
Clinically, he was wheelchair bound due to his right hip pain. His vital parameters, cardio-respiratory and abdominal exam were normal. Examination of the right hip revealed limitation in range of motion compared to the left hip.
An Endocrinology team review was sought. He was investigated for endogenous glucocorticoid excess with 24-hour urine free cortisol levels, low-dose dexamethasone suppression test and ultrasound of the kidneys and adrenal glands, all of which returned with normal results. To assess exogenous steroid intake, a pharmaceutical review of the jamu (Montalin, PJ Air Madu, Magelang) preparation consumed by the patient was undertaken, revealing that it was a banned preparation with undocumented steroid content. Further review of the preparation revealed the presence of ingredients such as Centenella Asiatica, Glasioza Superbal, Minosa Pudical, Phyllantus Urinalialinn and Sonchus Arvesisi. Laboratory investigations to rule out infections, autoimmune disorders and malignancy were also performed with unremarkable results. Serum vitamin-D levels and corrected serum calcium were within normal limits. His uric acid levels corresponded with his history of gout.
Radiographs of the patient’s pelvis and right hip revealed generalized osteopenia within the region of the proximal femur bilaterally. A right-sided sub-capital neck of femur fracture was seen in addition to sclerotic changes and loss of sphericity of the right femoral head (Figure 2). A CT scan of his right hip further substantiated the findings (Figure 3). MRI scans were not indicated in view of the radiographic findings indicative of ongoing femoral head osteonecrosis.

Pelvic radiograph revealing generalized osteopenia within the region of the proximal femur bilaterally. A sub-capital neck of femur fracture is seen at the right hip with loss of sphericity of the right femoral head (Ficat Stage IV).
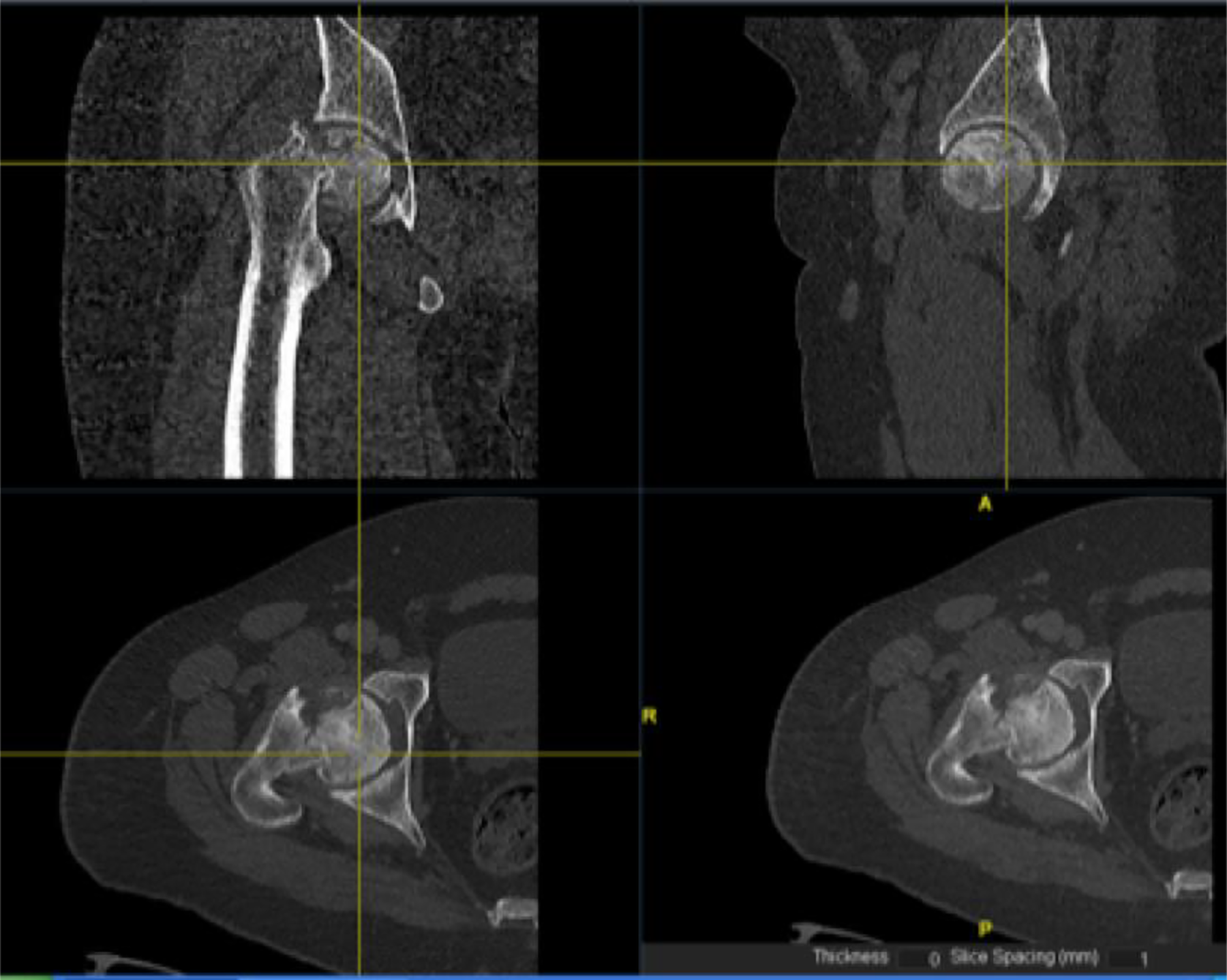
Right pelvic CT images delineating a sub-capital neck of femur fracture with a partially deformed femoral head and degenerative changes of the hip.
He was diagnosed with a pathological sub-capital right neck of femur fracture with secondary osteoporosis with underlying osteonecrosis of the right hip secondary to chronic exogenous steroid consumption (chronic jamu consumption). He was advised to stop jamu consumption and management with a multidisciplinary approach was initiated. He was advised for total hip replacement of the right hip by the Arthroplasty team but was not keen for surgical intervention. He currently ambulates relatively well with a walking frame and is still under regular follow up.
Discussion
Osteonecrosis or avascular necrosis is defined as ischemic bone death caused by insufficient blood supply. It represents the final common pathway of several disorders that disrupt osseous blood supply.
Clinically, patients may experience slow-onset groin pain, which could be unilateral or bilateral. This is amplified with weight bearing and relieved with rest. Eventually, range of motion is affected especially hip abduction and internal rotation. These features were evident in both patients discussed.
The condition commonly presents between 30 to 50 years of age and is more common in males than females (ratio of 3:1). Predisposing factors are divided into either traumatic or non-traumatic factors. Traumatic causes commonly mentioned include dislocations; femoral neck fractures and slipped capital femoral epiphyses in children. The list of non-traumatic factors is exhaustive with chronic corticosteroid use mentioned as one of the more common causes. 1 Jamu intake has never been quoted as a non-traumatic factor as little is known regarding its steroid content and side effects of its ingredients. Due to the scarcity of literature regarding this condition resulting from chronic jamu consumption, the incidence is also unknown.
Widespread use of jamu to treat health conditions is common in South East Asia. One of the commonest indications is management of pain. With advancements in preparation methods, jamu is now obtainable in tablet or capsule forms and available in most traditional medical stores and in even certain modern pharmacies. Although this has made jamu preparations more accessible and convenient to consume, local health authorities have emphasized caution and outlawed its sale due to its unknown side effect profile. Despite this, the relative affordability, accessibility and efficacy still make it a prime choice of analgesics for many patients within the South East Asian region. 2,3 These factors influenced the index patient to favor the use of jamu on a regular basis for prolonged durations. Unbeknown to patients, the manufacturing process of jamu is often questionable and dangerous compounds (such as steroids) are often added to increase its efficacy. 4
In the case described, the chronic consumption of jamu containing steroids, highlighted its devastating side effects. Despite the absence of steroids within the formulary, high performance liquid chromatography analysis performed by Sugiarti et al. revealed that each (Montalin, PJ Air Madu, Magelang) tablet contained significant amounts of Dexamethasone within each 500 mg capsule. 4 This finding was also substantiated by a pharmacological review of the patient’s jamu capsules by the Endocrinology team. This significant finding highlights the hazardous non-disclosure of steroids in jamu preparations.
Although omnipotent, steroid use has deleterious side effects. In relation to bone metabolism, steroids modify function, amount and differentiation of osteoblasts while up-regulating osteoclastic activity. This results in inhibition of osteogenesis and reduced remodeling, leading to secondary osteoporosis and increased fracture risks. 5 Besides osteoporosis, hip osteonecrosis is another possible result of chronic steroid consumption and conceivable sequelae from a steroid-induced osteoporotic neck of femur fracture. In the case described, a steroid-induced osteoporotic sub-capital neck of femur fracture occurred first evidenced by the trivial initial injury which subsequently led to osteonecrosis of the femoral head. It is quoted that hip osteonecrosis occurs in as many as 25% of patients taking exceptionally high short-term doses or long-term moderate doses, a sequela that would have occurred with chronic jamu consumption. 6
Patho-mechanistic theories regarding hip osteonecrosis secondary to steroid use are still being debated. Kerachian and colleagues proposed that endothelial cell damage resulting in thrombosis and resultant ischemia is the predominant pathway. Amplified adipogenesis with resultant increase in intra-osseous pressure and resultant ischemia has also been postulated in addition to possible deregulation between apoptosis of osteoblasts and osteocytes in the presence of prolonged osteoclast lifespan and disrupted angiogenesis. 7 –9 The combination of these processes eventually culminate in hip osteonecrosis.
Conclusion
The scarce information regarding steroids in jamu preparations leave an avenue for further analyses and discussion. In an effort to increase awareness regarding the possibility of osteonecrosis occurring secondary to jamu intake, we highlight this case in hope that further research will be done to scrutinize the content of these preparations and suggest tighter regulations on production by relevant health authorities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Consent for publication of case histories and radiographs were obtained from the index patient.