
Abstract
Background/purpose
Vitamin C has been proposed to prevent the incidence of complex regional pain syndrome, but the results are conflicting. We evaluated the effectiveness of vitamin C in the prevention of complex regional pain syndrome-1 after distal end radius fractures in the aging population.
Methods
This was a prospective, randomized study. Patients treated with either conservative or surgical management for distal end radius fracture received Vitamin C (500 mg/day) plus standard therapy or standard therapy alone for a period of 3 months. The presence of complex regional pain syndrome-1 was assessed with Budapest criteria.
Results
The complex regional pain syndrome-I occurred in 11.3% in Vitamin C plus Standard in compared to 26% in Standard therapy alone. Vitamin C was significantly associated with a reduction in the likelihood of exhibiting complex regional pain syndrome-1.
Conclusion
Vitamin C (500 mg/day) supplementation was effective and associated with a lower occurrence of acute complex regional pain syndrome-1. It can be a promising prophylactic option for the prevention of complex regional pain syndrome-1 after distal end radius fracture.
Introduction
Complex regional pain syndrome (CRPS-1), formerly known as reflex sympathetic dystrophy is a complex and multifaceted disorder. CRPS may be defined as a painful and disabling disorder characterized by autonomic dysfunction, inflammatory, trophic changes, and impaired function. 1 CRPS can be classified into type 1 and type 2, of which type 1, without a nerve lesion, is more common with various associated risk factors.2,3
CRPS is one of the most devastating fracture complications, especially of the wrist.4,5 The estimates of the incidence of CRPS after radius fracture vary widely, from 1% to 37%,5–8 and can occur after both operative and non-operative treatments of a distal radius fracture.1,3 With the use of standard scales, the incidence ranges from 1% to 22%.3,9–12
The pathophysiology of CRPS-1 remains unclear with multiple associated risk factors causing uncertainties for diagnosis and management. 13 The CRPS-1 treatment remains largely empirical and symptom-based; hence devising effective preventive strategies is a key clinical focus. Vitamin C, a natural anti-oxidant has emerged as a prophylactic option in the prevention of CRPS.10,11 Exact mechanism is unclear, but Vitamin C is capable of neutralizing the reactive free radicals, which are hypothesized to be implicated in the pathogenesis of CRPS.10,11
In previous studies, vitamin C supplementation has demonstrated efficacy in preventing CRPS-1 in distal end radius fractures,10–12 although the results are conflicting with few. 14 Similar heterogeneities are observed in the reports of several meta-analyses regarding the effectiveness of vitamin C in the prevention of CRPS in distal end radius fracture.15–18 Therefore, the present study evaluated the effectiveness of vitamin C as a prophylactic agent in the prevention of CRPS-1 after distal end radius fractures in the aging population.
Material and methods
This was an open-label, prospective, randomized, parallel design study evaluating the effectiveness of vitamin C in the prevention of CRPS involving patients with a fracture of the distal end of the radius. It was carried out over at tertiary care teaching hospital in Navi-Mumbai (India). The study was conducted in accordance with the ethical standards as laid down in principles of the Declaration of Helsinki and Good Clinical Practice (ICH-GCP) guidelines, Approval of the Institutional Ethics Committee (IEC) was taken, and written informed consent was obtained from participants. The minimum sample size was 132 (66/group) participants, based on a previous randomized control trial (RCT) conducted by Zollinger et al. 10
Patients were enrolled between January 2020 and March 2020 and were followed up for the next 3 months. A total of 150 patients of more than 50 years old of either gender with unilateral distal end radial fractures treated irrespective of the type of management (conservative or surgical) were recruited into the study. After taking informed consent, the patients were randomized to either test or standard group. Participants in the test group received vitamin C (500 mg/day) plus standard therapy (from the day of fracture management), whereas participants in the standard group received only standard therapy (from the day of fracture management) for a period of 3 months, respectively. Standard treatment included post-management administration of calcium (500 mg/day) and vitamin D (1000 IU/day) supplementation for 3 months along with standard physiotherapy care. A computer-generated list of random numbers was used. The participants were randomized with a 1:1 allocation using 4-block randomization.
Patients aged less than 50 years, having existing wrist deformity or wrist disease, having a previous distal radial fracture or bone surgery in the current fractured distal forearm, taking vitamin C or multivitamin therapy prior to the fracture, having a renal impairment, having a muscular disorder, having a psychiatric disorder, and unable to provide consent were excluded from the study.
At the time of enrollment, the general and clinical characteristic of the patients was recorded, including age, gender, the side of the fracture, type of fracture, and the fracture management details.
After fracture management, both group patients were evaluated during routine visits and more often and/or at other times (if necessary) for treatment evaluation, compliance, and CRPS features (continuing pain that is disproportionate to any inciting event and the Budapest criteria complete list of signs and symptoms. 19 An independent assessor made the diagnosis of CRPS-1, from amongst the participants with CRPS features. If CRPS-1 was diagnosed, the endpoint of the study was reached and the study was terminated to allow for further CRPS treatment.
Study evaluation and outcomes
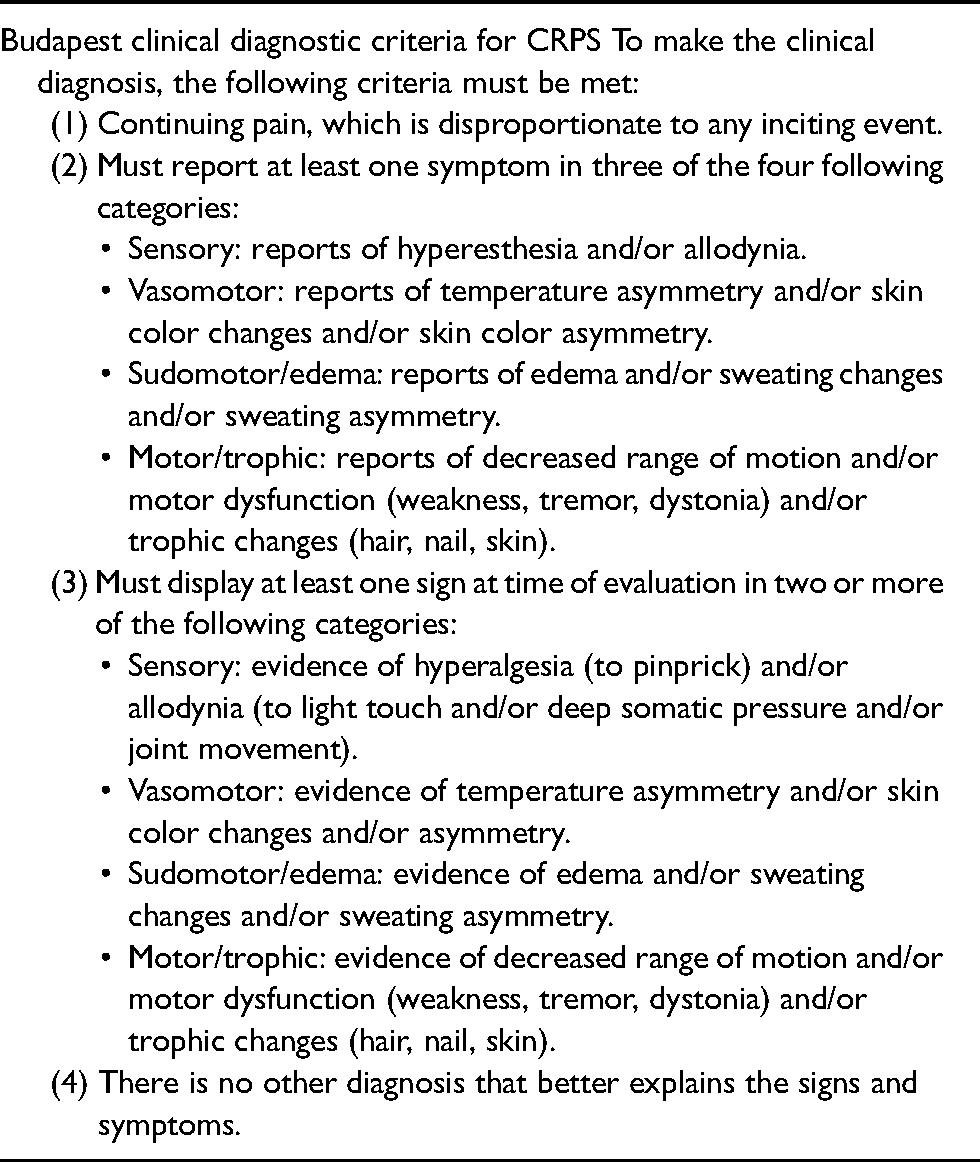
CRPS-1 occurrence: The endpoint of the study was defined as the presence of CRPS-1 using Budapest clinical criteria at any time within 3 months after the fracture management. The Budapest criteria is a validated scale, found to have higher specificity while maintaining sensitivity in the diagnosis of CRPS. 19 As per Budapest diagnostic criteria, CRPS was diagnosed when CRPS characteristics were present in at least three of four symptom categories and in at least two of four sign categories (Table 1). 19
Budapest clinical diagnostic criteria for complex regional pain syndrome (CRPS). 19
Time length for diagnosis of CRPS-1: The average time length for diagnosis of CRPS-1 (time between fracture management and the diagnosis of complex CRPS) was calculated.
Probability of CRPS-1: Kaplan-Meier estimate of cumulative probability of CRPS-1, with the occurrence of CRPS as an endpoint in both the groups, was plotted.
Statistical analysis
Statistical Package for the Social Sciences (IBM SPSS, Windows) software version 20.0 was used for statistical analyses. Data were expressed as an actual number, mean ± standard deviation, and frequency (percentage) as appropriate. Data normality was assessed using the Kolmogorov-Smirnov test. The independent t-test was applied to quantitative variables. Chi-square was used for categorical variables. A measure of association along with their confidence intervals was calculated with the Pearson chi-square test. Relative risk was also calculated. Logistic regression was conducted for the likelihood ratio with complex regional pain syndrome as a dependent variable. Kaplan-Meier estimate with 95% confidence interval for both groups was plotted for time to event analysis, with the occurrence of CRPS as endpoint and was compared by log-rank test p-values <0.05 were considered statistically significant.
Results
Of the 150 participants that were enrolled, six were excluded due to lack of follow-up or underwent a secondary management/second operative procedure. The final analysis was conducted on 144 participants. Of the 144 participants, 71 participants received vitamin C along with standard treatment, and 73 participants received standard treatment.
General characteristics
The general characteristics of the participants in both groups are summarized in Table 2. The majority in both the groups had fractures of the distal end of the radius involving the right wrist The mean age of the participants in the vitamin C plus standard group was 56.5 ± 5.3 years, whereas in the standard group, it was.57.6 ± 8.5 years. There were no significant inter-group differences in general characteristics (Table 2).
General characteristics of the patients in both groups.
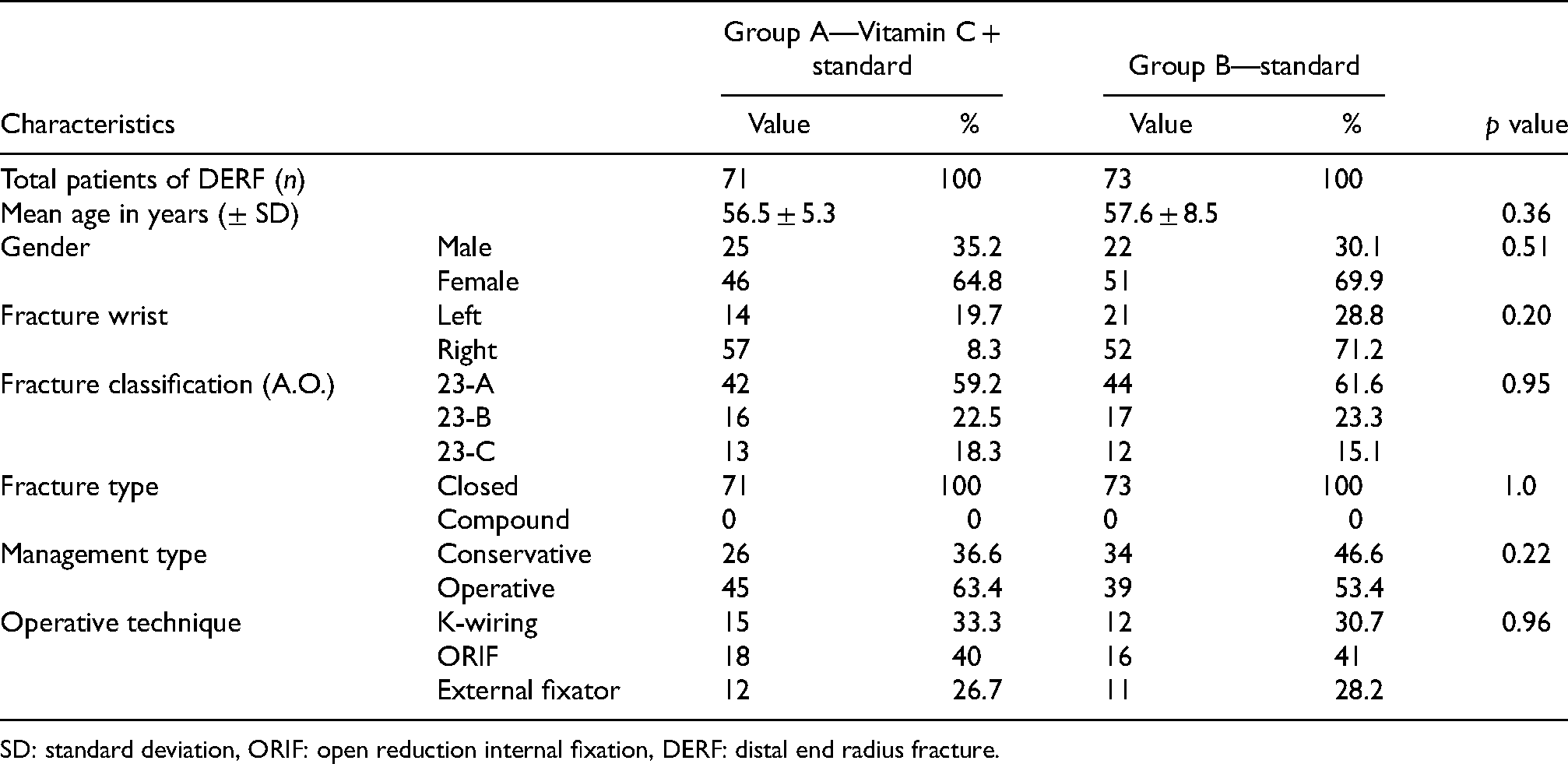
SD: standard deviation, ORIF: open reduction internal fixation, DERF: distal end radius fracture.
Frequency of CRPS-I occurrence
Overall, the prevalence of CRPS-I in the entire study cohort was 18.8% (27 of 144). The CRPS-I occurred in 11.3% of vitamin C plus Standard group participants (8 of 71), as against 26% (19 of 73) in standard group participants (Table 3). There was a significant difference between the vitamin C plus standard and the standard group (p = 0.023), in which the relative risks of CRPS-I were 0.43 (95: 0.20–0.92).
Occurrence of CRPS-1 in the two groups.
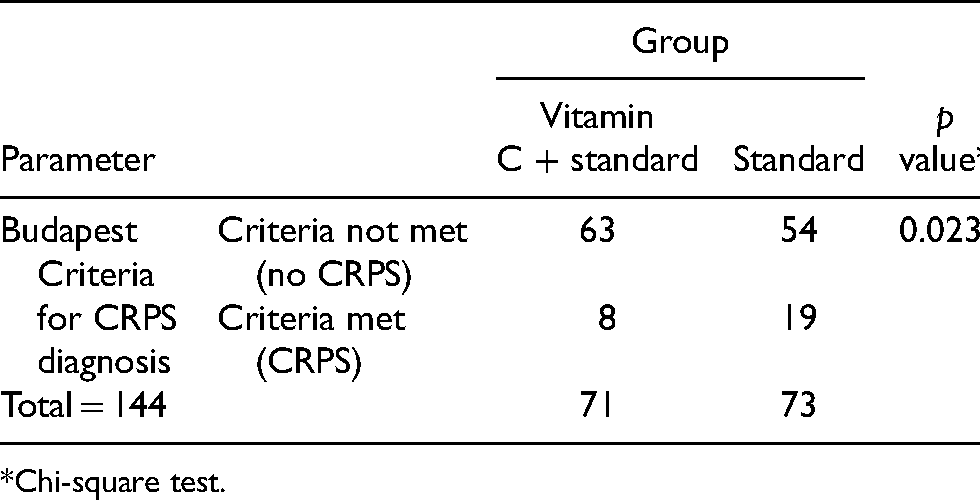
*Chi-square test.
Logistic regression was performed to ascertain the effects of gender, smoking, alcohol, comorbidities, fracture classification, and vitamin C (500 mg) therapy on the likelihood of CRPS-1. In the logistic-regression analysis, vitamin C (500 mg) therapy had significant odds ratios (odds ratio: 3.01, 95% confidence interval: 1.12–8.13, p = 0.029) and was associated with a reduction in the likelihood of exhibiting CRPS-1. Gender, smoking, alcohol, and comorbidities were not found to be associated predictive factors for CRPS-1; however fracture classification was significantly associated (p < 0.001).
Time length for diagnosis of CRPS-I
Overall, CRPS-I was diagnosed at an average of 66 ± 12 days after fracture management. The average time length for diagnosis of CRPS-I was 70 days in the vitamin C plus standard group, whereas it was 64 days in the Standard group. However, this difference was not significant (t = 1.094, p = 0.284).
Probability of CRPS-1
Kaplan-Meier's estimate of the cumulative probability of no CRPS-I was higher and significant in the vitamin C plus standard group (88.7% vs. 74%, p = 0.020) in comparison to the standard group (Figure 1).
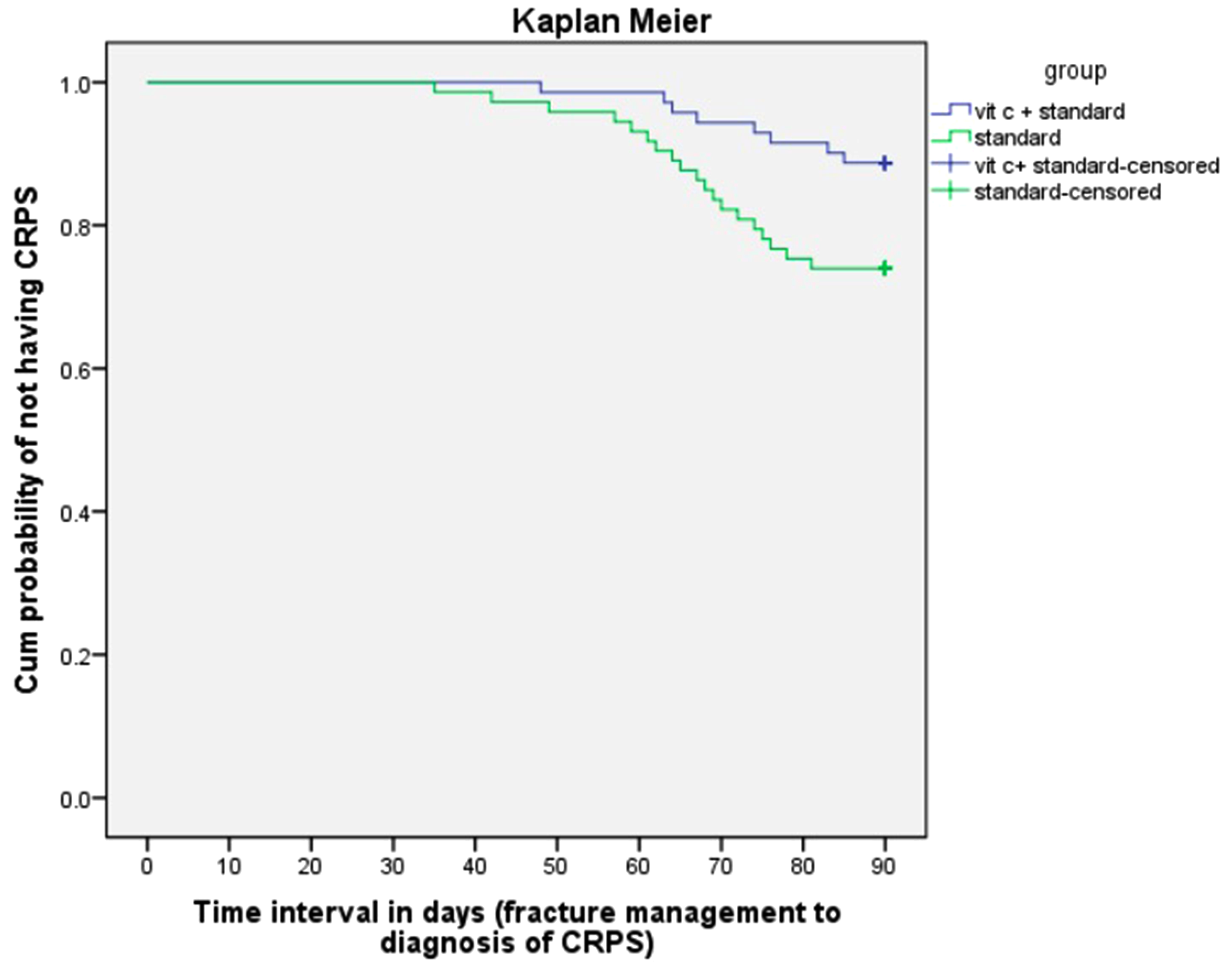
Kaplan-Meier's estimate for both groups, with the occurrence of complex regional pain syndrome (CRPS) as the endpoint.
Discussion
The findings of this study documented that vitamin C (500 mg/day) supplementation for 90 days was associated with a lower occurrence of acute CRPS-1, suggesting that vitamin C supplementation is a promising option for prophylactic use in the prevention of CRPS-1 after DERF in the aging population.
CRPS-1 is a devastating, painful condition causing impairment in function and quality of life. There is a high prevalence of CRPS after fracture of the distal radius.5–8 The estimates of the incidence of CRPS after radius fracture vary widely (1–37%).5–9 This varying incidence could be due to heterogeneity in the utilization of scales and the lack of a gold standard test for CRPS diagnosis. With no definitive cause or treatment, its management is a challenge. Prevention is desirable, particularly as there is no definitive treatment. Several clinical trials have documented that vitamin C could have some efficacy related to its antioxidant properties in preventing CRPS-I in distal end radius fractures.10–12 However the results of previous study 14 are conflicting, leading to heterogeneous inference.
In this study, we documented that prophylactic vitamin C (500 mg) supplementation along with standard treatment showed a significantly lower incidence of CRPS-I in comparison to standard treatment alone (11.3% vs. 26%, p = 0.023).
Zollinger et al.10,11 in two placebo-controlled, randomized clinical trials documented that vitamin C (500 mg) for 50 days decreased the risk of CRPS after wrist fractures. Zollinger et al. 10 in 1999 reported the occurrence of CRPS of 7% in the vitamin C (500 mg/day) group and 22% in the placebo group. Similarly, Zollinger et al. 11 in 2007 reported the prevalence of CRPS of 2.4% for the overall vitamin C group and 10.1% in the placebo group (p = 0.002). On subgroup analysis, the prevalence of CRPS-1 was lower and significant in vitamin C (500 mg/day) than in the placebo group (p = 0.007). The author's recommended vitamin C (500 mg /day) for 50 days for CRPS prevention in wrist fractures. 11 Similarly, Cazeneuve et al. 12 found a lower prevalence of CRPS in the vitamin C (1 gm/day for 45 days) group than the control group.
Based upon the consistent findings and the level of evidence of the two trials, the American Academy of Orthopaedic Surgeons (2010-AAOS) Clinical Practice Guideline has included and suggested adjuvant treatment of distal radius fractures with vitamin C for the prevention of disproportionate pain (moderate strength recommendation). 20 Our findings are similar and support the vitamin C efficacy findings of previous studies (Zollinger et al. and Cazeneuve et al.).10–12
However, a recently published trial reported a conflicting result. Ekrol et al. 14 documented a contradictory result, demonstrating no significant reduction in the prevalence of CRPS at one year in patients with either a displaced or non-displaced fracture treated with vitamin C (500 mg) daily for 50 days compared with Placebo. There was a significantly greater prevalence of CRPS at 6 weeks in the vitamin C group in the non-displaced fracture cohort (p = 0.022). Similar heterogeneities are observed in the reports of several meta-analyses regarding vitamin C in the prevention of CRPS in distal end radius fracture.
The meta-analysis by Evaniew et al. 16 and Aim et al. 17 of only randomized controlled trials documented that the relative risk (RR) of CRPS-1 after a wrist fracture was not significantly diminished in the group given vitamin C in any dose (200, 500, or 1500 mg). Heterogeneity was high and statistically significant.16,17 However, in the Aim et al. 17 meta-analysis, when the analysis was confined to the 500 mg vitamin C dosage versus placebo, they documented the RR of CRPS-I was 0.54 (95%CI, 0.33–0.91; p = 0.02). 17 The risk of CRPS-1 was significantly decreased by vitamin C in the 500 mg dosage. The heterogeneity rate was 65% and non-significant. They concluded that vitamin C 500 mg daily supplements for 50 days decreased the risk of CRPS-1 after wrist fractures. 17
In this study, overall the prevalence of CRPS-I was 18.8%, which is lower than the population-based studies.5–9 This could be due to the fact that we used a validated clinician-based assessment scale rather than a patient-reported scale.
In this study, the average time length for diagnosis of CRPS-I was 66 days. This finding is consistent with the result of the average time length of 76 days reported by Zollinger et al. 11 However, in our study, the diagnosis of CRPS was earlier for the patients in the Standard group than Vitamin C plus Standard group (average 64 days vs. 70 days), which is opposite to the findings of Zollinger et al. 11 in which diagnosis of CRPS was made earlier for the patients in the vitamin C group than Placebo group (average 68 days vs. 83 days).
In this study, the cumulative probability of not having CRPS-I was higher and significant in Vitamin C plus Standard group (88.7% vs. 74%, p = 0.020) than in the standard group. Similarly, a higher probability of not having CRPS was observed in the vitamin C group than in the placebo group (p = 0.0009) in the Zollinger et al. 11 study.
Overall in this study, supplementation of vitamin C (500 mg) daily for 90 days along with standard treatment was associated with lowering the risk of CRPS-1 in patients with distal end radius fracture. However, further robust randomized control trials with a larger sample size are warranted to validate these beneficial results and for the recommendation.
Various criteria exist for the diagnosis of CRPS.19,21 However, they are limited by self-reported symptoms and lack incorporation of motor and trophic features commonly associated with CRPS. 19 The strength of this study is that we used a newly validated Budapest diagnostic criterion, 19 which is based on the clinical decision and has a higher specificity and good sensitivity for CRPS diagnosis.
Limitations
The present study has certain limitations. This was a pilot study with a heterogeneous treatment pattern. The research was conducted in a single-center hospital, with a small sample size and a limited duration of three months. The study design was open-label, which may be influenced by subjective bias. Participants’ usual dietary vitamin C intake and dietary pattern were not assessed, which may influence and be one of the reasons for the conflicting results in literature studies. We observed the acute CRPS occurrence for a time period of three months post-management and hence are not able to conclude on the long-term incidence of CRPS and its evaluation. Post-discharge rehabilitation was not accounted for, which could also influence the findings.
Conclusions
In conclusion, our results suggest that vitamin C (500 mg/day) supplementation was associated with a lower occurrence of acute CRPS-1 after distal end radius fracture. Vitamin C (500 mg/day) supplementation thus can be a promising prophylactic option for the prevention of CRPS-1. However, further robust randomized control trials with a larger sample size are warranted to validate these beneficial results for further recommendation.
Footnotes
Ethics approval
This study was approved by our Institutional Ethics Committee (Approval reference no. DYP/IECBH/2020/05).
Statement of human and animal rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of informed consent
Informed consent was obtained from all individual participants included in the study.
Role of the funding source
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.