
Abstract
Background/Purpose
Knee joint line is commonly defined as a tangent to medial and lateral tibial plateaus in various radiographic measurements. We aim to investigate radiographic differences between medial and lateral knee joint line coronal obliquity. It has significant implication on radiographic analysis following unicompartmental knee arthroplasty.
Methods
We analysed the knee radiographs of 48 young patients (mean age 25.1 + /-5.6 years) with 50 anterior cruciate ligament-deficient knees. Medial and lateral tibial plateau coronal obliquity were defined as angles between femoral knee joint line and the tangent to articular surface of each tibial plateau. Mediolateral differences and linear correlation were analysed.
Results
Significant difference was found between medial (mean = -1.5, SD = 2.4 degrees) and lateral obliquity (mean = + 0.6, SD = 3.0 degrees) (p < 0.001). The mean mediolateral difference was 3.1 degrees (SD = 2.8, range 0–11.8 degrees), without significant correlation (r = 0.085, p = 0.56).
Conclusion
Mediolateral differences exist in knee joint line obliquity. Each compartment should be considered separately when measuring knee joint line obliquity.
Keywords
Introduction
Knee joint line obliquity has been traditionally defined as the angle between the horizontal line and the tangent to both medial and lateral tibial plateaus. It is an important parameter to measure knee joint line coronal alignment after high tibial osteotomy, unicompartmental and total knee arthroplasty. Its pre-existing definition is based on the assumption that the two articular surfaces are parallel and aligned so that a tangential line can be drawn across both tibial plateaus to define the knee joint line. However, anatomical differences clearly exist between medial and lateral tibial plateaus, the lateral being convex while the medial being concave in shape. Hence it might be inaccurate radiographically to draw a tangent across the two surfaces, which are not necessarily aligned. Up to the authors’ best knowledge, there is as yet no literature investigating differences between medial and lateral tibial plateau coronal obliquity. The answer to this question is critical in conceptualizing and defining knee joint line obliquity, hence leading to improved measurement accuracy. Furthermore, should there be significant differences, any potential correlation between medial and lateral tibial plateau coronal obliquity might be helpful in estimating the pre-arthritic joint line in patients with tibial plateau bone loss.
Methods
We retrospectively recruited 48 young patients (40 male and 8 female ; mean age = 25.1 + /-5.6 years) with 50 anterior cruciate ligament-deficient knees from our clinical database of anterior cruciate ligament reconstruction preoperative workup.
There was no prior study to measure medial and lateral joint line obliquity separately. Hence the sample size estimation was based on the assumption of effect size being 0.85, indicating a large effect, with the power at 0.8 and significance level at 0.05. A minimum of 46 patients was required to detect statistically significant difference with paired t-test
Inclusion criteria were patients without significant collateral ligament laxity of their knees (which might potentially affect directions and degrees of joint line obliquity), age below 40 years old, absence of mechanical knee pain and joint line tenderness to suggest pre-existing knee arthritis. Exclusion criteria included radiographic evidence of knee osteoarthritis with Kellgren and Lawrence grading of 2 or above, prior ipsilateral knee bony surgery which could affect localization of bony landmarks for measurement, coexisting bony pathology including trauma and tumour, any flexion contracture or genu recurvatum which might preclude standardized radiograph-taking.
Standardized anteroposterior non-weight-bearing preoperative radiographs of the 50 anterior cruciate ligament-deficient knees were used for measurement. All the knee radiographs were taken using a standardized protocol at the authors’ institute. Patients lied supine on a couch with knee relaxed and fully extended at 0 degrees. Patients’ legs were positioned in slight internal rotation so that patella faced upward. Standard anteroposterior knee radiographs were taken to include distal femur and proximal tibia. Neutral rotation was ensured as indicated by one-third of fibula head superimposed by the lateral tibial plateau and central patella position. Suboptimal radiographs were defined by malrotation, as indicated by either eccentric patella position or inappropriate amount of fibula head overlapping with tibial plateau. All radiographs were scrutinized to ensure neutral rotation.
As a reference for mediolateral comparison, femoral knee joint line was defined as a line intersecting the most distal points of medial and lateral femoral condyles (Figure 1).

Femoral knee joint line.
Since medial and lateral tibial plateaus differ in shape, we took the line joining the two edges of each plateau's articular surface to dictate the overall inclination of the respective knee compartment. We excluded the tibial spine which was not articulating with the femoral condyle, hence deemed not pertinent to the joint line obliquity concerned. We then defined medial (MJLO) and lateral joint line obliquity (LJLO) as the angles between the femoral knee joint line and the line joining the most medial and lateral points of articular surface of each tibial plateau. The apparent point of transition from tibial plateau articular surface to tibial spine was chosen to exclude the tibial spine. Positive angles denoted lateral inclination while negative angles denoted medial inclination, with reference to femoral knee joint line (Figures 2 and 3).
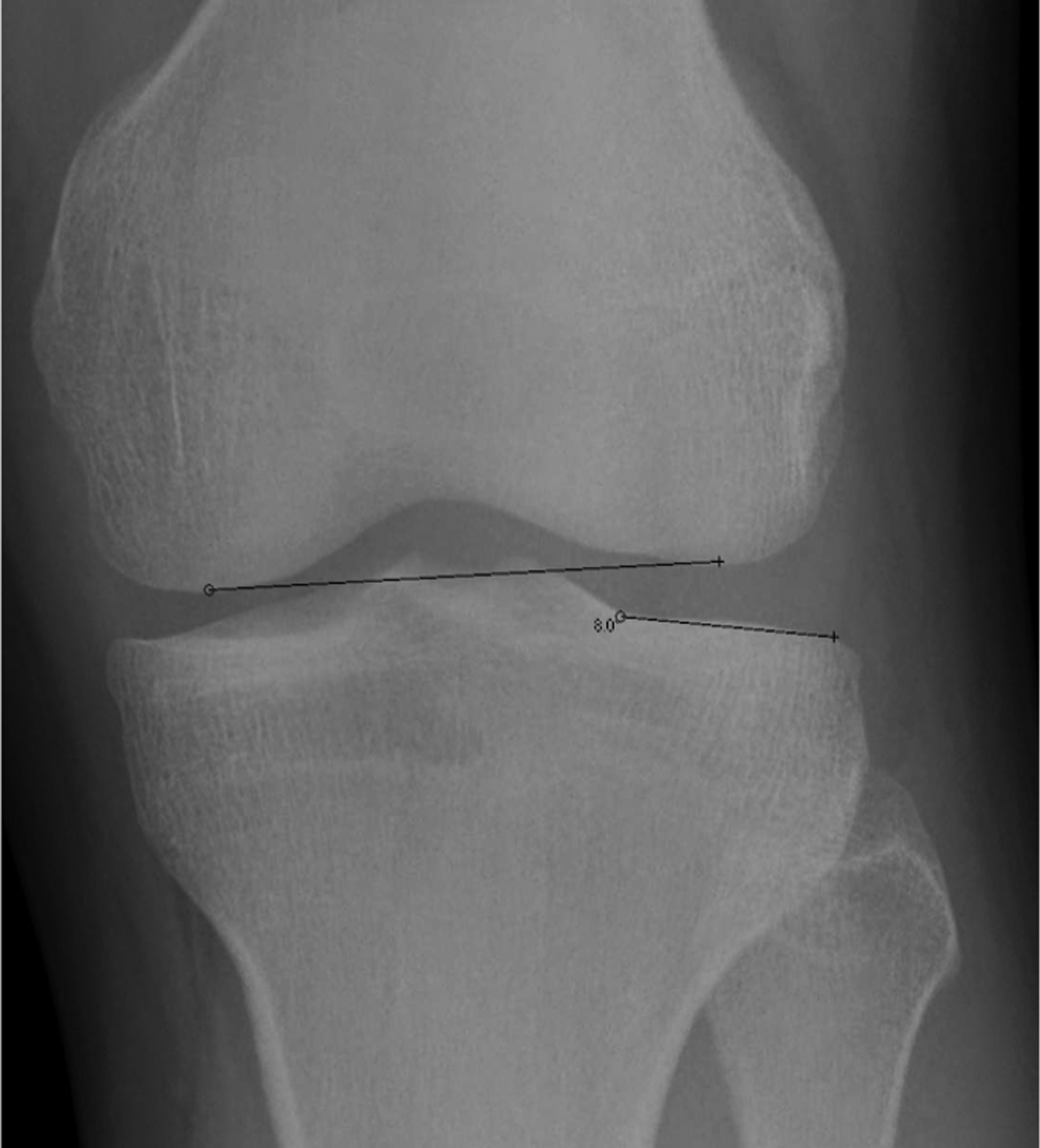
Lateral joint line obliquity.
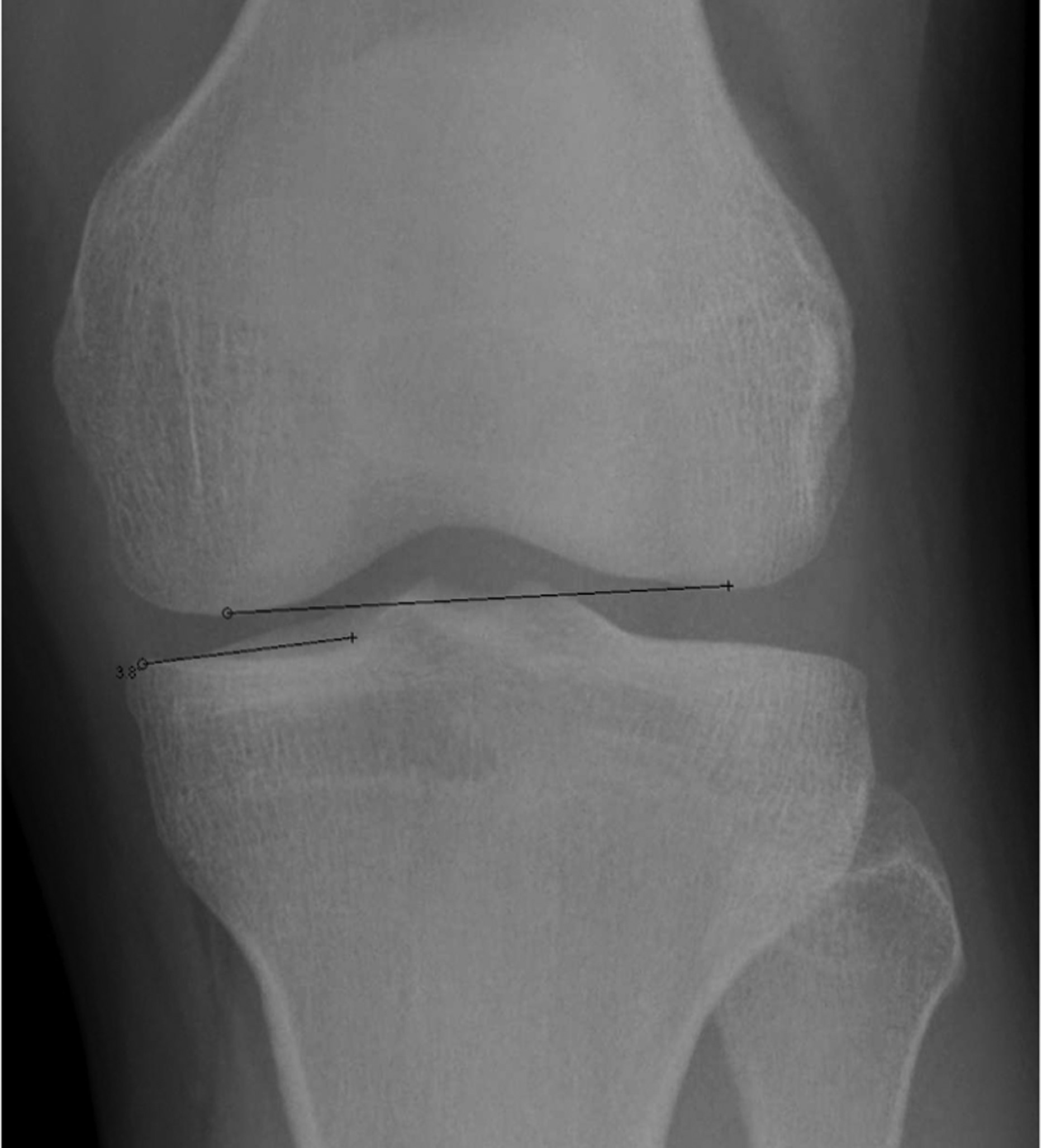
Medial joint line obliquity.
The measurements in all patients were performed and repeated by one author 12 weeks apart. Another author repeated the measurements twice 2 weeks apart independently in all patients. Both observers’ intra-observer reliabilities were excellent, as shown by intraclass correlation coefficients above 0.8 for both medial and lateral obliquity. Inter-observer reliability was moderate to good, as shown by intraclass correlation coefficient (0.75 for lateral obliquity, 0.57 for medial obliquity).
Results
Significant difference was found between medial (mean = -1.5, SD = 2.4 degrees) and lateral obliquity (mean = + 0.6, SD = 3.0 degrees) (p < 0.001). The mean difference was 3.1 degrees (SD = 2.8, range 0–11.8 degrees). The distributions of lateral and medial tibial plateau coronal obliquities are depicted in Figure 4.
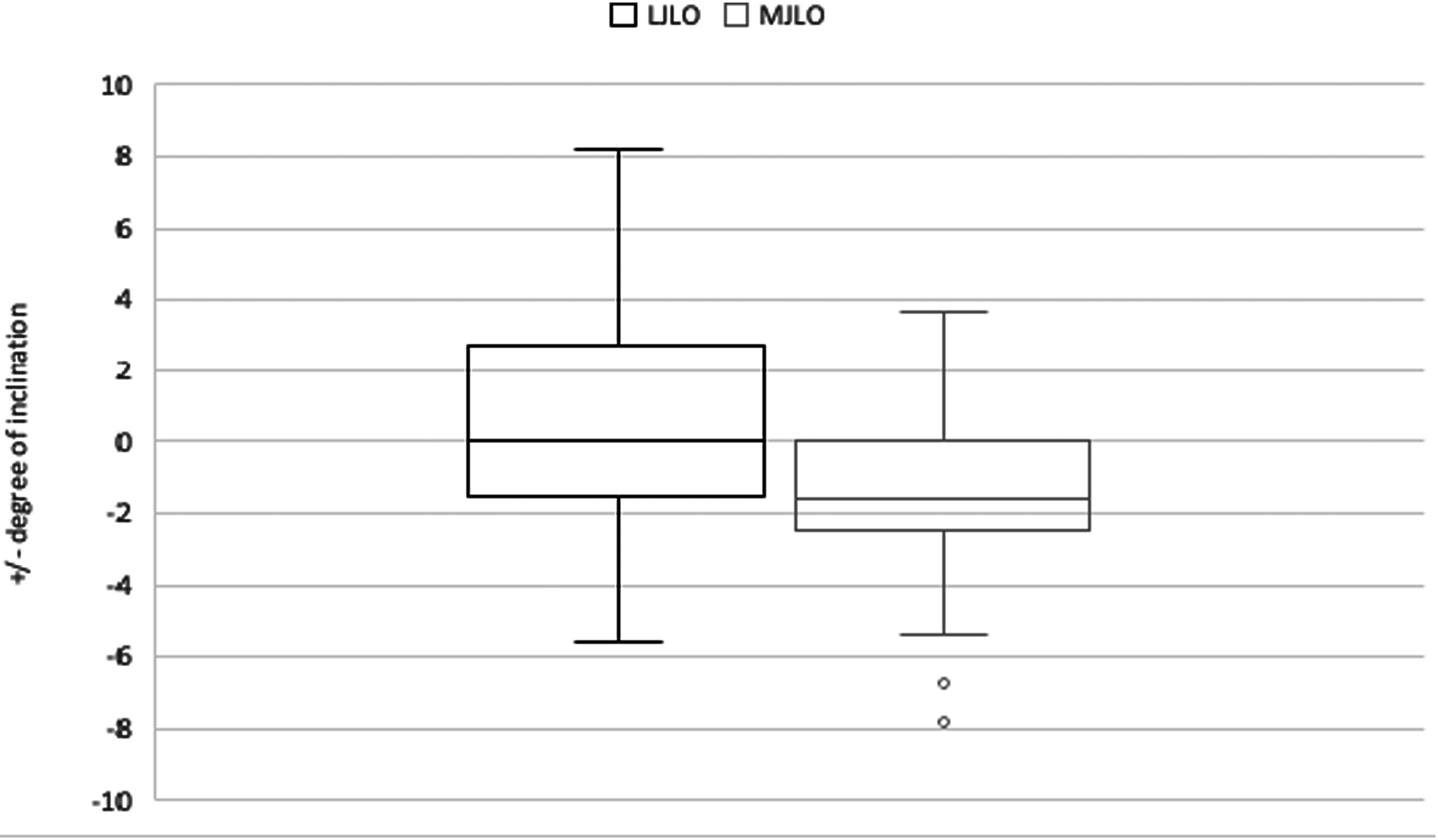
Box and whisker plot of lateral joint line obliquity (LJLO) and medial joint line obliquity (MJLO)
To adjust for radiographic and measurement errors, 2 degrees was taken as an arbitrary cutoff to stratify data into 3 groups, −2 to + 2 degrees, <-2 degrees and > + 2 degrees (Table 1).
Numerical distribution of medial and lateral tibial plateau coronal obliquity.
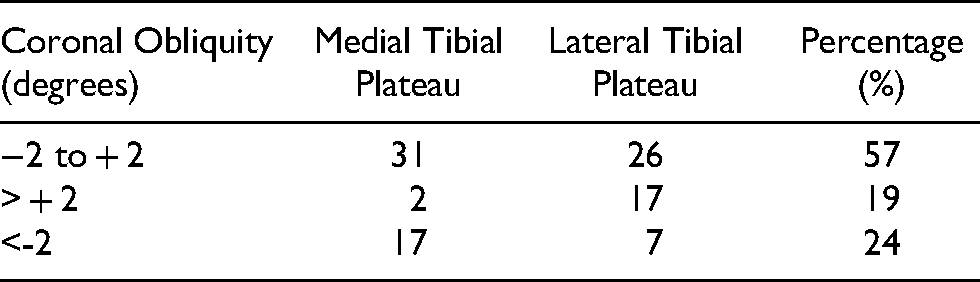
The latter two groups were considered more representative of clinically significant obliquity. For lateral tibial plateau obliquity, 26 out of 50 were within −2 to + 2 degrees, while 17 out of the remaining 24 were > + 2 degrees, i.e. laterally inclined. For medial tibial plateau obliquity, 31 out of 50 were within −2 to + 2 degrees, while 17 out of the remaining 19 were <-2 degrees, i.e. medially inclined. In other words, we observed a trend of lateral inclination of lateral tibial plateau, and medial inclination of medial tibial plateau. Pearson correlation revealed no significant linear correlation between medial and lateral obliquity (r = 0.085, p = 0.56).
Discussion
Knee joint line obliquity in native knee has been widely reported in previous literature. Tang et al. reported medial inclination of knee joint line in 50 Chinese young subjects with 100 knees (5.4 + /- 2.5 degrees in female and 4.9 + /- 2.3 degrees in male). 1 Yau et al. also found an average of 5 + /- 3 degrees of medially inclined knee joint line obliquity in Chinese. 2 Similar radiographic studies by Hsu et al. and Moreland et al. found less medial inclination in Caucasian (1 and 3 degrees respectively).3,4 Bellemans et al. also defined knee joint line as tangent to both tibial plateaus in measuring medial proximal tibial angle, and concluded medial inclination of 3 + /- 2 degrees. 5 Victor et al. concluded that knee joint line is parallel to the floor in both constitutional varus and neutral knees, with mean tibial joint line angle 0.3 + /- 2 degrees. 6 Moreover, Howell et al. reported more varus alignment of tibial joint line after kinematically aligned total knee arthroplasty, resembling native knee. 7
All of the above-mentioned defined the knee joint line obliquity as the angle between the horizontal and the tangent to both medial and lateral tibial plateaus. However, despite such pervasive assumption of mediolateral parallelism, there is no prior studies investigating differences between medial and lateral tibial plateau coronal obliquity. Our results of significant mediolateral differences in directions and degrees of obliquity posed a legitimate challenge to the existing definition of knee joint line obliquity. In addition, it would be worthwhile to further investigate whether both sides of knee of the same patient would be similarly inclined. The answer to it would hopefully provide hints on predicting native joint line obliquity in patients with tibial bone loss.
Several limitations of this radiographic study should be noted. First, this study was biased toward relatively young patients with anterior cruciate ligament injury from our database, with male predominance. This was limited by the availability of our preoperative database of knee radiographs, to eliminate unnecessary radiation hazard to young individuals. In the absence of established correlation between ACL deficiency and coronal joint line obliquity, the authors believed that the inclusion bias would not pose significant impact on the results. We did not include patients with established osteoarthritis which often involved medial compartment-predominant degenerative changes, hence leading to sources of errors in comparing medial and lateral joint line obliquity. Instead, the group of anterior cruciate ligament-deficient patients was chosen because they were at increased risk of developing osteoarthritis, hence more representative of the pre-arthritic knee joint line. 8 Second, despite efforts in standardizing radiographs, some degree of minute variations including femoral malrotation were inevitable. Moreover, all radiographs were taken supine. Ideally, weight-bearing radiographs could have been taken and measured to provide more information on the functional knee joint line on standing. Although CT scan would have allowed more accurate measurement as bony landmarks and rotational alignment could be more precisely defined, its radiation hazards would preclude its ethical use. As this is our preliminary radiographic study to screen for mediolateral difference in coronal joint line obliquity, we shall further investigate with magnetic resonance imaging to verify the findings. However, we believe that radiographic measurement is more applicable in the clinical setting, on the ground that majority of preoperative planning in primary knee arthroplasty was solely based on knee radiographs. In addition, despite the excellent intra-observer repeatability, the interobserver repeatability was only moderate to good. It might be explained by the fact that the point of transition from articular surface of tibial plateau to tibial spine was chosen arbitrarily by the observer. Nevertheless, through adjusting for potential measurement errors by the 2 degrees cutoff which approximates the standard deviation of most of the above-quoted values, our results demonstrated a trend of mediolateral discrepancy in the direction of obliquity. When compared to previous literature which did not take into account the disparity of mediolateral obliquity directions, we believe our methodology of measurement is more accurate and clinically relevant than assuming a tangent across two nonaligned surfaces.
Our study has significant clinical implications. This is a pioneering study to prove differences between medial and lateral tibial plateau coronal obliquity.
Footnotes
Acknowledgements
Dr Yau, Wai Pan, Associate Professor of the Department of Orthopaedics and Traumatology, University of Hong Kong, is acknowledged for providing the database and radiographs for analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.