
Abstract
Keywords
Introduction
Fractures of the phalanges are among the most common fractures in children and the majority of cases are treated conservatively with early, protected mobilization.1,2 Phalangeal neck fractures incidence is estimated at 14%–50% of finger fractures in the pediatric population, and represent a special subset of phalangeal fractures.3,4 They pose challenges to the treating physician both in regards to determining operative versus non-operative treatment courses and in choosing appropriate fixation techniques. 5 Also termed “subcondylar” or “subcapital” fractures, these injuries are extra-articular, transverse fractures through the distal aspect of the proximal or middle phalanx.6,7 Due to the distal condylar fragment of these fractures being incompletely ossified in young children, the injuries have also been called the “cartilaginous cap” fracture.8,9 Typically, the fracture assumes an apex volar angulation at the fracture site, with concomitant dorsal displacement of the cartilaginous cap. 10 Based on the degree of displacement and bony contact, phalangeal neck fractures are classified according to the Al-Quattan classification system: Type 1—non-displaced; Type 2—displaced with bone-to-bone contact at the fracture; Type 3—displaced with no bone-to-bone contact. 11
Aggressive attempts at performing closed reduction in the emergency department have been discouraged due to the risk of fragmenting the distal segment. 12 The fractured phalangeal neck also is relatively ischemic after injury, receiving blood supply only from the soft tissue attachment of the collateral ligaments.12,13
Many advocate the prompt reduction and fixation of these fractures given their propensity for displacement, instability, and avascularity.14,15 Controversy exists over the proper reduction technique with some supporting reduction by closed means to reduce any risk of further devascularization of the condyles and subsequent avascular necrosis.13,15,16 On the other hand, others advocate open reduction due to difficulty correcting deformity by closed means. 17 It goes without saying that restoring anatomic alignment, providing bony stability, preserving vascularity, and initiating an appropriate post-treatment rehabilitation protocol are essential to good functional outcomes.
The purpose of this study is to retrospectively evaluate non-operative and operative treatment of subcapital phalangeal neck fractures in a pediatric population over a 5-year period, with specific attention given to decision-making on operative versus non-operative management, complications following treatment, and functional outcomes.
Materials and methods
A retrospective review was performed on all children treated for subcapital phalangeal fractures from 2009 to 2014 with institutional review board approval. To identify these injuries, International Classification of Diseases 9 codes 816.01, 816.03, and 816.13. Inclusion criteria were age 18 years or younger at injury with a proximal or middle phalanx neck fracture. Exclusion criteria included patients with fractures proximal to the phalangeal neck, missing initial, and final radiographs, unicondylar/bicondylar fractures of the phalangeal head, previous attempts at treatment by another physician, and failure to complete follow-up. No minimum duration was established for follow-up only that bony union was achieved with absence of tenderness at the fracture site. This did not explicitly exclude non-unions but filtered out patients who missed their follow-up clinic visits.
These criteria produced a study cohort of 177 patients. The cohort was split into non-surgical and surgical groups with the surgical group containing two subgroups of open reduction internal fixation (ORIF) using Kirschner wires and closed reduction percutaneous pinning (CRPP). Immobilization included a short or long-arm cast that includes the fingers in the younger population. A dorsal splint maintaining interphalangeal joint flexion may be utilized in older patients. The non-surgical group contained those patients whose fractures were treated conservatively with early splinting and immobilization, or in whom surgery was not deemed necessary based on radiological imaging/surgeon judgement. Patient demographics, mechanism of injury, initial and final radiographic parameters, treatment, time to treatment, and complications such as hardware loosening were recorded. Radiographs were measured for initial displacement and angulation, post intervention displacement/angulation, and displacement/angulation on final follow-up. All measurements were made on digital images using radiographic measuring software.
Demographic and clinical differences between the groups were compared using two sample t-tests with means and standard deviations (SD) or Wilcoxon rank-sum test with median and interquartile range (IQR), and chi-square and Fisher's exact tests for categorical variables. To determine whether there was an association between final follow-up radiographic parameters and treatment group, linear regression models, considering initial parameters as covariates, were used. R version 3.1.1 software (R Foundation for Statistical Computing, Vienna, Austria, http://www.R-project.org/) was utilized.
Results
Four-thousand and eighty-nine charts were reviewed and 282 cases of phalangeal neck fractures were identified. Of these, 105 were ineligible due to insufficient data or lack of follow-up, leaving 177 cases with a mean follow-up of 43 days (SD: 28, range: 12–195). Median age was 8.6 and 9.2 years for operative and non-operative groups, respectively. The most common mechanism of injury was crush (27%), followed by axial loading (18%) and hyperextension (12%). Almost half (43%) of the charts did not have a clear mechanism described (e.g. “fall”). There were 119 fractures (67.2%) treated non-operatively and 58 fractures (33.8%) treated operatively. The small finger was predominately-affected (57.5%) followed by index (14.5%), long (12%), ring (11%), and thumb (5%). The proximal phalanx represented 128 (72.3%) fractures versus 51 (27.7%) of the middle phalanx. The right (57%) extremity was more frequently injured than the left (43%). The Al-Quattan classification identified type 1 as the most prevalent and both type 2 and 3 were significantly more likely to be associated with the surgical group (Table 1).
Demographic and clinical characteristics.
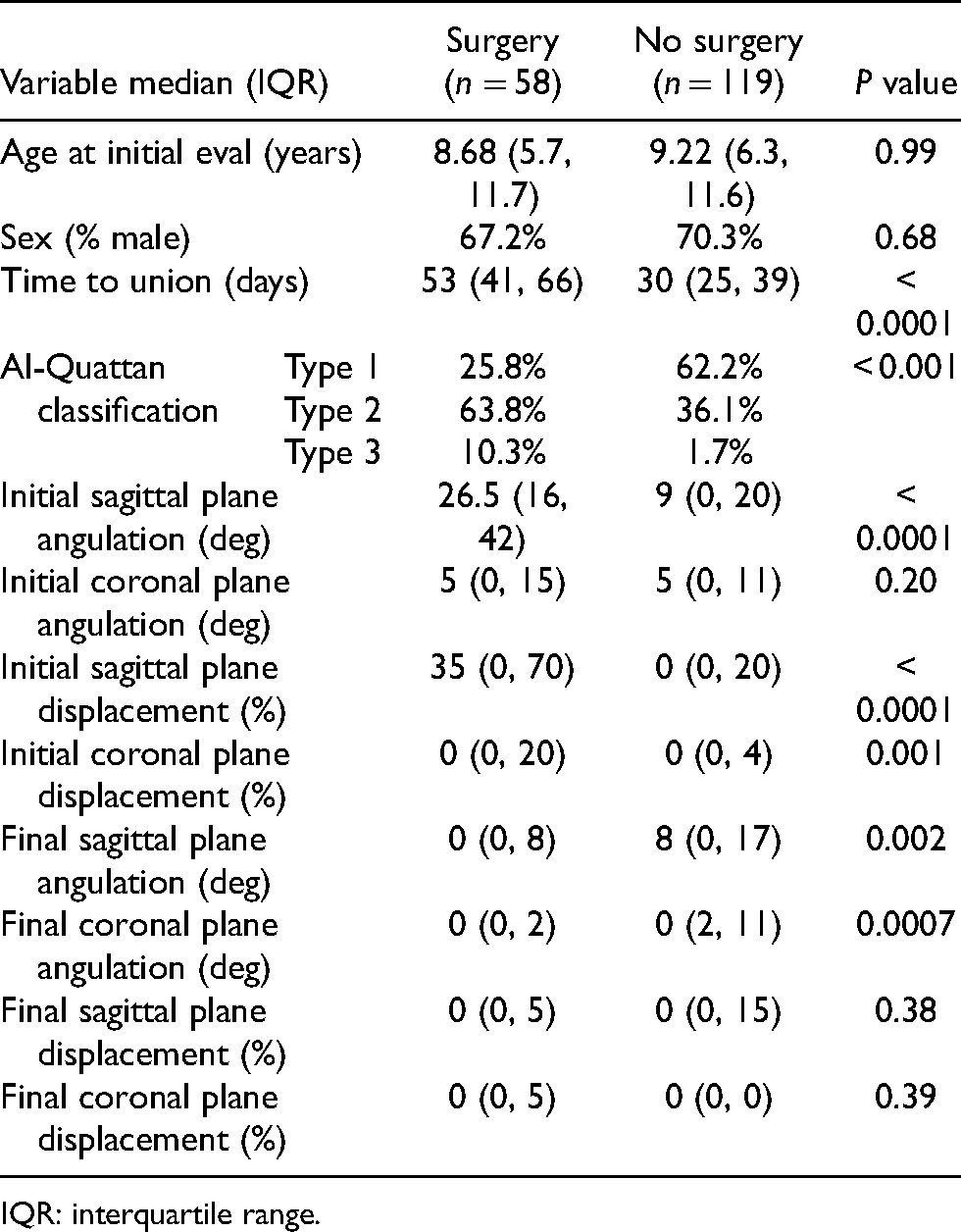
IQR: interquartile range.
On initial injury radiographs, the translational displacement of each fracture was measured as the percentage of the phalangeal width (Figure 1). Initial sagittal plane displacement was median 0% (IQR: 0, 20) in the non-operative group, compared with 35%(IQR: 0, 70) in the operative group (p < 0.0001). The median (IQR) displacement in the coronal plane was 0% (0%, 20%) in the non-operative group, compared with 0% (0%, 4%) in the operative group (p = 0.0001). The angulation of the distal fragment was measured in degrees (Table 1). In the sagittal plane, the median sagittal angulation was 9° (IQR: 0, 20) for the non-operative group, compared with 26.5° (IQR: 16, 42) in the operative group (p < 0.0001). The median coronal angulation was 5° (IQR: 0, 11) in the non-operative group, compared with 5° (IQR: 0, 15) in the operative group (p = 0.20).

Coronal view of a displaced proximal phalanx neck fracture in the second finger of a 4 year old.
Final follow-up radiographs indicated a significant difference between operative and non-operative groups in the correction of sagittal angular deformity and coronal angular deformity, after adjusting for initial deformities (Figure 2). Surgical treatment corrected initial deformity more than non-surgical treatment by 14° (95% CI: −19, −9) in the sagittal plane (p < 0.001). In the coronal plane, surgical treatment corrected initial deformity more than non-surgical treatment by only 2° (95% CI: −4, 0), which did not reach statistical significance (p = 0.09).

At 6 weeks follow-up the proximal neck fracture from Figure 1 shows progressive healing.
The non-operative group had a median time to union of 30 days (IQR: 25, 39 days), defined as absence of tenderness on exam and radiographic evidence of healing. Those requiring surgery (CRPP or ORIF) had an average time to union of 53 days (IQR: 41, 66), nearly twice as long as the non-operative group (p < 0.0001). Within the operative group, those that underwent CRPP had a median time to union of 51.5 days (IQR: 40, 60), compared with a median 67 (IQR: 45, 101 days) for the group that had open reduction (p < 0.06). Overall, both closed and open surgical treatment led to an increased time to union. In a subgroup analysis, we evaluated patients who had between 16 and 25 degrees of sagittal angulation for both the non-operative and surgery groups. We found that the median time to union for the non-operative group was 33 days (IQR: 27–44, n = 22) while it was a median of 58.5 days (IQR: 44–83, n = 14) for the surgical group. Median percent of sagittal displacement was 20% versus 30% for the non-operative group and surgical group, respectively (p = 0.53). The 75th percentile within the surgical group included sagittal displacement values of 50% compared to 30% in the non-operative group that may explain the 25 extra days until union in the surgical group relative to the non-operative group.
Within the operative group, all surgeries were classified as CRPP or ORIF. CRPP was performed on 47 (81%) of the fractures, and open reduction was required on the remaining 11 (19%).
Eleven patients (19%) had a delay in treatment (a delay in definitive management more than 2 weeks from the injury). Five of these (45%) were due to a lack of recognition on the part of the initial provider, while six (55%) were due to a failure of the parents/guardians to bring the child in for evaluation, as seen in the new patient intake form. Of the 11 patients with delayed treatment, four required open reduction, a slightly higher percentage than the non-delayed group (36% vs 14%, p = 0.19; Table 2).
Outcomes associated with functional range of motion.
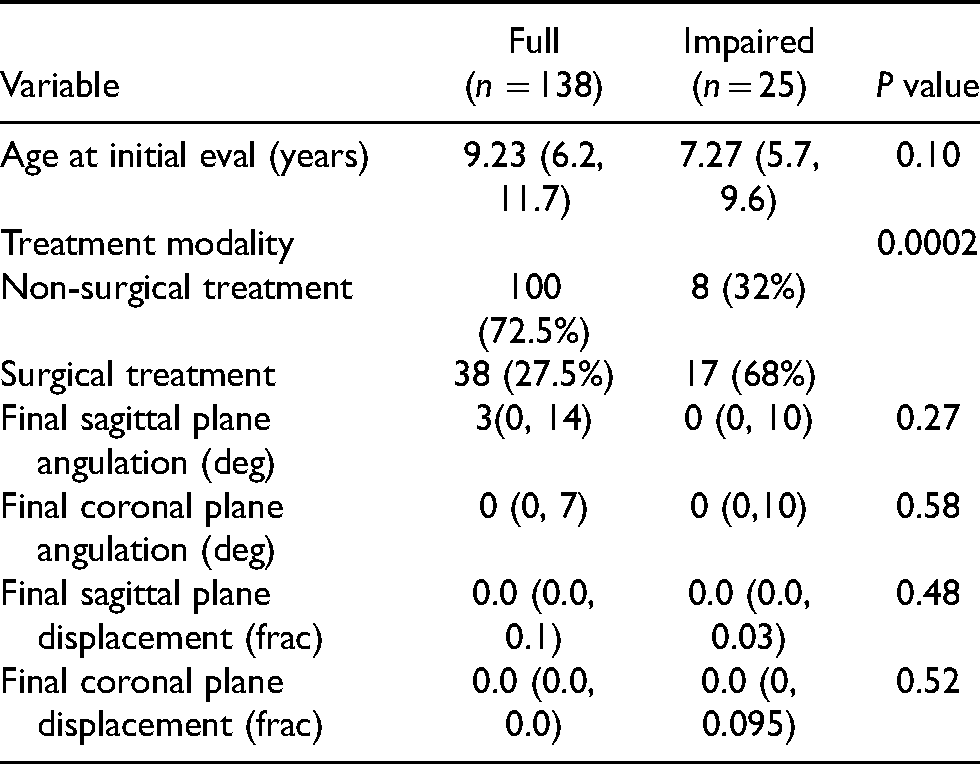
Twenty-five patients had limited range of motion on final follow-up exam (25/163, 15.3%). Compared to the rest of the patients, this group was more likely to have received surgery (68% vs 27.5%, p = 0.0002). Limited range of motion was classified as less than excellent or full range of motion. Some nonstandard limited range of motion documentation included but was not limited to “15 degree extension contracture,” “difficulty achieving full composite flexion,” “incomplete extension at final follow-up.” There was no significant association between limited final range of motion and initial displacement of the fracture (Table 3).
Within the surgical treatment group: Delay in treatment (> 14 days) association with type of surgical treatment.
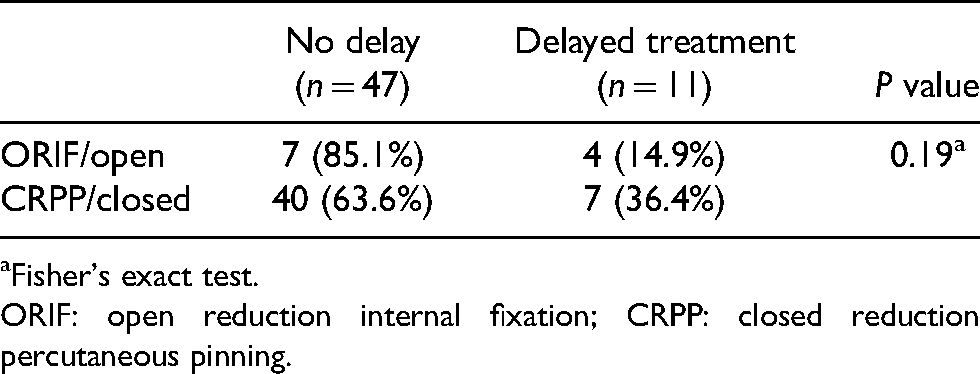
Fisher's exact test.
ORIF: open reduction internal fixation; CRPP: closed reduction percutaneous pinning.
There was one case of nonunion, which developed after noncompliance with immobilization. Given the significant delay in final surgical management of these patients, they were excluded from our statistical analysis for operative time to union. There were no incidences of hardware failure.
There were 23 patients with malrotation on initial presentation (23/174, 13.2%). Thirteen of twenty-three (56.5%) required surgery. Comparatively speaking it is a disproportionally higher amount than those patients without malrotation who required surgery only 29.8% of the time (p < 0.02; Table 4). Out of the 10 patients who presented with malrotation, eight healed in anatomic alignment with no rotational deformity and all eight patients received a closed reduction. One patient received splinting only with no reduction and the guardian and child were satisfied despite slight rotational deformity at final follow-up. The other patient presented 2.5 weeks after injury and chose splinting only as opposed to an osteotomy with ORIF. At final follow-up, the patient had a slight rotation with moderate angulation in a radial direction with minimal crossover at the fingertips. Within the surgically treated group, there was no significant association between presenting malrotation and the need for open reduction in the operating room. Closed reduction with percutaneous pinning was adequate to restore anatomic alignment. No cases of rotational deformity on final follow-up were observed although comments on this parameter were sometimes absent from the record.
Association of initial malrotation with treatment group.
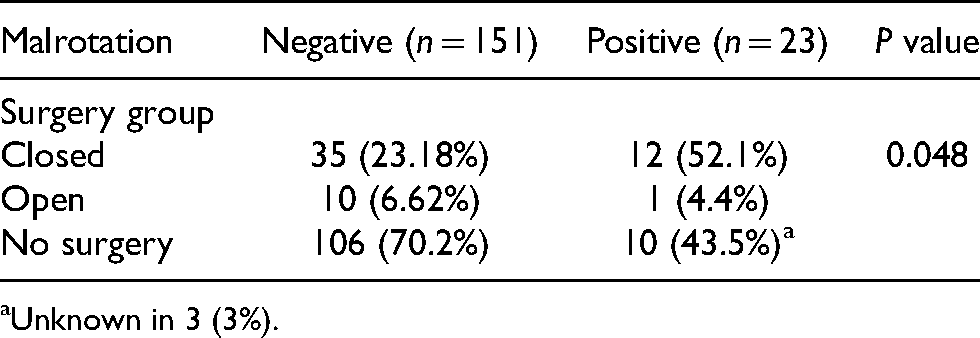
Unknown in 3 (3%).
Discussion
The aim of this study was to evaluate factors that influence treatment strategies of middle and proximal phalanx neck fractures. The instability and deformity associated with these injuries is often difficult to appreciate in the pediatric hand, due in part to swelling and the superfluous adipose in the subcutaneous tissue. Despite significant angulation and displacement, the pediatric finger can still clinically appear well aligned. The degree of displacement can be misjudged if necessary imaging such as a true lateral radiograph was not performed. Thus, inadequate reduction or other conservative treatment at the time of presentation can lead to reduced range of motion due to bony blocks or malunion, which requires surgery (osteotomy) months after the injury to correct the defect. 18 Education for guardians as well as providers may decrease the rate of delayed presentation and ultimately lead to less invasive treatment. Proximal phalangeal shaft fractures are treated by closed reduction with application of a short arm cast with the wrist held at 30 to 40 degrees extension and maintaining 70 degrees of metacarpophalangeal flexion.
An important finding of this study was that there is an increased time to union in the operative versus non-operative groups. We believe this to be in part due to the higher degree of initial displacement in the operative groups, predisposing these fractures to vascular disruption and delayed healing. Open reduction took on average 13 days longer to reach documented union suggesting that open reduction can produce additional vascular insult, though this difference was not statistically significant. This is consistent with prior literature, which has shown increased rates of avascular necrosis associated with open reduction. In a previous study reviewing the outcome of 23 patients with 24 phalangeal fractures showed that of the 13 cases that required open reduction all of them had poor functional results compared to closed reduction, and phalangeal head osteonecrosis was documented in four of these cases treated by open reduction.1,8,10
The degree of sagittal displacement on initial radiographs was strongly associated with the occurrence of surgery. Deforming forces often bring the distal fragment into extreme extension and can be missed on initial radiographs because it can be difficult to see in the anteroposterior (AP) view. Sagittal malalignment is considered by some to be a less important surgical indication than coronal displacement, because the former is more easily corrected by bony remodeling. 19 Others have observed that sagittal angulation can result in swan-neck deformity despite remodeling. 20 In our sample, sagittal malalignment was significantly associated with the need for surgery while coronal malalignment was not.
Our findings suggest that a delayed presentation raises significant challenges to the treating surgeon when surgical treatment is implemented. Evidence shows a slightly higher rate of open reduction (36%) that was necessary in surgically treated patients with delayed presentation as compared to the rest of the patients (14.9%; Table 3). The two factors that led to delayed presentation are the initial lack of recognition of the injury by the child's guardian, and the difficulty in viewing the fracture with an AP radiograph. Thus, some authors recommend the true lateral X-ray as part of the initial diagnosis to carefully examine the fracture and guide treatment. 12
Limited range of motion on final follow-up was more common in patients treated surgically than those treated with closed reduction only, a finding that is not surprising given the more severe nature of the fractures that required surgery with post-operative scarring. Patients with malrotation on physical exam were also more likely to require surgery than those without malrotation, which is also not surprising, given that this is a commonly used criterion for operative treatment for any fracture of metacarpals or phalanges. Initial malrotations in the non-operative group were generally resolved with closed reduction in the emergency department or clinic. In our study, mild malrotations remained among those did a not received a closed reduction. From previous studies it has been observed that in fractures of the neck of the phalanx, the distal fragment tends to go into malrotation due to the violent attempts of withdrawal from the patient. Moreover, the malrotated fragment can rotate up to 90° and most of these cases require open reduction or K-wire fixation to decrease the risk of malunion and non-union. 7
Strengths and limitations
Our study has several limitations given its retrospective design. First, almost half of the cases analyzed were excluded due to missing data or lack of patient follow-up, and analysis of the included records focused on radiographic examination due to missing parameters particularly range of motion. The interrater reliability may have skewed our measurements of initial displacement in radiographic evaluation. Clinical union as a time point in children has limitations given the variability of remodeling characteristics and age and scheduling appropriate follow-up appointments. Strengths include a large case cohort and robust statistical analysis.
Conclusion
It is imperative to evaluate a pediatric digital injury for sub-capital fracture of the proximal of middle phalanx. Clinical presentation can be deceiving with apparent normal clinical alignment and fusiform swelling of the digit which can be misdiagnosed as a “sprain.” Assessment of proper radiographic angles for these injuries and careful evaluation for sub-capital fracture are very important. Minimally displaced sub-capital fractures may be managed with immobilization, and a relatively short time to union may be expected. Patients presenting with sagittal angulation between 16–25 degrees and at least 10% displacement can be expected to have good outcomes with malrotation often resolved through non-operative closed reduction. A longer treatment course and time to union was associated with both open and closed forms of surgical treatment. In our sample, displacement of at least 30% in the sagittal plane was a potential indicator for surgical management. Proper education of treating physicians in the recognition and care of these fractures may lead to earlier treatment and less invasive options with more predictable outcomes.
Footnotes
Acknowledgments
We would like to thank Andy Lalka, MPH for project coordination and minor contributions to the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by NIH/NCRR Colorado CTSI Grant Number UL1 RR025780. Its contents are the authors’ sole responsibility and do not necessarily represent official NIH views.