
Abstract
While giant cell tumour of bone is a relatively common tumour in adults, it is exceedingly rare in children. Multicentric metachronous giant cell tumour is an even rarer presentation of this tumour in skeletally immature patients. We present here the challenges in management of this rare tumour.
A 12-year-old girl presented with a giant cell tumour affecting four different bones sequentially, three times within a 3-year period. The disease first appeared in the right distal fibula, then a year later in ipsilateral talus and calcaneus and finally a year later, in the T5 vertebral body, all requiring surgical treatment. Our strategy was to manage this lesion aggressively based on the limited literature available and present our own long-term surveillance strategy. Our patient responded well to treatment each time and has remained disease-free for 24 months from her last surgery.
This is a rare case of metachronous multicentric giant cell tumour of bone in a skeletally immature patient requiring aggressive treatment and surveillance.
Introduction
Giant cell tumour (GCT) of bone is a relatively common benign but locally aggressive bone tumour of adults, majority of whom are in the age group of 20–45 years. GCT by itself is an exceedingly rare tumour in the immature skeleton, with a reported incidence of 1.8% 1 and multicentricity of GCT in paediatric age group is very unusual. Multicentric GCT can be either synchronous (discovered at multiple sites at once or within 6 months of each other) or metachronous (the second tumour diagnosed more than 6 months after the first). 2 We report one such case of metachronous multicentric GCT of the bone in a 12-year-old girl involving distal fibula, followed by talus and calcaneum, and finally T5 vertebral body, each appearing after an interval of 12–15 months.
Case report
A 12-year-old girl presented with a progressive painful swelling over the lateral aspect of right ankle of 3 months duration, in January 2016. The swelling was firm to hard in consistency, localized to the lateral malleolus, and was causing some limitation of ankle dorsiflexion. Radiographs (Figure 1) showed an expansile osteolytic lesion involving the distal fibula epi-metaphysis with a thin shell of cortex and narrow zone of transition. MRI revealed a lesion that was hypointense on T1 and heterogeneous with a mild hyperintense signal on T2 weighted images (Figure 2). The lesion was reported to be a GCT of bone on percutaneous bone biopsy. As this was an unexpected finding in a child, the findings were discussed with the radiologist and the pathologist who acknowledged the unusual finding but affirmed that the histological findings were consistent with a diagnosis of GCT. Metabolic bone disease was ruled out by checking the serum calcium, phosphorous, alkaline phosphatase, and parathyroid hormone levels. As the tumour had significant thinning of the bone, the patient underwent wide excision of the lesion with a 15 mm margin of fibula proximally, followed by non-vascularized proximal fibular turn-down graft fixed with a one-third tubular plate and screws. Histopathological examination (HPE) of specimen revealed a giant cell containing tumour which had eroded the articular cartilage and insinuated onto its surface along with soft tissue extension. The tumour showed many multinucleated osteoclastic giant cells interspersed with mononuclear stromal cells. The mononuclear cells were oval to spindly with scattered mitoses (Figure 3). The diagnosis was confirmed to be GCT of bone after discussion in an MDT involving two experienced histopathologists, a radiologist and Orthopaedic surgeons.
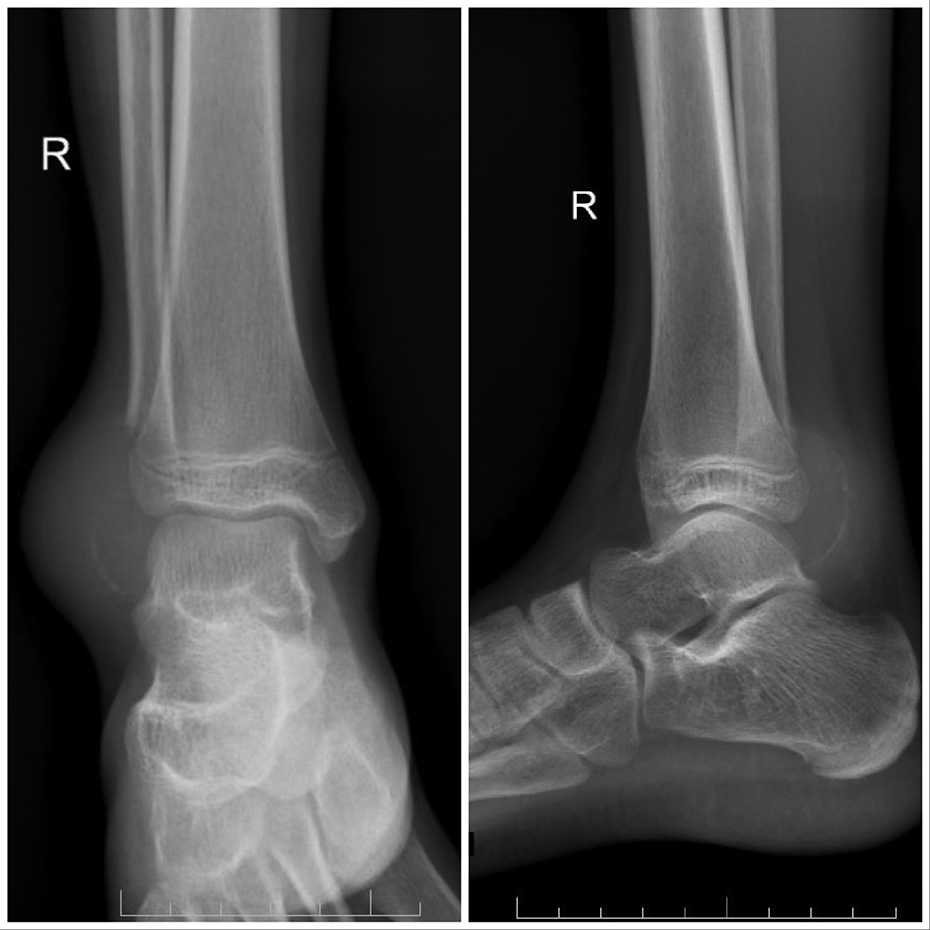
Anteroposterior and lateral radiograph of right ankle showing an expansile osteolytic lesion in the distal fibula with loss of the physis and narrow zone of transition proximally.
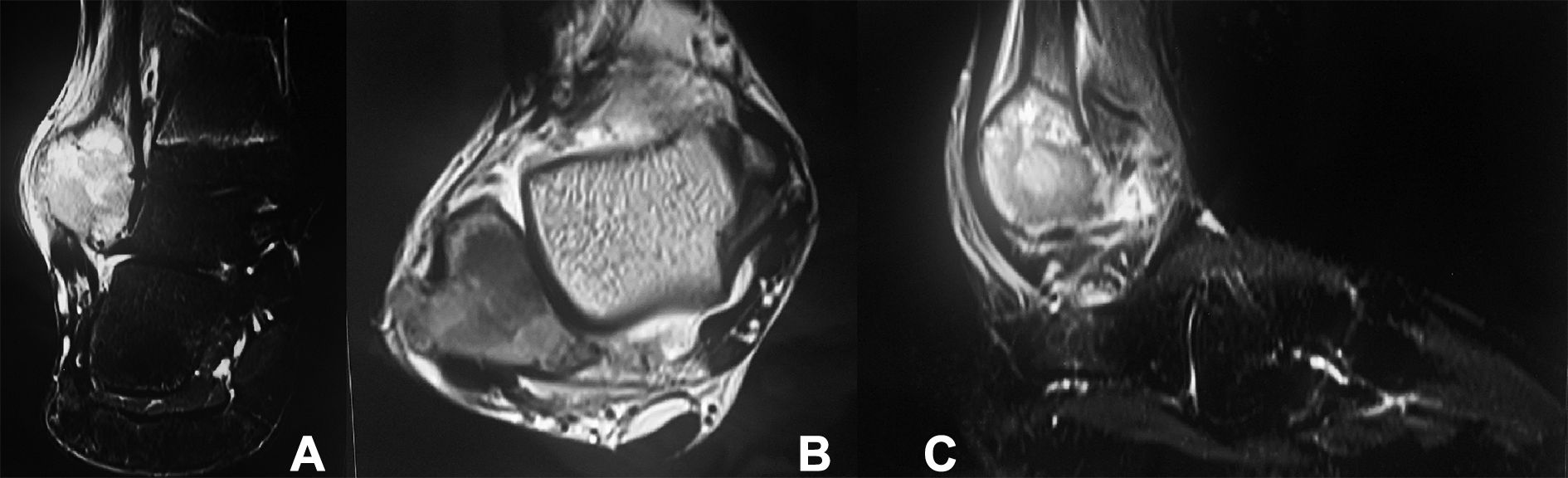
MRI of the right ankle showing a hyperintense lesion in right distal fibula on T2 weighted coronal (A), T1 weighted transverse (B) and T2 weighted sagittal (C) sections.
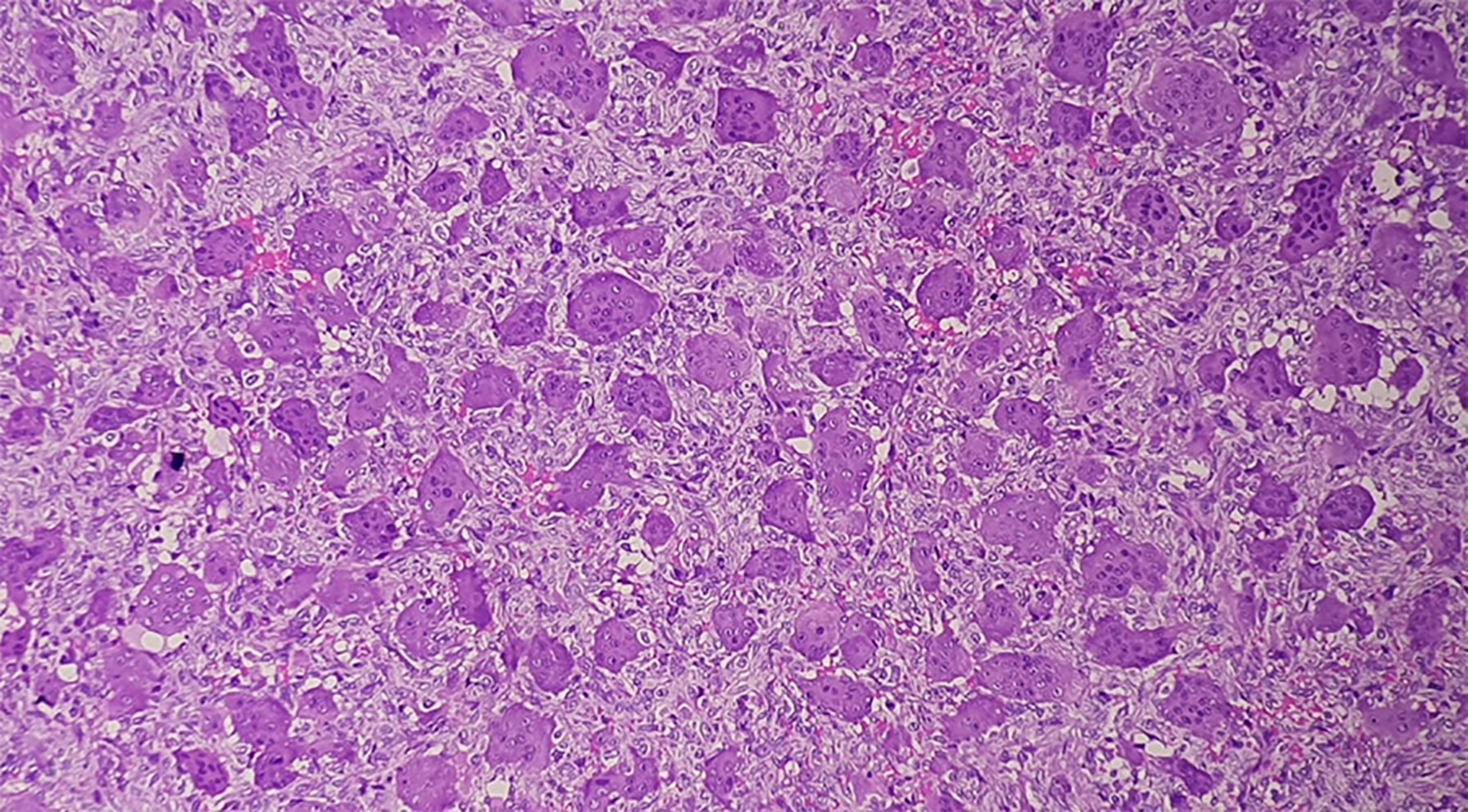
Photomicrograph (H&E – 10× magnification) of the excisional biopsy of the fibular lesion showing numerous multinucleated osteoclast like giant cells evenly distributed in sheets of stromal cells suggestive of giant cell tumour.
Three months after surgery, she presented with a progressively increasing soft tissue swelling over the posterior aspect of the grafted fibula, which was noted as local soft tissue recurrence on MRI (Figure 4). Because of the short duration, it was deduced that this was possibly a local residual tissue seeding resulting in recurrence and pointed towards the aggressive nature of the lesion. The soft tissue mass was excised en masse followed by local thermocoagulation.
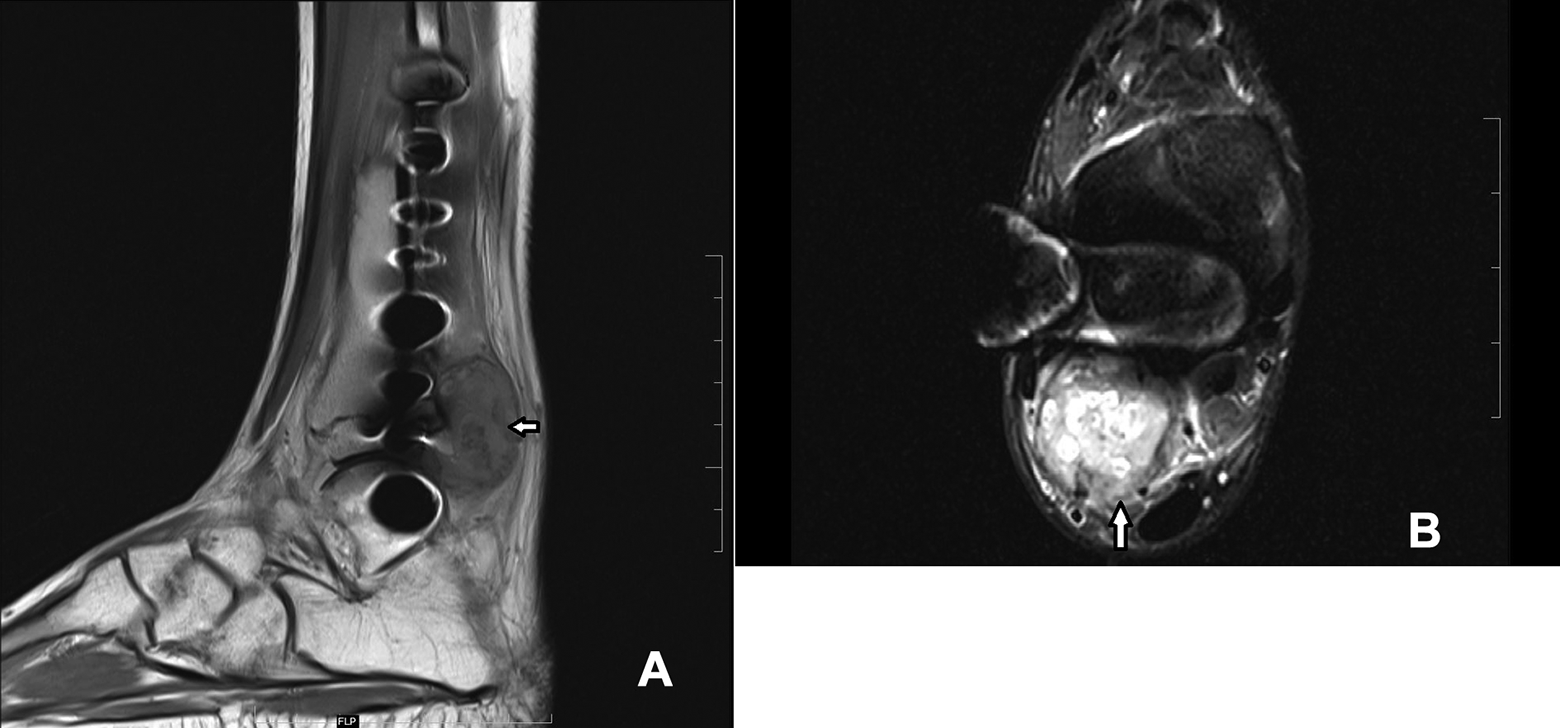
MRI scan of right ankle shows a recurrent soft tissue lesion in sagittal T1 weighted (A) and transverse PD fat suppressed (B) section posterior to the fibula (white arrow).
The patient remained symptom-free for a year after which she developed pain in the ipsilateral hindfoot. The radiographs showed a lytic, non-contiguous, non-expansile lesion in the talus and calcaneum with a lytic lesion at the osteosynthesis junction between the grafted fibula and the fibula stump left after resection of the primary tumour (Figure 5). This was confirmed on MRI to be of the same signal intensity as the previous lesion in fibula (Figure 6). A positron emission tomography (PET) CT scan showed that the disease was confined to the right foot only (Figure 7). A percutaneous biopsy of the calcaneal lesion again confirmed this to be a GCT of the bone. The patient underwent extended curettage and iliac crest bone grafting for the talus and calcaneum. For the fibular lesion, implant removal and segmental resection of the affected fibula was done, keeping the malleolar part of the reconstruction intact. HPE of the curettage specimen confirmed recurrence of GCT of bone with areas of reactive osteoid.

Anteroposterior and lateral radiograph of right ankle taken a year after index surgery shows recurrence of an osteolytic lesion in the fibula and in the talar head and neck as well as calcaneum (black arrows).

MRI of the right ankle and foot showing lesions with the same intensity as the previous MRI in the right talus, right calcaneum and right fibula.
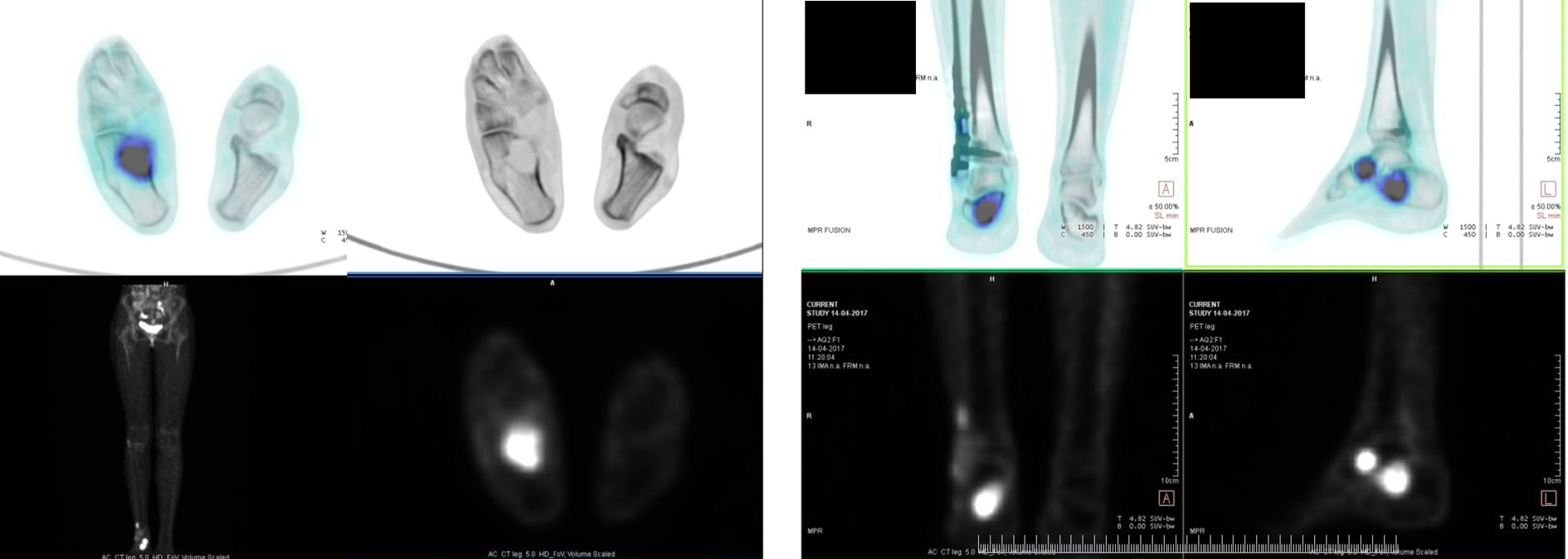
PET CT scan shows lesions localised to the right talus, calcaneum and fibula with no other skeletal lesions or pulmonary metastasis.
After a symptom-free period of another year, she presented with upper back pain without any neurological deficit of a few weeks’ duration. Imaging revealed a pathological fracture of T5 vertebral body with an epidural extension of the tumour compressing the spinal cord (Figure 8(A) and (B)). A transpedicular biopsy again revealed the same histology. A fresh PET-CT confirmed this to be an isolated lesion with no pulmonary metastases and with no recurrence in the previously operated areas. After 3 months of treatment with Denosumab, the tumour margins were reasonably ossified (Figure 8(D)) and the epidural tumour tissue had resolved (Figure 8(C)). The patient underwent a T5 en bloc resection (Figure 8(E) and (F)). Postoperative histopathological analysis revealed the margins to be tumour free. No residual giant cell tumour was seen in the specimen. The surrounding bone showed features of denosumab therapy. Denosumab was discontinued postoperatively and the patient monitored with weekly blood test for hypercalcemia for a month and then once a month for 3 more months. No rebound hypercalcemia was observed in our patient. PET scan was done at 1 year postoperatively and subsequently at 16 months thereafter (delayed due to COVID pandemic and lockdown). The patient remains tumour free and symptom free till date (30 months follow-up from last surgery) (Figure 9).
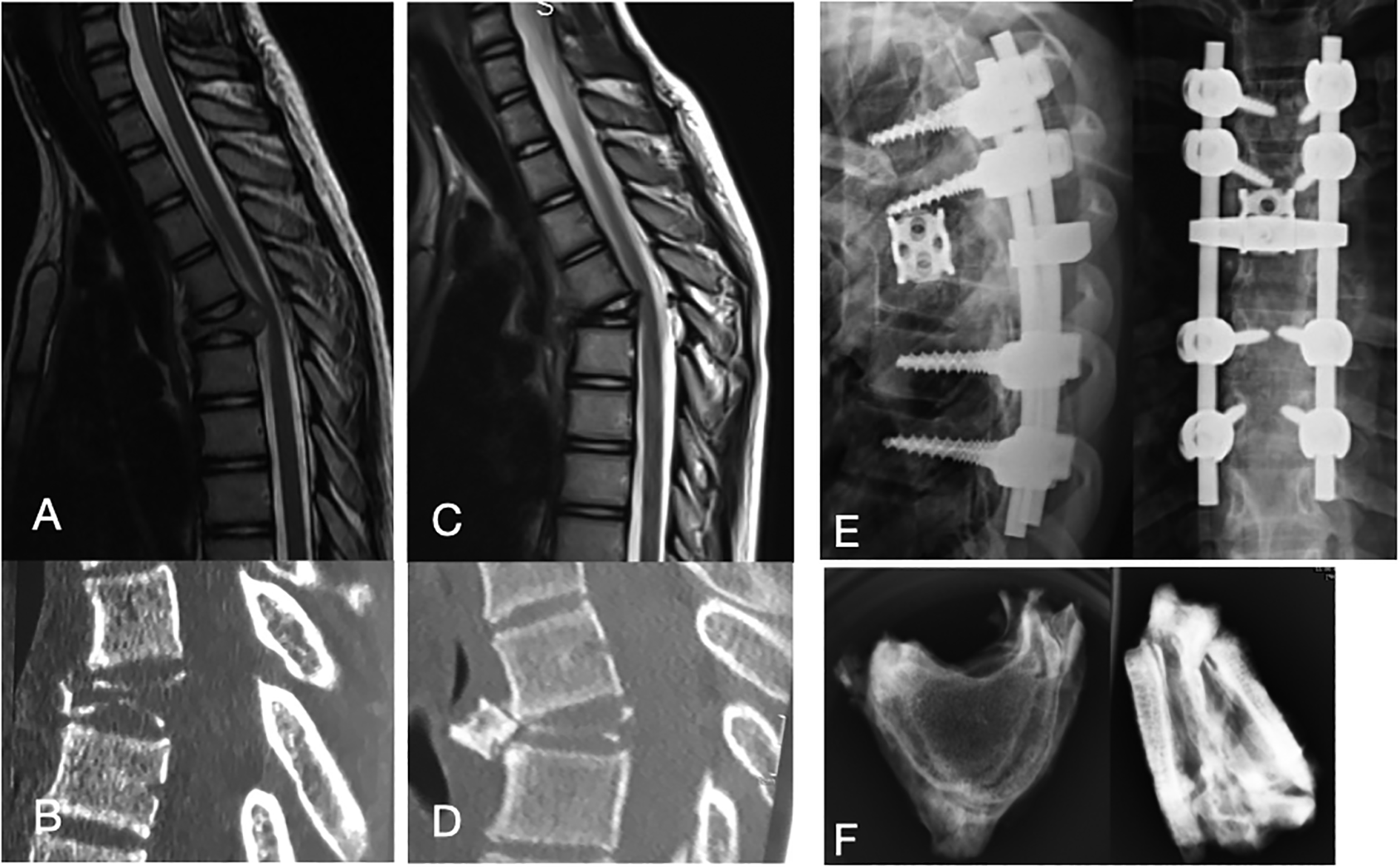
MRI (A) and CT (B) at presentation showing destruction of T5. MRI (C) and CT (D) 3 months after Denosumab showing ossification and resolution of epidural tumour. Radiographs (E) after T5 spondylectomy and reconstruction and in-vitro radiograph of excised vertebral body (F).

Radiograph of the right ankle at final follow-up shows good healing of all lesions with no valgus at the ankle.
Discussion
Multicentric GCT of bone has been described in adults but is exceedingly rare in children. Literature review revealed 10 cases of metachronous multicentric GCT of bone in children, 3 –7 ranging in age from 10 to 16 years, male to female ratio of 3:7 and involving 2–10 sites over a span of 1–15 years (Table 1). In most reports, the second lesion was more aggressive than the first, recurrence was common, and curettage was ineffective as treatment with majority requiring wide resection and reconstruction.
Comparative data from literature for previously reported metachronous multicentric GCT of bone.
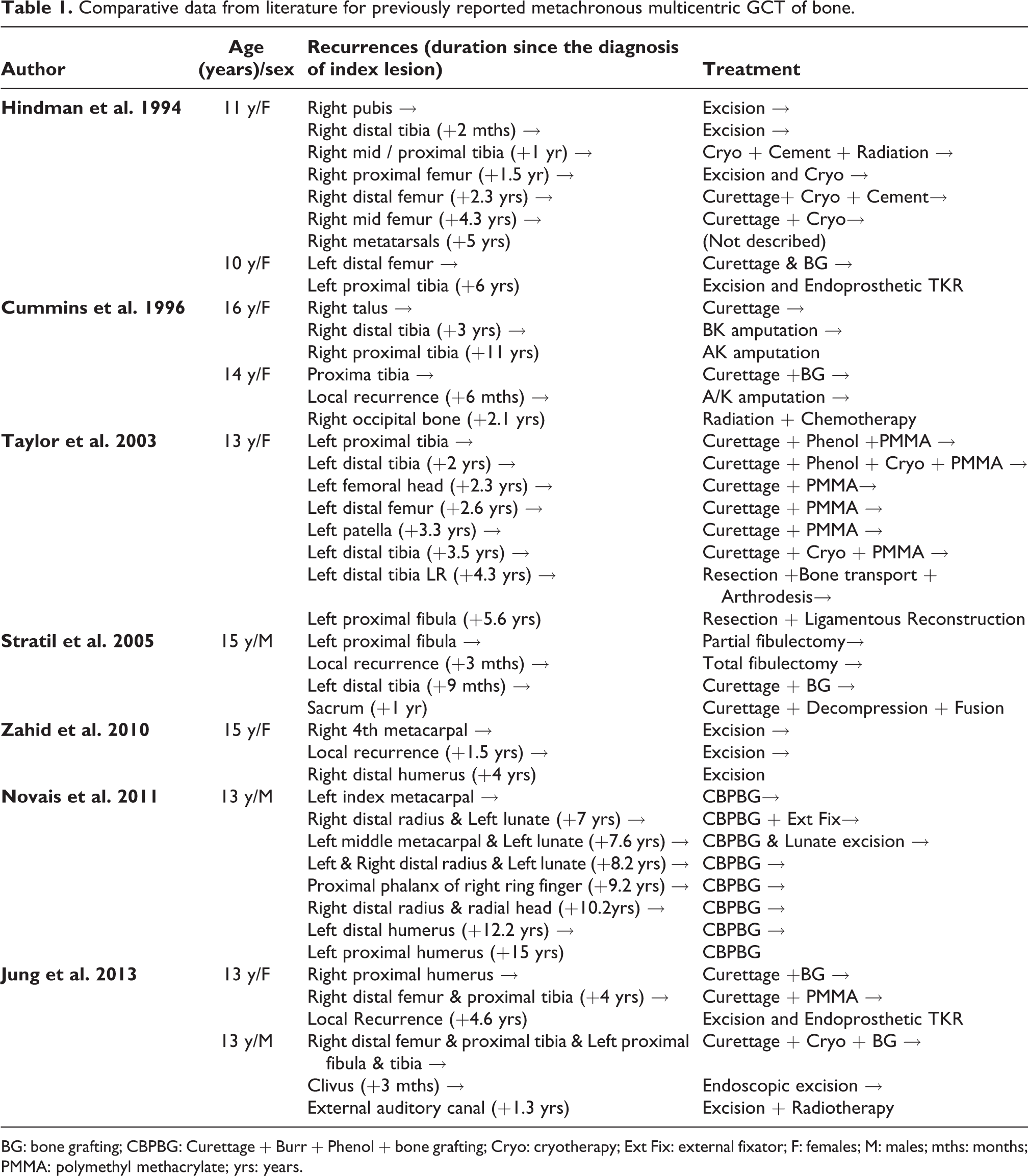
BG: bone grafting; CBPBG: Curettage + Burr + Phenol + bone grafting; Cryo: cryotherapy; Ext Fix: external fixator; F: females; M: males; mths: months; PMMA: polymethyl methacrylate; yrs: years.
Metachronous GCT may represent metastatic GCT onto a remote bone from a primary focus or de novo development of lesion and do not necessarily imply malignant transformation. Pathogenesis is unknown and there seems to be no way of defining the mechanism radiologically or histologically. The histology of multicentric GCTs is indistinguishable from solitary GCT. Additional secondary changes like fibrohistiocytic areas, reactive bone formation, or aneurysmal bone-cyst like changes can be seen in both. In our patient, histopathology was classical of GCT with some secondary changes in all the four metachronous sites. Ki-67 proliferation index in metachronous lesion has been reported to be similar for each metachronous new location, but the index is increased in case of a local recurrence. This suggests that the appearance of GCT at a new location does not seem to be related to an increase in its aggressiveness. 8 In our patient, Ki-67 proliferation index was in the range of 5–8% in the various metachronous lesions. The recurrent tumour in fibula showed a Ki 67 index of 10% whereas the primary lesion in fibula showed an index of 8%.
Hoch et al. 2 have reported on the largest retrospective series of multicentric GCT in 30 patients (94 lesions), frequently presenting as a synchronous lesion around the knee. In their series, metachronous tumours were identified in 63% of patients, with an average time of 5.8 years between the appearance of the second lesion after index case. Local recurrence was reported to be 26%. 2
Pre-treatment with denosumab in spinal lesions is recommended not only because the ossification of the tumour margins makes the tumour handling easier and safer for en bloc resection, but also it has been shown to reduce local recurrence rate. 9 In contrast, Denosumab has been shown to increase the chance of leaving residual tumour behind in intralesional surgeries, Hence, it was not used in previous surgeries around the ankle. 10,11 It was tempting for us to consider continuing denosumab therapy after the third instance of the tumour with the hope that subsequent recurrences would be prevented. However, there is no evidence to suggest that denosumab can prevent future lesions in metachronous GCT. 10,11
The optimum strategy for surveillance of children with metachronous GCT is a challenge. We can only speculate whether an early diagnosis on screening before the lesion becomes symptomatic can alter the prognosis or the extent of surgery. This also must be balanced with the risk of exposing the child to hazards of radiation due to repeated imaging. Dhillon et al. 12 in their review of multicentric GCT recommend half-yearly screenings with bone scan or skeletal survey for up to 5 years in ‘high-risk group’ which they classified as young age, females, GCT at unusual sites such as hands and feet, and those with initial synchronous multicentric lesions. We have derived our own strategy for 6 monthly clinical follow-up and annual PET CT screening for our patient for up to 5 years from the last lesion. We chose PET CT over a bone scan in our patient as it is better at defining anatomical characteristics of the lesions in addition to the metabolic activity which makes it easy to understand the bone health and risk of fracture. PET CT can also pick up pulmonary metastasis in addition to bony lesions.
We conclude that GCT in a child needs a low threshold for aggressive treatment and a meticulous follow-up protocol due to a higher probability for multicentricity based on our case and those reported in literature. Once diagnosed as metachronous and multicentric, patient requires a potentially long-term surveillance at least annually for up to 5 years after the last lesion.
Footnotes
Availability of data
All data presented in this study including images, are available upon request.
Consent for publication
The patient’s parents have given their written consent for publication of the case including the images, in an anonymised manner.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent
The Hospital Ethics committee approved the case for publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.