
Abstract
Diabetes mellitus effects around 10% of the whole population and unhealed diabetic foot ulcer is one of the most debilitating and economically burdensome conditions. This condition is commonly seen by different specialists including physicians, orthopaedic surgeons and vascular surgeons. We present a case of unhealed diabetic foot ulcer which has been treated in our Hyperbaric Oxygen Therapy (HBOT) centre. We also review the literature with respect to management strategy and rationale of hyperbaric oxygen therapy for diabetic foot ulcers.
Introduction
The use of hyperbaric oxygen therapy for the treatment of selected diabetic problem wounds has been receiving much attention in recent years. Historically, Jacques-Yves Cousteau’s divers were working 35 feet below the surface of the Red Sea and claimed that their wounds healed significantly faster when they lived in an underwater environment. In 1964, Hunt et al. investigated this phenomenon and provided the scientific evidence and rationale that wound healing is dependent on tissue oxygenation. 1
The first hospital-based Hyperbaric Oxygen Therapy (HBOT) Centre was established in September 2018 and offers treatment for different emergency and elective treatments in Hong Kong. Indications for elective treatments included chronic unhealed wounds, delayed radiation injuries and idiopathic sensorineural hearing loss. In this article, we present a case of chronic unhealed wounds and review the literature on the effects of hyperbaric oxygen treatment.
Case report
A 62-year-old male hepatitis B carrier with a past medical history of diabetes mellitus who was on self-administered insulin therapy, for 20 years, suffered from a chronic non-healing wound on the lateral side of his right foot for 1.5 years. He was treated with wound dressings and occasional antibiotics by out-patient clinics. He was once admitted to the orthopedics ward in May 2019 due to wound infection and right lower limb cellulitis. His unhealed wound increased in size and the amount of discharge. He was then treated with Augmentin and discharged. However, he was admitted again 2 days later due to an increased darkening of skin surrounding the wound. The patient suffered from increased foot pain and difficulty in walking.
X-rays of the right foot showed Osteomyelitis with osteomyelitic changes over the right fifth metatarsal and the base of the proximal phalange of the fifth toe (Figure 1). An emergency operation was performed the next day with excisional debridement of the wound. The Orthopaedic surgeon also considered ray amputation with or without below knee amputation. However, the patient refused. A CT Angiogram was performed for both lower limbs and showed the right anterior tibial artery was limited by its small caliber. Some segments were not well opacified and stenosis had to be considered. The left anterior tibial artery showed mild stenosis over the distal segments. The patient had had angioplasty performed in June 2019 but the right anterior tibial artery and the dorsalis pedis artery had failed to recannulise. Thus, the patient could only be treated with daily dressing of the wound.

Osteomyelitic changes over the right fifth metatarsal and the base of the proximal phalange of the fifth toe.
The patient was then referred to our HBOT Centre for assessment and treatment. On the first day of assessment, transcutaneous oximetry monitoring (TCOM) was performed on the patient’s wound (Figure 2). The result showed that the patient had critical hypoxia around the wound with values of less than 20 mmHg shown in Table 1, and oxygenation had greatly improved to more than 100 mmHg after breathing 100% oxygen. This suggested that the patient is indicative for HBOT treatment. A total of 40 sessions of HBOT with maximum 2.4 ATA and 90 min of oxygen time each session were provided to the patient. Subsequent TCOMs were performed and showed normalised results of average values more than 30 mmHg with optimal oxygenation around the wound (Table 1). HBOT was stopped on Day 64 after the start of treatment due to greatly improving wound condition and the wound oxygenation was normalised. Continuous daily dressing was done in the general out-patient clinic. The wound was totally healed 2 months after the completion of the HBOT (Figure 3(a) to (g) show the progress of wound healing during HBOT treatment). The patient recovered with a well healed wound, no callosity and pain in subsequent orthopedics follow-up.

TCOM assessment of wound.
TCOM assessment results.
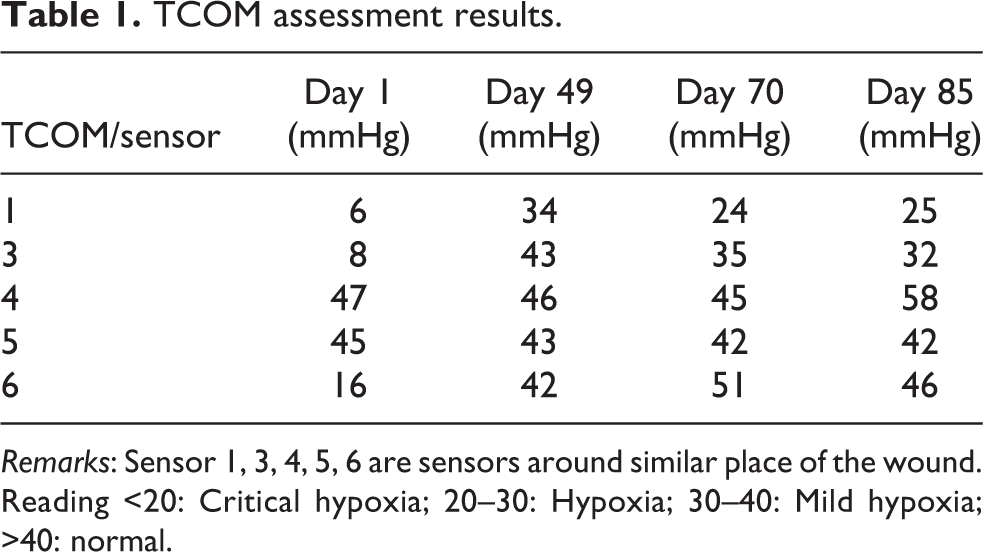
Remarks: Sensor 1, 3, 4, 5, 6 are sensors around similar place of the wound. Reading <20: Critical hypoxia; 20–30: Hypoxia; 30–40: Mild hypoxia; >40: normal.
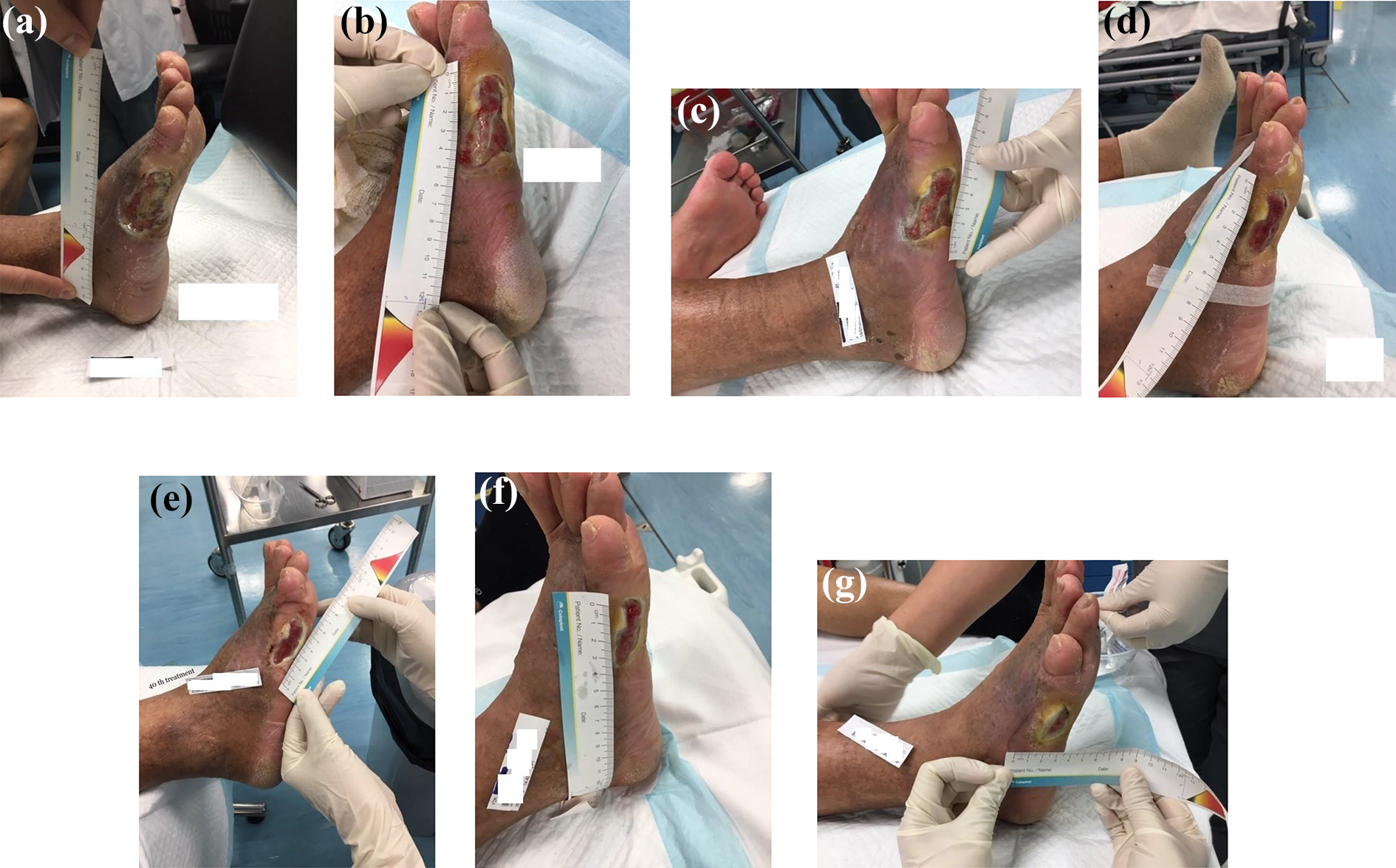
(a) Wound status day 1 of treatment. (b) Wound status day 18. (c) Wound status day 32. (d) Wound status day 49. (e) Wound status day 65. (f) Wound status day 70. (g) Wound status day 85.
Discussion
Unhealed chronic diabetic foot ulcer (DFU) with recurrent infection is a common complication in long standing diabetic patients. Thirteen percent of diabetic patients will have one or more episodes of diabetic foot ulcer, 59% of the DFU patients will have a recurrence over the next 5 years. 2 –4 The occurrence of DFU is considered distressing to the health related quality of life due to the negative impact to both physical and psychosocial aspects of the patients and their care givers. Enormous healthcare cost is needed to manage DFU and diabetic related lower extremity amputation. 5
Troublesome triad of diabetic foot, pathophysiology of DFU
Three problems are always contributing to the development of chronic DFU, they are deformity, deep infection and ischaemia–hypoxia. This troublesome triad, together with an indirect contributor, neuropathy, often delays the patient seeking care for his condition. 6 Deformities in the lower extremity develop ulcers with analogous biomechanical abnormalities. Shear stresses tangential to the skin surface in conjunction with deformities and bony prominences are prone to ulcer formation. Oxygen is need in many cellular processes from collagen deposition to anti-microbial activities. Oxygen-sensitive processes, including fibroblast replication, collagen deposition and angiogenesis, are all essential to wound healing. 7 –9 Efficient phagocyte bacteria killing requires a local partial oxygen pressure of 30 mmHg or above. 10 Neutrophils has a 70% killing rate of bacteria in a tissue oxygen tension 30 mmHg whereas it drops to 37% when there is no oxygen. 11 Early antibiotics administration, together with hyperoxia, results in more efficient bacterial clearance. 12
Strategies in management of diabetic foot wound
The first important strategy in successful management of the DFU is to properly manage the wound bed. Debridement is the hallmark of management which included sharp debridement, autologous debridement, enzymatic debridement, pulsatile lavage debridement and biological debridement. Firstly, it is important to correct the deformities by osteotomy, ostectomy or tenotomy. For dead tissue, proper removal is needed. Secondly, the wound should be protected and stabilised by well-padded soft dressings, splints, removable walkers or fixations etc. This provides the best possible conditions for the wound to heal. Thirdly, optimal medical management is needed in terms of good diabetic control with optimised glucose and HbA1c levels. Cardiac, renal and nutritional statuses are also important for wound healing. Fourthly, It is important to select an optimal wound dressing agent. There are thousands of dressing agents and it is depends on the stage of the ulcer, the infectivity and the amount of secretion. Lastly, it comes to the next section of the discussion, wound perfusion and oxygenation of the wound. 13
Patient selection
For effective and efficient use of HBOT, patient selection is crucial. The best practice to treat DFU would be a detailed assessment with vascular team involvement to see if intervention is necessary, removal of neuropathic ulcers, infection control, medical condition optimisation and surgical debridement of devitalised tissue. HBOT should be combined with these measures especially for those reversible hypoxic wounds. HBOT should not be delayed if there is still a chance to ameliorate the effects of hypoxia in the ischaemic penumbra.
Diabetic patients with an acutely infected Wagner grade 3 DFU requiring surgical intervention should be treated with HBOT urgently if there is a concern of tissue hypoxia. Tissue hypoxia increases in the first 3–4 days following surgery and HBOT can hyper-oxygenate the compromised tissue in the postoperative phase. For chronic unhealed wounds more than 30 days old despite optimisation of medical and surgical conditions, Wagner Grade 3 DFU suggests treatment by HBOT according to the UHMS Clinical Practice Guideline. 14 In our case, the patient has a chronic diabetic ulcer despite optimisation of the infection and dressing condition with appropriate vascular assessment. There is no further vascular or surgical intervention can be performed. Hyperbaric oxygen becomes his final hope.
Transcutaneous oximetry (TCOM)
TCOM measures the tissue oxygen level or tissue oxygen tension in mmHg. It approximates arterial capillary partial pressure of oxygen. The normal value ranges from 40 to 90 mmHg depending on body area measured. It can be used for screening for vessel disease, identifying healing potential, selection of amputation level, selection of hyperbaric suitable patients and monitoring of ventilated hyperbaric patients. It is good predictor for healing failure as hypoxic tissue does not spontaneously heal. But whether a wound can be healed successfully depends on other factors such as infection and nutrition. A pre-treatment TCOM is important because if the peri-wound bed TCOM values shows hypoxia or critical hypoxia (values < 20 mmHg), it indicates that hypoxia is one of the reason for chronic wound condition. Oxygen challenge test will be done for the patient with TCOM measurement again, if the values grossly improve with greater than 100 mmHg, it indicates that the hypoxic wound condition will likely response to hyperbaric oxygen therapy.
Rationale for HBOT
HBOT aids wound healing especially for ischaemic and hypoxic wounds. An increase in the oxygen diffusion gradient enhances diffusion of oxygen to ischaemic tissue beds. It provides sufficient oxygen for the wound. Oxygen diffusion at the tissue level varies in direct linear relationship to the increased partial pressure of oxygen. 15 HBOT can also ameliorate the ischaemia–reperfusion injury, stimulate circulating stem progenitor cells, augment neutrophil bacterial killing activity and produce reactive oxygen and nitrogen species. HBOT demonstrates its role in stimulating angiogenesis through recruitment and differentiation of circulating stem progenitor cells to form vessels. 16 HBOT has also been shown to increase synthesis of many growth factors including the vascular endothelial growth factor (VEGF), platelet-derived growth factors (PDGF) etc. 17,18 HBOT is reported to accelerate epithelialisation by about 30%. 19
HBOT directly corrects the pathophysiology of DFU by reversing the hypoxia caused by diabetes mellitus and stimulating different growth factors as stated above. There have been different studies from 1979 to now. A randomised control trial in 1996 showed that HBOT reduces major amputation from 33% to 9% and an improvement of tissue oxygenation as measured by TCOM was noted. 20 In 2003, Kessler et al. suggested that the HBOT group had a significantly larger reduction in wound size than the control group (41.8% vs 21.7%) at the time of discharge. 21 In 2010, Londahl performed a randomised double-blind sham-controlled trial in which he showed the one-year healing rate based on intention-to-treat analysis was significantly higher in the HBOT group (52% vs 29%) and was even higher when using per-protocol analysis for patients that received more than 35 treatments (61% vs 27%). 22
Conclusion
This is the first experience of treating a chronic DFU patient with hyperbaric oxygen therapy in a Hong Kong public hospital. It was successful because the patient was treated according to international guidelines. Moreover, the patient was well selected with the assistance of TCOM which can indicate whether the hypoxic wound is reversible or not. Further experience with long-term follow-up and assessment is needed for long-term efficacy of HBOT treatment for chronic DFU. It is worthwhile to promote this treatment to all chronic DFU patients in terms of promising a short-term positive outcome.
Footnotes
Consent
The patient was treated in accordance with the Declaration of Helsinki, the patient provided informed consent for the treatment/procedures, and patient provided consent for publication verbally.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.