
Abstract
Background:
Pelvic ring and acetabular fractures are some of the most morbid in orthopedic trauma. They commonly require large exposures for fixation and are associated with significant morbidity and mortality. This study attempts to identify risk factors for complications following operative fixation of pelvic injuries.
Methods:
126 patients treated for pelvic injuries were reviewed retrospectively. Demographics, procedure characteristics, and outcomes were recorded. Variables associated with complications were analyzed using logistic regression analysis.
Results:
Complications occurred in 12 patients. Higher BMI, longer length of stay, and ilioinguinal approach were significantly associated with increased infection risk. Co-morbid heart disease and concurrent smoking status showed a trend for increased infection risk. Higher BMI and ilioinguinal approach were significantly associated with an increased likelihood of re-operation. Positive psychiatric history and Medicaid payer status showed a trend toward higher reoperation risk.
Conclusion:
Knowledge of these risk factors can help guide management and predict outcomes following pelvic fracture fixation.
Introduction
Operative pelvic ring and acetabular fractures are relatively rare injuries, accounting for about 7–10% of all pelvic fractures. 1 Operative pelvic fractures often result from high energy mechanisms and thus, are some of the most morbid injuries in orthopedic trauma. Patients with pelvic and acetabular fractures often present with concomitant injuries including head injuries in 16–22%, abdominal injuries in 8–28%, thoracic injuries in 10–21%, genitourinary injuries in 3–22%, limb injuries in 35–41%, and spinal injuries in 2–4% of patients. 2 –4 Furthermore, post-operative complications following fixation of pelvic fractures can lead to devastating complications. Few studies have attempted to identify risk factors for complications following surgical stabilization of pelvic ring or acetabular fractures. Knowledge of such risk factors can help aid physicians in counseling these patients about their respective perioperative risks and guide appropriate management of pelvic and acetabular fractures, especially in high risk patients.
This study attempts to enhance current literature regarding risk factors for complications following operative fixation of pelvic and acetabular fractures. We hypothesize that elevated body mass index (BMI) and more invasive surgical approaches will increase the risk of complications in this patient population.
Methods
Patients were identified via Current Procedural Terminology (CPT) codes for operative fixation of pelvic and/or acetabular fractures and cross referenced to their electronic medical record. Procedures of interest include percutaneous cannulated screw fixation and open reduction internal fixation (ORIF) of all pelvic ring and acetabular injuries. Medical records were retrospectively reviewed and data was extracted via comprehensive chart review. Patients treated from 2012 to 2018 at our urban level 1 trauma center were included.
Demographic variables including age, race, smoking status, body mass index (BMI), medical co-morbidities, psychiatric history, substance use, injury mechanism, Medicaid insurance payer, diabetes, human immunodeficiency virus (HIV), chronic obstructive pulmonary disease (COPD), and cardiac history were collected. All patient records were checked at least 1 year postoperatively to assess for most recent follow up status. In addition, mechanism of injury, operative approach, infection, malunion, nonunion, hardware failure and reoperation rates were collected. Reoperation was due to premature implant failure, nonunion, malunion, as well as infection. Infection was also analyzed independently of other sources of reoperation. Complications were based on treating surgeon determination as recorded in the medical record. Length of stay was defined as total length of stay from admission to discharge.
A post hoc power analysis with alpha of .05 and a desired statistical power of 0.80 revealed that the sample size required for adequate statistical power for this study was 926 for small effects, 135 for moderate effects, and 66 for large effects. Demographic variables are represented as mean, percentage and standard deviation where appropriate. Multiple logistic regression analysis was used to identify variables predictive of infection and reoperation using backward stepwise elimination. Age and length of stay were entered into the regression as continuous variables, whereas BMI was entered as a binary variable with cutoff of >30. Data analysis was performed using SAS statistical software (SAS Institute Inc. Cary, NC).
Results
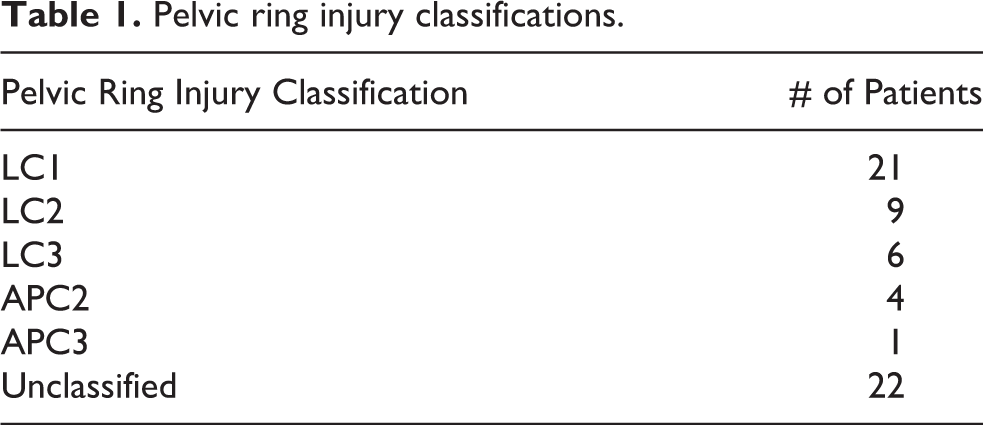
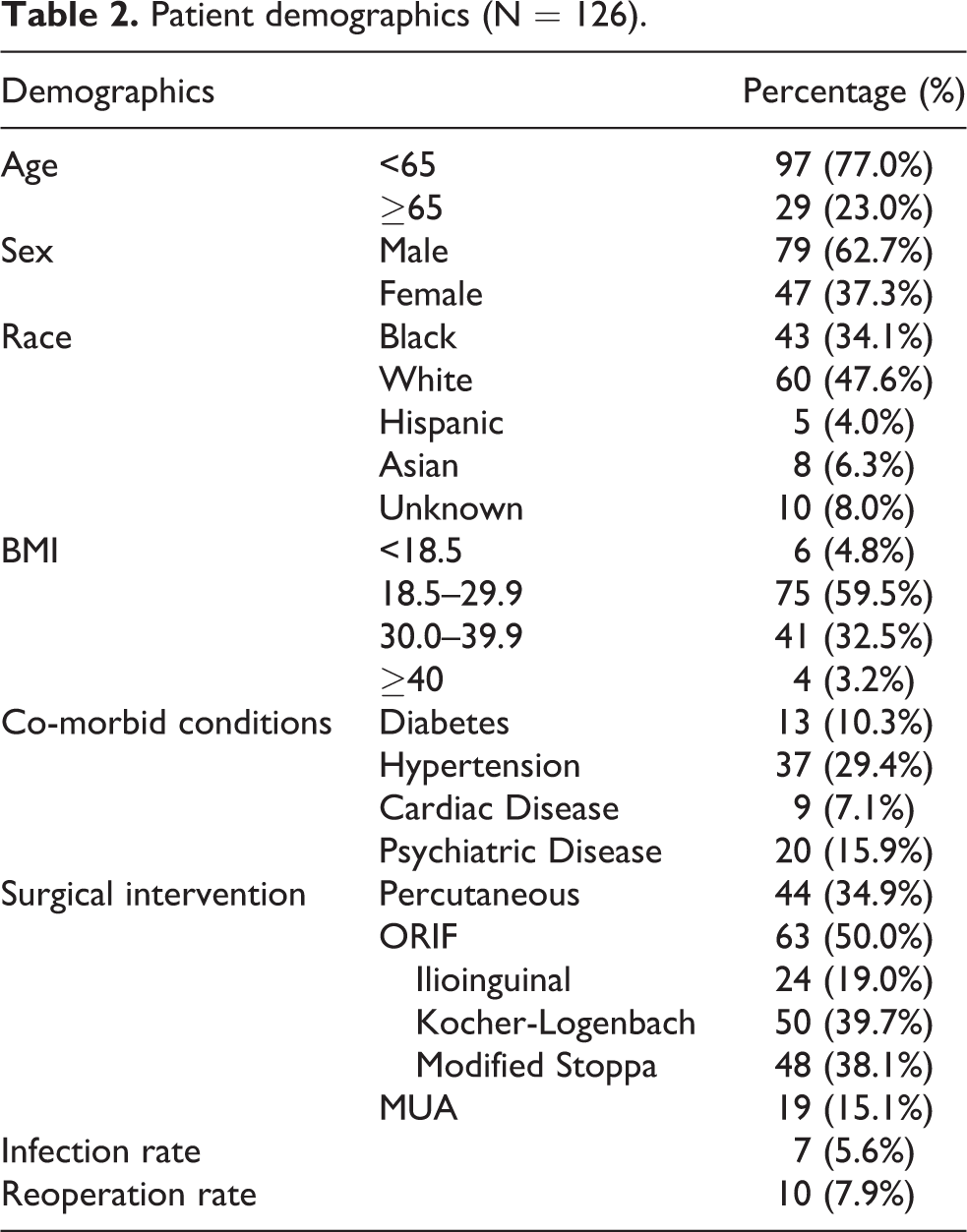
One hundred thirty-one patients aged 11 to 94 undergoing surgical fixation of pelvic and/or acetabular fractures between the years 2012 and 2018 were identified. Five patients had incomplete data and were excluded from further analysis. Of those included, 63 were treated for an acetabular fracture (50%), 40 for a pelvic ring injury (31.7%), and 23 for concurrent acetabular and pelvic ring injury (19.3%). Pelvic ring injuries were further classified (Table 1). Patient demographics are outlined in Table 2. The average patient age was 45.7 ± 16.85 years and 62.7% were male. The average BMI of our sample was 28.7 ± 6.87 and 63 underwent ORIF. Average time from operation to most recent follow up was 8.5 ± 12 months.
Pelvic ring injury classifications.
Patient demographics (N = 126).
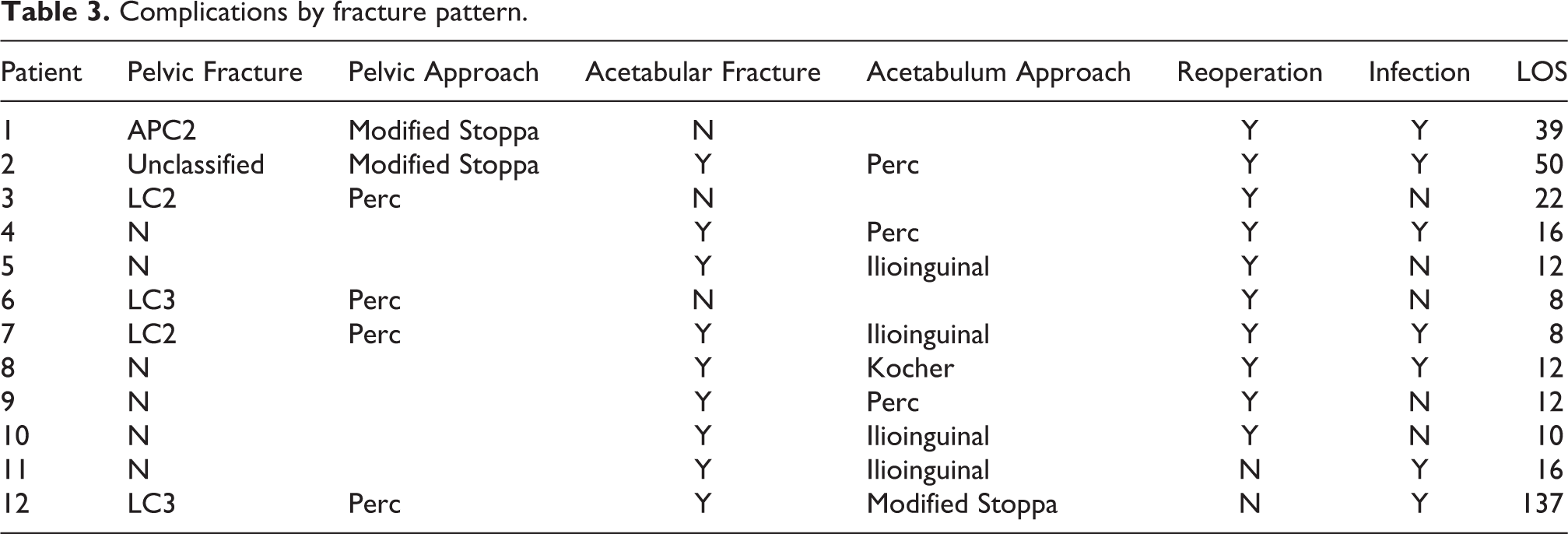
Complications requiring additional unexpected management postoperatively occurred in 12 patients (9.5%). Reoperation was performed for either malunion, nonunion, or premature failure of instrumentation in 10 cases (7.9%). Management of surgical site infection was necessary in 7 cases (5.6%). Specific complications by fracture pattern are presented in Table 3. The infection rate for BMI ≥ 30 was 11.1% (5/45) and for BMI <30 was 2.4% (2/81). Isolated pelvic ring injuries had an infection rate of 2.7% (1/37), acetabular fractures of 4.8% (3/63), and concurrent pelvic ring and acetabular fracture of 13% (3/23). In regards to specific approaches, the infection rate for ilioinguinal approach was 16.6% (2/12), Modified Stoppa was 13% (3/23), Kocher-Langenboch was 4.2% (1/24), and percutaneous fixation was 4.2% (1/24). The reoperation rate for BMI ≥ 30 was 13.3% (6/45) and for BMI <30 was 4.9% (4/81). Isolated pelvic ring injuries had a reoperation rate of 8.1% (3/37), acetabular fractures of 7.9% (5/63), and concurrent pelvic ring and acetabular fracture of 8.7% (2/23). In regards to specific approaches, the reoperation rate for ilioinguinal approach was 25% (3/12), Modified Stoppa was 8.7% (2/23), Kocher-Langenboch was 4.2% (1/24), and percutaneous fixation was 16.6% (4/24).
Complications by fracture pattern.
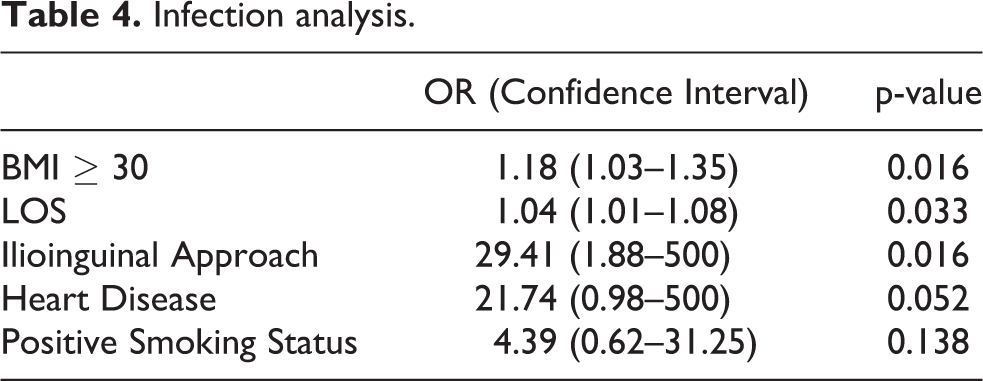
Multiple factors were associated with increased rates of infection after surgical fixation of pelvic fractures (Table 4). Higher BMI (OR 1.18, CI 1.03–1.35, p = 0.016) and longer length of stay (OR 1.04, CI 1.01–1.08, p = 0.033) were independently associated with higher rates of infection postoperatively. In addition, percutaneous screw fixation, Kocher-Logenbach approach, and modified Stoppa approach were associated with lower infection risks compared to ilioinguinal approach (OR 29.41, CI 1.88–500, p = 0.016). Co-morbid heart disease (p = 0.052) and concurrent smoking status (p = 0.138) showed a trend toward increased infection risk but was not statistically significant.
Infection analysis.
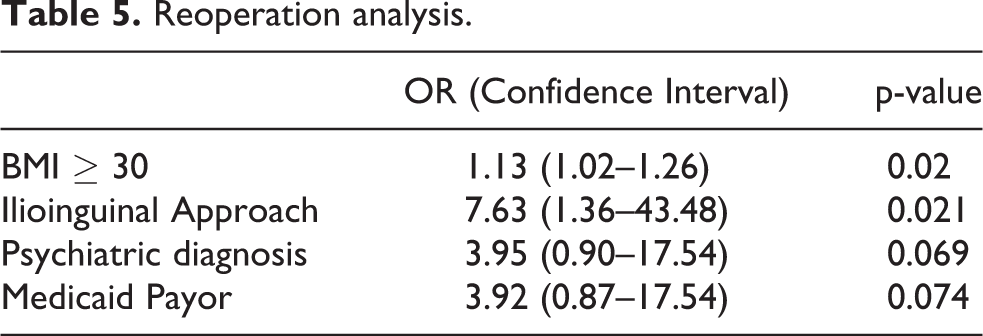
Numerous factors were associated with rates of reoperation (Table 5). BMI > 30 was associated with an increased likelihood of re-operation (OR 1.13, CI 1.02–1.26, p = 0.02). Similarly, ilioinguinal approach was associated with increased reoperation risk compared to other approaches (OR 7.63, CI 1.36–43.48, p = .021). There was a nonsignificant trend for subjects with a documented psychiatric history (p = 0.069) and for those with Medicaid payer status (p = 0.074).
Reoperation analysis.
Discussion
Current literature is mixed regarding variables that increase risk of complications following operative management of pelvic fractures. Several studies have shown increased BMI to negatively influence outcomes after pelvic and acetabular fracture repair, however, supporting data is limited. In one study, obese patients were seven times more likely to have a complication and over four times more likely to have reoperation than non-obese patients after pelvic ring injury fixation. 5 Other studies have corroborated these findings after acetabular fracture repair, with increased chances of wound infection and reoperation. 6 Waist-hip ratio has been suggested to be more predictive than BMI for wound complications after treatment of pelvic and acetabulum fractures. 7 To our knowledge there have been no other studies that have addressed the so called “apple” vs “pear” phenomenon and its effects on postoperative complications. This study may more reliably explain the effects seen by BMI on complication rates and could explain mixed results seen with studying BMI to date. We had similar findings with higher reoperation and infection rates for patients with elevated BMI.
There are many possible reasons for this finding. Increased body habitus may increase strain across fracture sites thus predisposing the patient to malunion, nonunion or premature failure of fixation. Obese patients may also have poor soft tissue envelope and require larger dissections, thus predisposing them to higher rates of infection. Therefore, it may be advantageous to delay or encourage slower weight bearing advancement to lessen strain across the repair site to prevent premature implant failure. It may also be beneficial to employ infection reduction strategies for patients with elevated BMI to counteract the higher infection risk. Percutaneous treatment of acetabular fractures may be a reasonable alternative to traditional open management in high-risk patient groups and may decrease rates of infection. 8 Less invasive approaches should be balanced with the need to provide adequate stability.
In contrast, it has been suggested that in young and middle aged patients, obesity, fracture type, and delay of surgery had no influence on reduction quality post-pelvic ring fracture reduction. 9 Factors other than BMI have also been shown to increase post-operative complications after operative management of pelvic fractures. Infection after acetabular fracture repair was found to be more likely to occur in patients who had longer LOS, prolonged operative times, or who experienced delay in time to fixation. 10 The increased infection risk in patients with longer LOS finding was consistent with the results of this study as infection risk increased by 4% (CI 1%–8%) for each additional inpatient day. Patients with longer length of stay after pelvic or acetabular fracture fixation may have suffered more severe concurrent injuries or polytraumatic injuries, which may explain higher infection rates. Patients with more complex or numerous injures may also have prolonged operative times and need multiple surgeries, both of which contribute to increased infection risk and longer hospital stays. Causality in this instance may, in fact, be reversed as patients that suffer acute post-operative infection would inherently require longer stays. High quality studies are needed to further elucidate this variable.
Despite finding no significance between smoking status, cardiac co-morbidities, and psychiatric history with complication rates, we found a trend for smoking status and cardiac history with increased infection rates. Smoking may increase the risk of morbidity, delays wound healing, increases infection risk, pulmonary and neurological complications, and the likelihood of costly ICU admission. 11 Several studies address smoking as a risk factor for postoperative complications following orthopedic procedures, including spinal and ankle fusion, recovery after spinal decompression, rotator cuff repair and anterior cruciate ligament reconstruction. 12 Smoking contributes to delayed wound healing, increased infection risk, impaired fracture union, increased LOS, and increased cardiopulmonary complications in patients undergoing elective total joint arthroplasty. 13,14 Smoking also has deleterious effects on healing after orthopedic trauma, including tibial and open fractures. 15 Smoking has not been discussed in regards to pelvic and acetabular fractures in the literature to date.
Preoperative smoking cessation has been suggested in patients undergoing elective orthopedic procedures as it may help reduce postoperative complications, especially with longer duration of abstinence. 16 Nicotine replacement therapy, bupropion, and varenicline appear to be efficacious in helping achieve and maintain smoking abstinence. 13 While it may be possible to mitigate smoking as a risk factor in elective procedures, this is often not feasible in trauma patients.
Psychiatric history showed a trend toward increased reoperation rates. Psychiatric history has been shown to impact outcomes after tibial plateau fractures, 17 distal humerus fractures, 18 and shoulder surgery. 19 A large multi-center study found that admissions with a psychiatric diagnosis had higher odds of prolonged hospital stays, surgical complications, and in-hospital mortality following inpatient orthopedic procedures. 20 This finding was exacerbated in low socioeconomic status populations. Patients with hip fractures and psychiatric co-morbid conditions demonstrated longer LOS, poorer outcome, and increased likelihood of discharge to an alternative living situation requiring higher level of assistive care than their preoperative residence. 21 While no significant association was found for psychiatric diagnosis and complication rates for the current study, studies with higher power may be able to elucidate these associations in the pelvic and acetabular fracture population.
Surgical approach is important when considering infection in orthopedic procedures. In total joint arthroplasty, there is current debate about optimal approach during total hip replacement surgery with regards to infection rates. 22 The present study found a novel association between surgical approach and infection risk in addition to reoperation rates in patients with pelvic and acetabular fractures. Larger surgical site exposures extend the infectious nidus and may succumb patients to increased risk of complications. While Stoppa and modified Stoppa approach have shown lower rates of blood loss than the ilioinguinal approach, 23 no difference in infection or complication rate has been reported to date after pelvic fracture stabilization. 24 It has been proposed that topical antibiotics may reduce the incidence of surgical site infection after open pelvic and acetabulum fixation, 25 which may be a viable infection reduction strategy in high-risk patients.
It should be noted that there may be a selection bias in patients undergoing an ilioinguinal approach as more invasive and larger exposures are required for worse injuries, leading to higher rates of complications. While this association was statistically significant, there was a wide confidence interval due to small sample size. As such, direct comparisons between similar approaches were not possible, but rather we compared individual approaches to other approaches as a whole. The different approaches described here have different indications for use depending on fracture pattern, require different levels of expertise to perform, and vary widely in amount of surgical dissection needed. Surgical approach was necessary to include as a confounder in such an analysis, however, results should be interpreted with caution.
Insurance carrier was used as a surrogate for socioeconomic status in our sample population. To our knowledge this is the first study that examined the effect of insurance carrier on outcomes in operative management of pelvic fractures. There was a trend toward significance for increased re-operation rates and Medicaid payor status. Studies have found increased complication rates for patients with Medicaid post spine surgery. 26,27 A later study found a more specific increased association of surgical site infections after spine surgery for Medicaid payors. 27 Other studies have also found associations between government funded insurance and complication rates in total hip arthroplasty, 28 total knee arthroplasty, 29 and shoulder arthroplasty. 30 Future studies with improved statistical power should analyze the association of insurance payor status and complication rates post pelvic fracture surgery.
There remain many limitations to our current study. We assumed that all patients with operative CPT codes were treated surgically. Valid coding in addition to precise data entry is essential to our analysis. We performed an in-depth chart review to help mitigate errors in coding. We did not perform a sub-analysis based on age due to small sample size. Our findings may not be applicable to specific age ranges, especially the elderly population as our sample was mostly middle-aged patients. Follow up time showed a large standard deviation. Our center takes care of a resource intensive inner-city urban population. Contacting patients for follow up was not always possible. We were not able to identify the specific cause of the prolonged length of stay and could be attributable to multiple factors including co-morbid injuries and treatment of infection. The most apparent limitation is the low power of the study due to the small sample size. Post-hoc analysis showed only the ability to observe large effects and could potentially miss small to moderate sized effects. Large multi-center studies are needed to validate the findings of the current study, including the role of BMI, LOS, and approach on outcomes after fixation of pelvic ring and acetabular fractures. In addition, the effects of smoking, heart disease, psychiatric diagnosis, and payor status on outcomes should be explored further.
Conclusion
This study found that higher BMI and ilioinguinal approach were associated with complications following surgical stabilization of pelvic fractures. Additionally, this study found an association between longer length of stay and increased infection risk. Smoking status, prior cardiac history, insurance status, and psychiatric history may also contribute to post-operative complications in these patients. Knowledge of these risk factors can help trauma surgeons mitigate modifiable risk factors and better educate patients on outcomes following pelvic surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.