
Abstract
Introduction:
Chronic unreduced shoulder dislocations are rare in orthopaedics. The aim of this study is to report how conservative treatment of chronic unreduced shoulder dislocations is done and evaluate the functional outcome in a low-middle income environment.
Patients and methods:
This was a hospital based prospective observational study carried out from January 2008 to January 2018. Cases of unreduced shoulder dislocations of at least 1 month duration were included in the study. Closed reduction was done by progressive soft maneuvers described by Kocher. Epi Info software was used to analyze this data. Results were represented on tables to ease organization and comprehension.
Results:
One of the 33 had a bilateral chronic unreduced anterior dislocation. The ages ranged from 21 to 80 years, with a mean age of 42.71 ± 16.13 years. The male to female ratio was 3.2:1. The duration of dislocation ranged from 1 to 120 months. Majority of the cases 79.4% (n = 27) had successful closed reduction. The average score was 78.04/100, representing a good score.
Conclusion:
Although treatment by non-operative method is a challenge, fair to good functional outcome can be obtained if this procedure is carried out under general anesthesia and adequate relaxation.
Introduction
Dislocations of the shoulder account for almost 45% of all dislocations with almost 90% being the anterior subtype. 1
A chronic unreduced shoulder dislocation is a rare entity in orthopaedics, with only few cases being reported in the literature. 2
Rowe and Zarins used 3 weeks to define chronicity because closed reduction is seldom possible after three weeks. 3 Goga later on used 1 week to define a shoulder dislocation as being chronic. 4 He further sub-classified them into early (1–3 weeks), late (3–12 weeks) and ancient (>12 weeks).
Treatment options for chronic unreduced dislocations of the shoulder include conservative management, closed reduction, open reduction, hemiarthroplasty, and total shoulder replacement. 5 Open reduction and joint fixation is recommended for most unreduced anterior dislocations of the shoulder and different fixation methods have been used to prevent redislocation. 6
Closed reduction of chronic unreduced shoulder dislocation is a challenge because fibrous and capsular contractures occur across the base of the glenoid. The capsule itself becomes adherent in the glenoid fossa, which prevents closed reduction. In chronic anterior dislocations, a compression fracture occurs in the posterolateral aspect of the humeral head, where it impinges against the anterior glenoid rim, further locking the shoulder in the dislocated position. The choice of procedure to restore glenohumeral congruity depends on such factors as the chronicity of the injury, associated bony and soft tissue injuries, age, hand dominance, vocational requirements, and medical co-morbidities. 5,6
The penchant for seeking unorthodox medical treatment for musculoskeletal injuries makes chronic shoulder dislocation one of the common complications of shoulder injuries in the West African sub-region. 7
There are few published data on the conservative treatment of this condition in sub-Saharan Africa and most developing countries. 8 –10 The aim of this study is to report how conservative treatment of chronic unreduced shoulder dislocations is done and evaluate the functional outcome in a low-middle income environment.
Patients and methods
Study design
This was a hospital based prospective observational study carried out from January 2008 to January 2018 at the Cardinal Paul Emile Leger National Rehabilitation Center for Persons with Disabilities (CNRPH) in YAOUNDE. All the activities carried out at this center contribute to the rehabilitation and reconversion of disabled people.
Study population and sampling
The study involved all patients who presented at the Cardinal Paul Emile Leger National Rehabilitation Center for Persons with Disabilities (CNRPH) in YAOUNDE with a chronic unreduced shoulder dislocation within the 10 years period. The sampling was done in a consecutive manner
Selection criteria
Inclusion criteria: All cases of unreduced shoulder dislocations of at least 1 month duration without local infection were included in the study
Exclusion criteria: Patients from whom relevant data could not be obtained and those who didn’t consent for the study were excluded.
Study procedure
Patients who presented with chronic unreduced shoulder dislocation were approached. Those who met the inclusion criteria were counseled on the aim and importance of the study. Patient demographics, duration of dislocation, mechanism of injury and reason for delayed treatment were recorded. When available, patient X-rays, CT scans and MRIs were reviewed to identify associated bony and soft tissue pathologies.
Closed reduction was done, under general anesthesia with maximum muscular relaxation, and progressive soft maneuvers described by Kocher: traction (Figure 1a) in the axis of each upper limb, external rotation and abduction (Figure 1b). In some cases, the reduction maneuver was done with C-arm guidance when available. The reduction was confirmed clinically (Figure 2a and 2b) after which the shoulder was immobilized by a temporary arthrodesis with two crossed pins (Figure 3a) completed by an elbow-to-body Desault bandage (Figure 3b) for 6 weeks. Early rehabilitation was undertaken as soon as the double contention was removed to favor the progressive recovery. The rehabilitation involved passive and active shoulder range of motion and joint amplitude exercises. Stability tests after removal of the immobilization at day 45 and before the patient’s exit after 20 sessions of rehabilitation were satisfactory. During follow-up visits scheduled every 45 days, the Constant-Murley functional assessment of the shoulder Score was done and the score obtained was recorded. 11 The score is divided into four subscales: pain (15 points), activities of daily living (20 points), strength (25 points) and range of motion: forward elevation, external rotation, abduction and internal rotation of the shoulder (40 points). The score was interpreted as follows: score of 100–90 (Excellent); 89–75 (Good); 74–51 (Fair); and 50 or less (Poor). A subjective evaluation by the patients was also assessed.
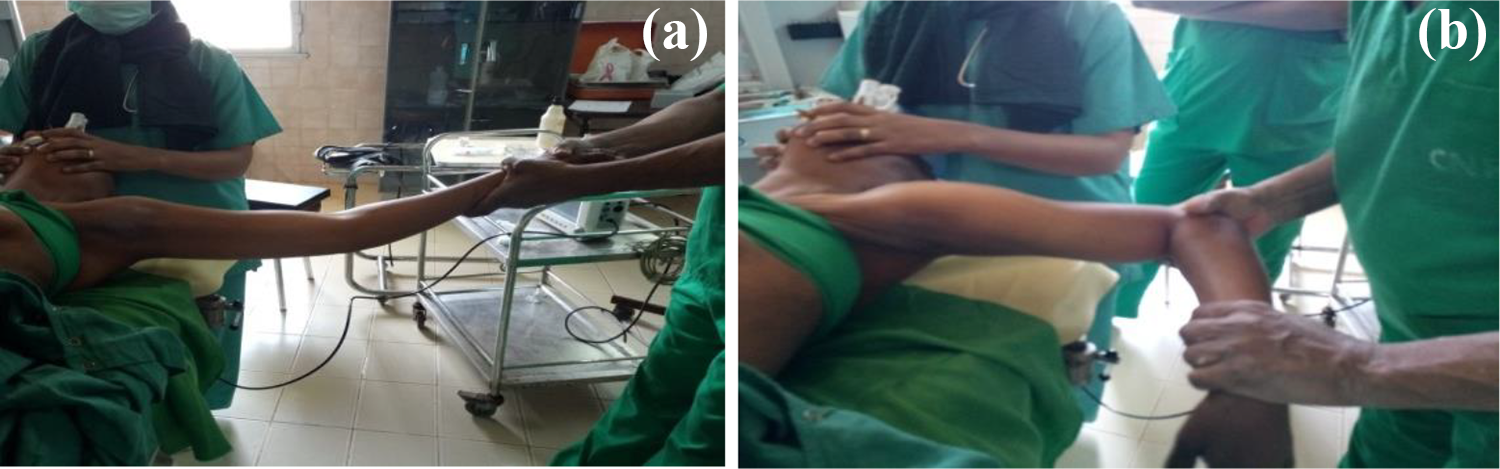
(a) Traction of the shoulder. (b) Rotation of the shoulder.

(a) Unreduced shoulder. (b) Reduced shoulder.
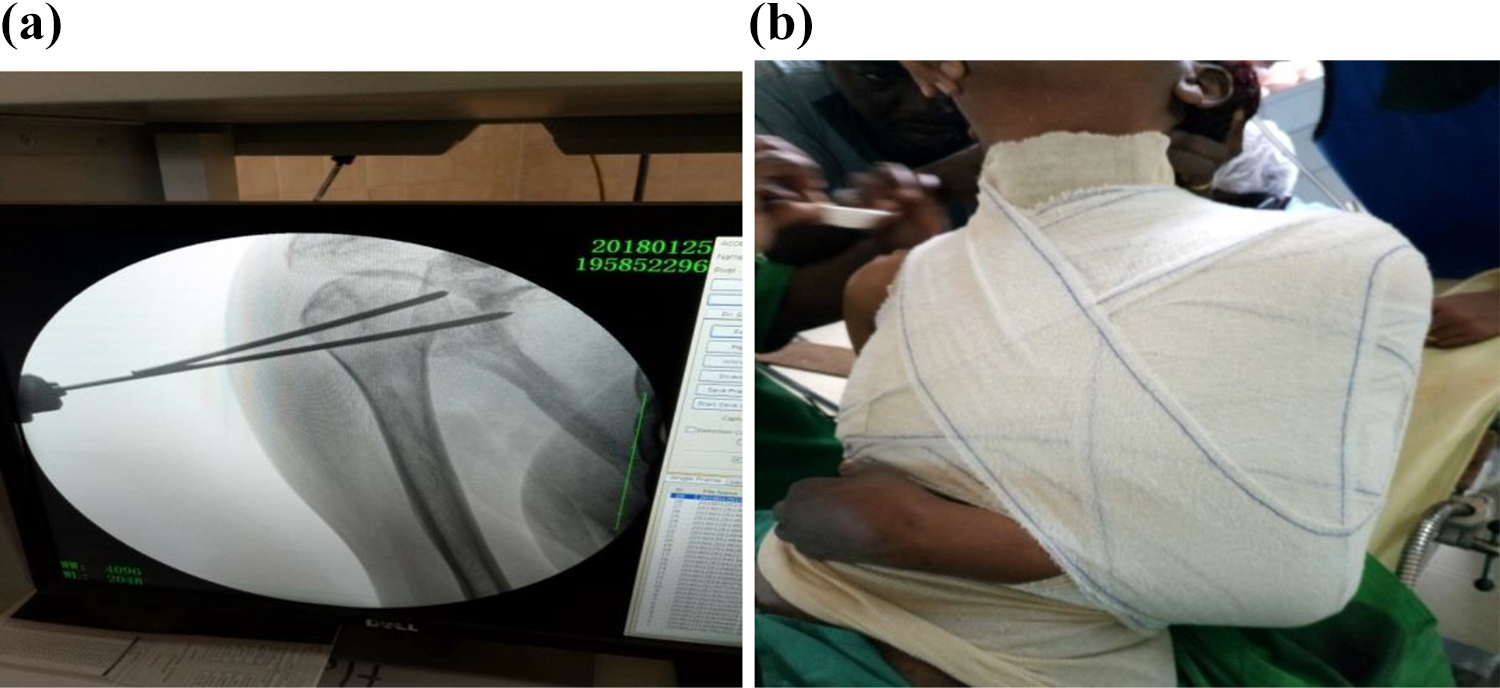
(a) Temporal K-wire fixation. (b) Arm to body bandage.
Data management and analysis
Data was kept secured and all information was recorded in a computer protected by a password. Epi Info software was used to analyze this data. Results were represented on tables to ease organization and comprehension.
Ethical consideration
Ethical clearance was obtained from the Faculty of medicine and biomedical sciences of the University of Yaounde 1 Institutional Review Board (IRB). An administrative approval was equally obtained from the director general of the The National Rehabilitation Center for Persons with Disabilities. A consent form was presented to participants explaining the procedure of the study, the goals of the research and why their collaboration was important.
Results
In this study, 42 patients were surveyed with a chronic unreduced shoulder dislocation. Nine patients who didn’t fulfill the inclusion criteria were excluded from the study. One of the 33 had a bilateral chronic unreduced anterior dislocation.
The ages ranged from 21 to 80 years, with a mean age of 42.71 ± 16.13 years. There were more males than females giving a male to female ratio of 3.2:1.
Characteristics of the chronic unreduced shoulder dislocations
Among the 34 dislocations 33 were anterior while only one was posterior (Table 1). Four of the 33 subjects had a past history of epilepsy, and one was diabetic. The others didn’t report any contributive past history. The majority of the shoulders, 85.3% (n = 29) never had a prior dislocation while 14.7% (n = 5) had at least a prior shoulder dislocation. Most of them (n = 26) had their right side affected while a few (n = 7) had the left side affected. Among the 26, 25 were right-handed while only 7 were left-handed. Three patients had axillary nerve injury, while the rest didn’t have a nerve injury.
Characteristics of the chronic unreduced shoulder dislocations.
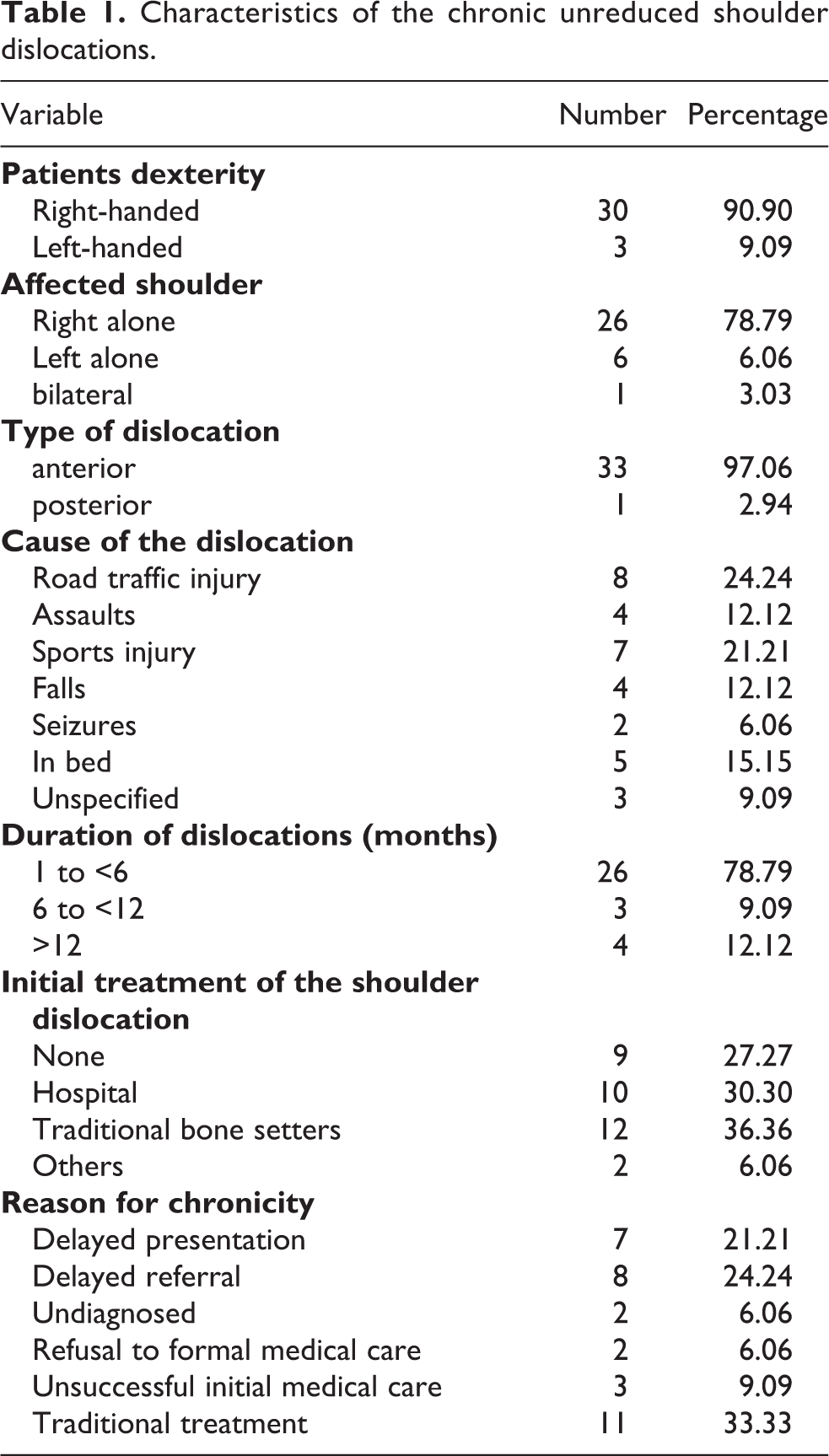
Sports injury and road traffic injuries were the most common causes of shoulder dislocation. The duration of dislocation ranged from 1 to 120 months with a mean duration of 11.15 ± 26.86 months. In most cases the dislocation was less than 6 months old. Most of them 35.29% (n = 12) initially went to traditional bone setters for treatment while 29.41% (n = 10) initially sought medical attention. However the others either didn’t have any initial treatment (n = 9) or had a bystander or a family relation help them initially (n = 3). The difference was not statistically significant (p = 0.743).
The reasons for chronicity were varied. The patient reported that they spent time receiving care from traditional bone setters (n = 11). A couple of them either presented late for formal medical care (n = 7) or were referred late enough to get adequate medical care (n = 9). A few either refused medical care when it was proposed to them (n = 2), or had care from unqualified medical staff and had unsuccessful reduction (n = 3). However, the difference in the reasons for chronicity wasn’t statistically significant (p = 0.45).
Initial imaging assessment
All subjects on initial assessment were requested to do shoulder x-rays (antero-posterior and axillary views), shoulder arthro-CT scan or an MRI scan. All the patients had the x-rays done, only five had an arthro-CT scan due to financial constraints and none did an MRI scan, not only due to financial constraint but also due to unavailability of MRI scan machine during the initial assessment of the subjects.
The x-rays showed two cases of Hill-Sachs lesions and two cases of greater tuberosity fractures. The arthro-CT scans showed one case of Hill-Sachs lesion, two Bankart and one bony Bankart lesions.
Treatment modality
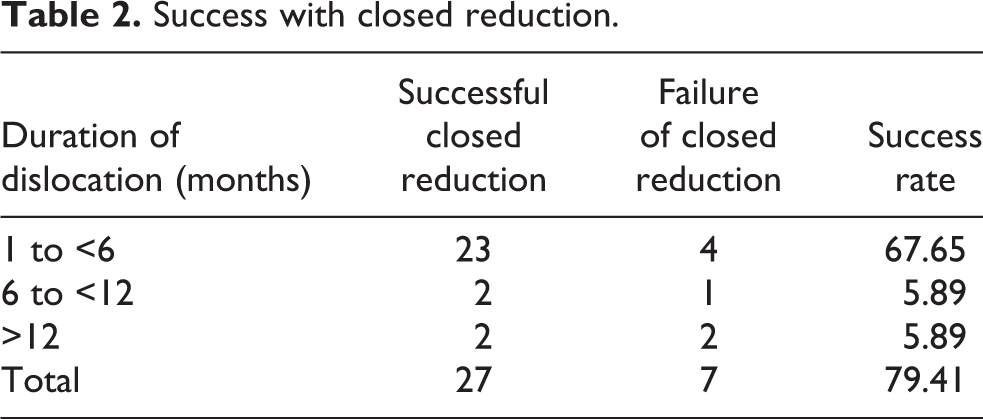
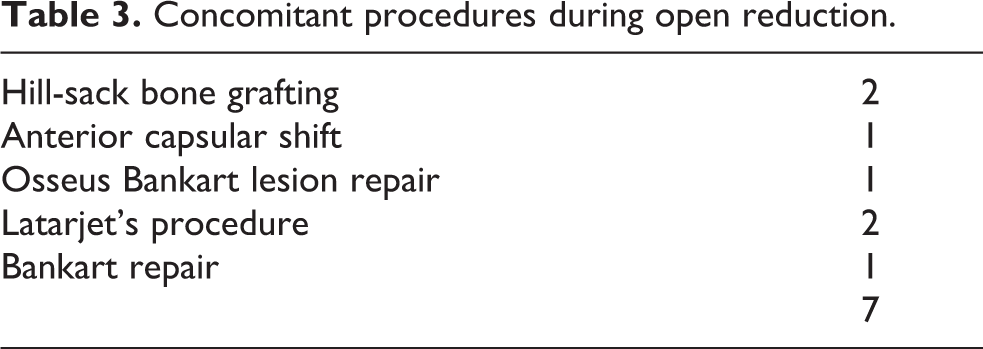
All 34 dislocations were initially programmed for closed reduction by external maneuvers, and prepared for conversion to open reduction if failure of closed reduction (Table 2). Those who had unsuccessful closed maneuvers underwent immediate open reduction with concomitant procedures as shown in Table 3, or were deferred for adequate preparation for open reduction. A successful closed reduction was verified and confirmed either by fluoroscopy when it is available or by the ease in mobilizing the shoulder joint under anesthesia and the disappearance of the observational signs of shoulder dislocation. Majority of the cases 79.4% (n = 27) had successful closed reduction while the rest 20.6% (n = 7) had the procedure converted to open reduction.
Success with closed reduction.
Concomitant procedures during open reduction.
The mean duration of dislocation for those who had successful closed reduction was 7.44 ± 22.83 months while that of open reduction was 25.42 ± 37.56 months.
Immediate post reduction complications
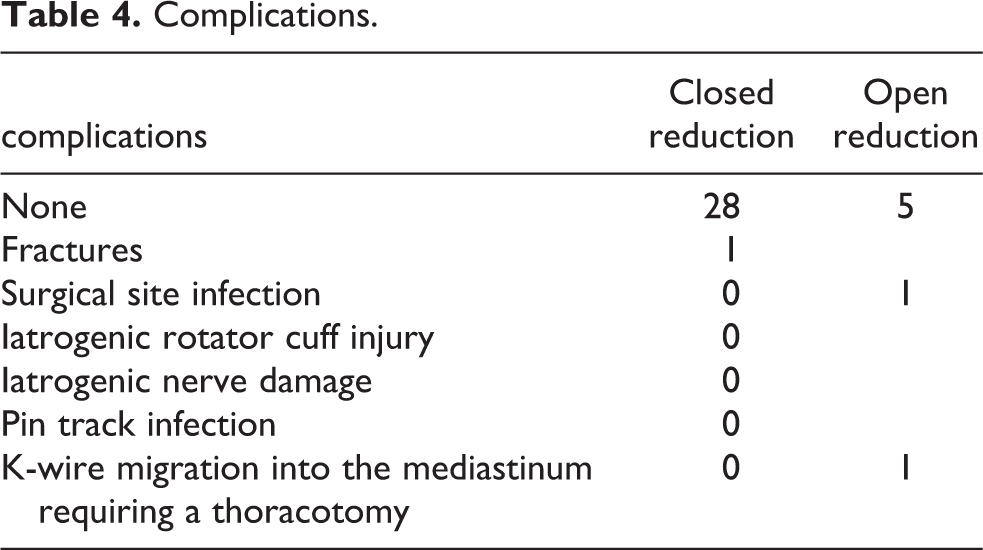
Complications related to either open or closed reduction were minimal in our study (Table 4). However, there was a case of k-wire migration into the mediastinum that required referral to a thoracic surgeon who did a thoracotomy to remove the k-wire.
Complications.
Duration of hospitalization
The duration of hospitalization for those who had closed reduction varied from 1 to 4 days with a mean duration of hospitalization of 2 ± 2.37 days, while that for open reduction varied from 5 to 21 days with a mean duration of 7 ± 11.22 days.
Prospective review at the clinic
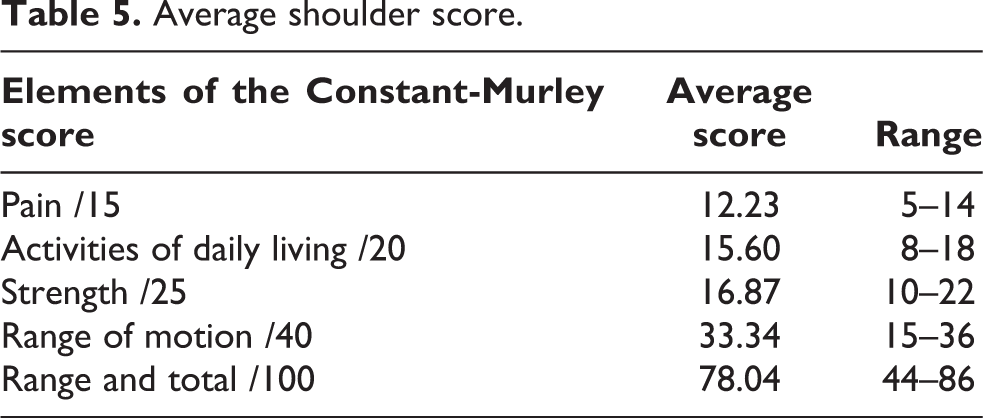
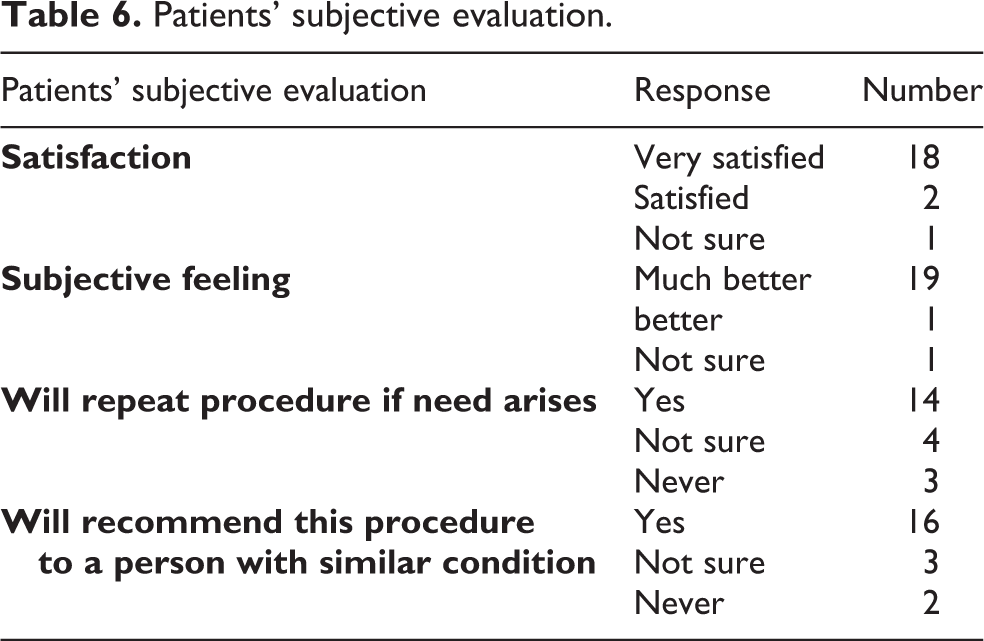
The average follow-up duration at the latest visit was 17 months (range 3–72 months). There were 21 shoulders reviewed that were treated by closed reduction. The average score was 78.04/100, representing a good score as shown in Table 5. Subjectively, most of the patients were very satisfied (n = 18), felt much better (n = 19), could repeat the same procedure if need arises (n = 14), and will recommend this procedure to a person with similar condition (n = 16) as shown in Table 6.
Average shoulder score.
Patients’ subjective evaluation.
Discussion
Chronic unreduced shoulder dislocations are extremely rare in the literature. 2,12 Shoulder dislocations are mostly traumatic, but may also result from a trivial injury. Dislocation resulting from a trivial event is more common with increasing age and when there is weakness or degeneration of the soft tissue about the shoulder joint, such as the subscapularis and other rotator cuff tendons. 13 Most cases in our study resulted from trauma from either a road traffic crash or sports injury. All cases that resulted from road traffic crash involved young individuals within the age range between 25 and 47 years. This study identified a patient with unusual chronic unreduced bilateral anterior shoulder dislocations.
Initial care of the shoulder injury was mainly unorthodox, which may explain the reason for the chronicity. Most of the patients resorted to inadequate medical remedy or had treatment from traditional bone setters. It is recommended that unreduced chronic anterior shoulder dislocation should be treated with an open reduction and reconstruction of the specific lesions, unless the patient is old or debilitated. 13 Due to financial constraints, most patients in this series could not afford surgical procedures, and were therefore treated non-operatively. The clinical outcome was marked by a good functional Constant-Murley shoulder scores. However, Golga observed that surgically treated patients fared better than those whose shoulders were left unreduced, regardless of the duration of the dislocation. 4
Most authors recommend temporal shoulder joint transfixation with Kirschner-wire to prevent redislocation following open reduction for 4 weeks. 14,15 in our context, we used two Kirschner-wire fixation for 4–6 weeks and an arm sling to stabilize the shoulder after successful reduction by external maneuvers. Capsulolabral complex repair has been recommended as a more favorable option to stabilize the joint compared with metallic fixation methods that enabled early motion the day after surgery. 16 Most reports on operative management have yielded a good to excellent outcome. 16 –18 The fair-to-good outcome in this study may be related to the longer duration of immobilization compared with other studies that used a maximum of 4 weeks of immobilization. The delay in initiating physiotherapy also affects the functional outcome. Moreover, chondral damage by the Kirschner-wires used for humeroglenoid transfixation of the joint may also affect the outcome. Nevertheless, the short duration for which patients presented for follow-up care may compromise the true definitive outcome 7
In this study, a case of chronic unreduced posterior shoulder dislocation was identified. It is worth mentioning that posterior shoulder dislocations are the most commonly missed major joint dislocation in the body. 19
Conclusion
Chronic unreduced shoulder dislocations are relatively common in low-middle income settings. Although treatment by non-operative method is a challenge, fair to good functional outcome can be obtained if this procedure is carried out under general anesthesia and adequate relaxation. However, a longer follow-up period is needed for the detection of potential complications that may arise and adversely affect the outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.