
Abstract
Introduction:
Sacroiliac joint (SIJ) can be a nociceptive source of the pain in lower back. Clinical diagnosis of SIJ pain remains yet problematic. The cause of SIJ pain is multifactorial. The pain may be a result of an inflammatory disease, arthrosis, traumatic injury, infectious process or overload. The potential role in SIJ examination have pain provocation tests.
Objective:
To review and further discuss the validity of some of the mostly used clinical provocation tests such as Distraction test, Thigh Thrust test, Compression test, Sacral Thrust test, Patrick’s (FABER), Gaenslen’s test, Standing Flexion Test, Gillet Test and Shimpi Prone test.
Method:
A literature search was conducted using PubMed. Reviewed were studies between 2005 and 2020 in English, Slovak and Czech with keywords: sacroiliac joint, sacroiliac assessment, provocation tests. The methodology of studies was not considered.
Discussion:
It is challenging to determine whether SIJ is the actual source of the pain by using only one of the provocation tests. Therefore, it is beneficial to combine more compression tests, what will also increase the validity of testing. Other widely used SIJ tests are palpation test, however their validity is poor.
Keywords
Introduction
Lower back pain (LBP) is the most common reason for seeking medical care 1 and it is often challenging to determine the exact cause of the LBP. 2 Sacroiliac joint (SIJ) can be a nociceptive source of the pain in lower back and lower limbs. 3 SIJ pain has vague symptoms and can be mistaken with other lumbar structures. These joints play a key role in spinal stability and are linking parts between axial skeleton and lower limbs. SIJs have very complex anatomy. There is a minimal movement in SIJ in sagittal plane, proximately 0.5 degree, and the translation ranges between 0.5 and 2.0 mm. 4 The cause of a SIJ pain is multifactorial. The pain may be a result of an inflammatory disease, arthrosis, traumatic injury, 5 infectious process 6 or overload. The most common overload and/or injury mechanism of SIJs occurs in a combined motion of axial load and rotation. 7 The ligaments that stabilize SIJ are sacroiliac (anterior, posterior), sacrotuberous, sacrospinous, and interosseous, 8 which are accompanied by muscles that are a dynamic component of the pelvic girdle. The clinical diagnosis of SIJ pain remains yet problematic. The potential role in SIJ examination have pain provocation tests. The palpation tests are another group of widely used tests. Further objective assessments related to SIJ issues are gait analysis, lower limbs length, SIJs emplacement and SIJ palpation to review consistence, reveal any swelling etc. However very important role in clinical examination of SIJ have special tests, which we introduce and in details describe in further sections.
Distraction test
Distraction (Grapping) test is performed in supine position with extended legs. Examiner places hands on patient’s anterior superior iliac spines (ASIS) and applies postero-lateral pressure towards SIJs (Figure 1). Another possible way to perform the test would be with a cross-over grip (Figure 2). The test is positive if it reproduces patient’s symptoms in SIJ. It is essential to repeat the test for three to six times. One has to be careful while applying pressure during these tests, it is certainly not a manipulation but rather a smooth motion.
Sensitivity 60%
Specificity 81% 9

Distraction test.

Distraction test – cross-over grip.
Thigh thrust test
This test is carried out with the patient is supine position, legs extended. Examiner standing by patient’s side brings the contralateral patient’s leg into 90 degrees’ hip flexion, knee is bent, and places one hand beneath SIJ of tested side (Figure 3). The longitudinal pressure is applied on the bent knee, through the femur, towards examined SIJ (Figure 4). Test is positive if pain is reproduced in examined SIJ. It is essential to repeat the test for three to six times.
Sensitivity 88%
Specificity 69% 9

Thigh thrust test – hand placement.

Thigh thrust test.
Compression test
Compression test, also known as Approximation test, is performed in side-lying position. Patient lies on the asymptomatic side, with hips flexed into 45 and knees into 90 degrees. Examiner stands behind the patient with hands on patient’s upper front iliac crest (Figure 5) and applies the vertical pressure. Reproducing patient’s symptoms indicates the positivity of the test. It is essential to repeat the test for three to six times.
Sensitivity 69%
Specificity 69% 9
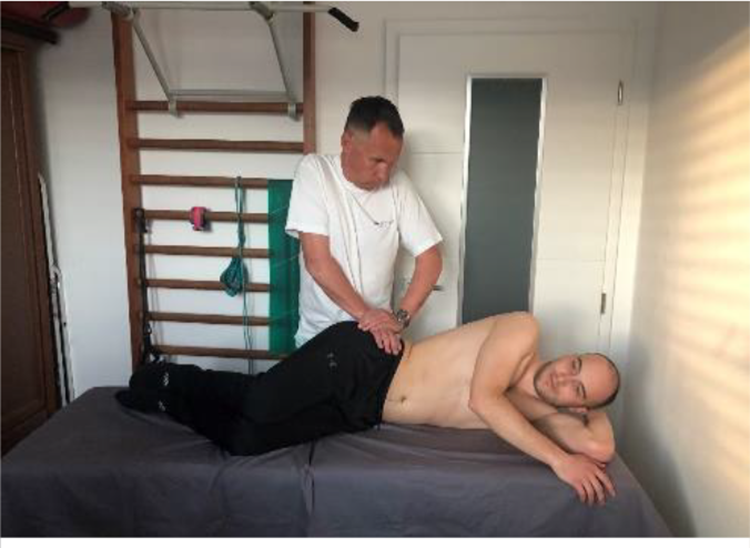
Compression test.
Sacral thrust test
Sacral Thrust test is performed with the patient prone,examiner (places hands, one over the other, on the S2 level (Figure 6) and applies an anteriorly directed pressure. Test is positive if pain occurs in SIJ. It is essential to repeat the test for three to six times. One has to be careful while applying pressure during pain provocation tests, it is certainly not a manipulation but rather a smooth motion.
Sensitivity 63%
Specificity 75% 9

Sacral thrust test.
Patrick’s (FABER) test
Patrick’s test, also known as FABER test what stands for hip being in Flexion, Abduction and External Rotation. Patient lies supine, examiner flexes the leg of the tested side into 45 degrees in hip and 90 degrees in knee. From this position the flexed leg is taken laterally. Contralateral iliac crest has to be fixed to prevent any pelvic rotation (Figure 7). Another test variant would be to rest patient’s lateral ankle on the contralateral knee. Pain in SIJ of the tested side indicates that the test is positive, however this pain must not be mistaken with any pain localized in the hip.
Sensitivity 69%
Specificity 16% 2

Patrick’s test.
Gaenslen’s test
Patient lies supine, pulls and fixes non-tested leg towards the chest, meanwhile the lower leg of the examined side is handing off the lateral edge of the treatment couch. Examiner creates pressure on the distal femur, pressing downwards into slight hip extension (Figure 8). Pain the tested SIJ indicates the test positivity.
Sensitivity 53%
Specificity 71% 9

Gaenslen’s test.
Standing flexion test
Standing flexion test which also can be found under Vorlauf test, belongs to the group of palpation SIJ tests. Patient stands straights, examiner is behind the patient and places his thumbs on posterior superior iliac spines (PSIS) (Figure 9). Patient is asked to slowly bend forward, meanwhile the examiner observes the thumbs placed on PSIS (Figure 10). The test is positive if thumbs will not remain at the same level throughout patient’s bending and/or at the end of it. The side with greater movement (cranially) is the affected one and this finding indicates a SIJ dysfunction.
Sensitivity 17%
Specificity 78% 4

Standing flexion test.

Standing flexion test – bending.
Gillet test
This test is also known as Stork test, but in some literature it may be also found under Marching test and it is another one from the group of palpation SIJ tests. Patient stands straight, examiner stands and palpates PSIS of the tested side. Other thumb is placed on the S2 spinous process. Thereafter, patient lifts the leg of the tested side to 90 degrees’ hip flexion (Figure 11). In normal SIJ function, the PSIS will drop under the level of S2. If this does not happen, or PSIS drops only minimally, the test is positive and this indicates SIJ dysfunction.
Sensitivity 43%
Specificity 68% 2

Gillet test.
Shimpi Prone test
Shimpi Prone test also belongs to the group of palpation SIJ tests. As the name suggests, this test is carried out in prone position. Examiner places a hand beneath one of the patient’s ASIS and asks him to hyperextend the tested leg up to 15 degrees (Figure 12). Test is considered to be positive if patient’s ASIS is lifted up from the examiner’s hand that was placed beneath it. If the pressure of ASIS onto the examiner’s hand increases, the test is negative.
Sensitivity 82%
Specificity 77% 10

Shimpi Prone test.
Test combinations
It is challenging to determine that the pain comes from SIJ by using only one test. Such testing may lead to false positivity or false negativity. Potential source approved by more stress tests can increase the validity of an actual testing. Laslett et al. 9 tested combination of several tests to detect pain in SIJ. Included was Distraction test, Thigh Thrust test, Gaenslen’s test, Compression test and Sacral Thrust test in a study with 48 patients. Sensitivity and specificity for 3≤ out of 6 positive SIJ tests were 94% and 78%, respectively. According Laslett et al., the provocation tests do have value in clinical diagnosis of SIJ pain. Further, if pain is not brought up by any of these tests, SIJ can be excluded as the origin of the pain.
The outcome values of SIJ testing maneuvers also studied van der Wurff et al. 11 Sixty participants with LBP were involved. The combination of Distraction test, Compression test, Thigh Thrust test, Patrick’s test and Gaenslen’s test was applied. Sensitivity and specificity in mutual combination of these maneuvers was 0.85 (95% CI) and 0.79 (95%), respectively. According van der Wurff et al. using combination of three of more positive tests leads to clinical finding of the origin of pain coming from the SIJ.
Diagnostic SIJ tests validity was also an object of a study for Szadek et al. 12 This analysis involves 18 studies. The highest validity was reached for the Thigh Thrust test (DOR, 18.461; CI, 5.82–58.53), Compression test (DOR, 3.88; CI, 1.7–8.9), and for the combination of three or more tests (DOR, 17.16; CI, 7.6–39).
Stuber 13 as well tested the validity of SIJ maneuvers, including six studies into his research. He concluded Distraction test, Compression test, Thigh Thrust test, Sacral Thrust test and Patrick’s test to be valid in regarding of potential SIJ pain.
SIJ palpation tests
There are other tests used for SIJ examination, such is Standing Flexion test, Gillet Test or Shimpi Prone test. These should point out the SIJ dysfunction and are aimed to reveal the optimal SIJ motion. Palpation itself is very important factor here.
Shimpi et al. 10 tested the effectiveness of the one that holds its author’s name, the Shimpi Prone test. Study involves 23 patients with pain origin in SIJ, and 22 in asymptomatic control group. This test came up with high value of sensitivity and specificity, 82% and 77%, respectively. On the other hand, the limitation of this study may be using a gold standard, which was not optimal, and therefore biased values of sensitivity and specificity.
The actual problem with assessing the SIJ motion is the fact, that SIJ has very limited motions, therefore it is problematic to examine it. Kibsgård et al. 14 looked at the range of motion in SIJ during one leg stance. The rotation of max. of 0.5 was measured. Translation motion was not detected. According Kibsgård et al. the SIJ motion is almost impossible to palpate and the palpation test itself does not provide an important information in clinical examination.
Another problem is the variability of findings among examiners. Further the difference in lower limb length may affect the actual SIJ and therefore bias the test’s objectivity. 15 The assessment validity among examiners is also low in regarding of replicate these tests. 16
The actual comparing of pain provocation tests with palpation ones was done by Soleimanifar et al. 17 Fifty patients participated. As palpation tests, Sitting Flexion test, Standing Flexion test, Prone Knee Flexion test and Gillet Test were chosen. For the other test group, Patrick’s test, Thigh Thrust test and Resisted Abduction test were examined. There was found no significant relationship between these two groups of tests. With a similar conclusion came up Robinson et al. 18 finding palpation tests to have lower validity than pain provocation tests.
Seronegative spondyloarthropathy
Clinical examination of SIJ can point at seronegative spondyloarthropathies. The most common disorder from this group is ankylosing spondylitis (AS) which manifests with morning pattern of inflammatory pain and affects mainly SIJ. 19 These patients have flexed posture. The purpose of Castro et al. 20 study was to examine the effectiveness of SIJ examination in AS patients. Twenty patients with AS were examined with Lasseque test, Standing Flexion test and with provocation tests as Gaenslen’s test, Sacral Thrust test, Patrick’s test and dorsal ligaments were palpated. Pain provocation tests resulted with higher validity in detecting AS. The highest validity got Patrick’s test, sensitivity 71% and specificity 75%. When the mutual combination of more tests was applied, the validity was even greater, sensitivity 86% and specificity 62%. According Castro et al. the pain evoked by provocation tests is correlated with SIJs inflammation. Positivity of some provocation tests with other symptoms may reveal AS. Finding benefit in provocation tests was the purpose of the study by Ozgocmen et al. 21 Examined tests were Compression test, Distraction test, Gaenslen’s test, Mennel’s test, Patrick’s test, Thigh Thrust and Sacral Thrust test and patients underwent MRI of lumbar and sacral spine as well. They found out that provocation tests seem to have higher validity when used in clusters – combinations, and these clusters may be beneficial in distinguishing sacroiliitis from mechanic LBP.
Limitations
The limitation of provocation tests is the SIJ structure itself. The compression may cause an irritation of a ligament, what in some cases may mimic the SIJ pain. The sensitivity and specificity of pain provocation tests is very low. It is possible to increase the validity by combining more tests. The mutual combination of palpation tests does not signify high sensitivity and/or specificity. It may be explained due to lack of motion in SIJ and low palpation ability of the examiner. The exception would be a pathological condition such as lumbago, which is associated with restricted movement.
Further, more systematic reviews with higher level of evidence are needed to be done in this matter.
Conclusion
Identifying the pain origin is a significant issue in lower back treatment. Pain provocation tests in their mutual combination have sufficient validity and are beneficial in the matter of clinical-decisioning in lower back patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.