
Abstract
Biodegradable magnesium-based implants are innovative alternatives that potentially eliminate the need for implant removal. Recent studies have demonstrated the osteogenic properties and bacterial inhibition potentials of magnesium screws. We reported a clinical series of three elbow fracture cases, where magnesium screws were used in the treatment of one radial head and two capitellum fractures. Postoperative clinical courses were uneventful, and fracture healing occurred within 3 months. In all cases, radiolucencies were observed around implants especially in the screw head region at 2 months post-operation, but disappeared with consolidation at 1 year post-operation. All patients achieved near normal range of motion, minimal symptoms and good functional outcomes. No complication such as failure of fixation, loss of reduction, malunion or infection was seen. No implant revision or removal was necessary. Magnesium bioabsorbable screws are shown to be a viable option for these fractures.
Introduction
Most current orthopedic implants used in fracture fixation are made of permanent metals such as titanium or stainless steel, which provide stable fracture fixation. Removal of implants is not routine, but commonly deemed necessary if there is implant protrusion with impingement symptom and pain. These secondary procedures can be very challenging with an increased risk of infection, retained or broken implant, re-fracture and neurovascular injuries. 1 Biodegradable magnesium-based implants are innovative alternatives that potentially eliminate the need for implant removal. Recent studies have also demonstrated the osteogenic properties and bacterial inhibition potentials of magnesium screws. Due to these clinical advantages, the use of magnesium implants has become more popular recently.
Fixation of distal metatarsal osteotomies in the treatment of hallux valgus deformities was one of the most reported applications of magnesium screws in orthopedic surgery. Clinical outcome using magnesium screws were comparable to that of titanium screws. 2 Magnesium screws were also widely used in trauma surgery, with success in the treatment of intercondylar eminence fractures, lateral malleolar fractures and medial malleolar fracture.
In elbow fractures, the load across the fracture and osteogenic properties of an acute fracture setting differ significantly from those of the lower limb counterparts. The fracture pattern, like capitellum and radial head fracture, often benefits from a screw fixation which directly compresses the cartilage side of the osteochondral fragment toward the subchondral bone. Besides, these juxta- or intra-articular fractures, often with significant displacement and associated vascular insult, have a high chance of complication like implant protrusion when osteolysis occurs, resulting in subsequent secondary osteoarthritis. The application of biodegradable magnesium screws is an attractive solution to these problems.
There are only a few clinical studies on the use of magnesium screws in upper limb fracture fixation, including a case of capitellum fracture with concomitant loosening of radial head prosthesis, a case of radial styloid fracture, and a study series of scaphoid fracture fixation which was terminated pre-maturely. While, there is a recent biomechanical in vitro study using 13 human cadaveric humeri, in which Bryan-Morrey Type 1 capitellum fracture was fixed using either magnesium or titanium screws, and it showed that there was no statistical significant difference in terms of construct stiffness, failure cycle and load to failure and the authors recommended the clinical applications of magnesium screws should be further evaluated. 3 Therefore, we would like to present the following clinical case series using magnesium screws in elbow fracture fixation and report the relevant findings. This would be important for the future translation to larger clinical trials.
Case series
Consent was obtained from all patients in this study.
Case 1: Bryan and Morrey type 1 capitellum fracture
A 48-year-old, right-handed female was admitted for a closed fracture capitellum of her right elbow. She slipped on level ground and landed on her right elbow. An X-ray of her right elbow (Figure 1(a)) and a computed tomography (CT) scan with 3D reconstruction (Figure 1(b)) revealed a type 1 capitellum fracture. Using the Kaplan approach, open reduction and internal fixation was performed under general anesthesia. Two 2.7 mm Magnezix (Syntellix AG, Hanover, Germany) screws were used for fracture fixation, one directly from the lateral edge of the articular surface and the other in an anterior-to-posterior direction. Postoperatively, a hinged elbow brace in forearm neutral position was used for rehabilitation for 6 weeks. Out of brace mobilization in supination, pronation, flexion and extension was encouraged three times a day, 10 cycles each direction. Progressive strengthening began at 6 weeks onward and full training at 3 months postoperatively. She was pain-free all along and a full range of movement with 130° of flexion, 0° of extension, 90° of supination, and 85° of pronation was restored at 8 months post-operation (Figure 1(c)). Her Disabilities of the Arm, Shoulder and Hand (Dash) score was 0. As shown in Figure 1(a), radiolucency was noted around the screw at 2 months post-operation but disappeared with resorption at 12 months post-operation. Radiological healing was documented at 8 weeks postoperatively, and complete consolidation was noted at 5 months postoperatively.
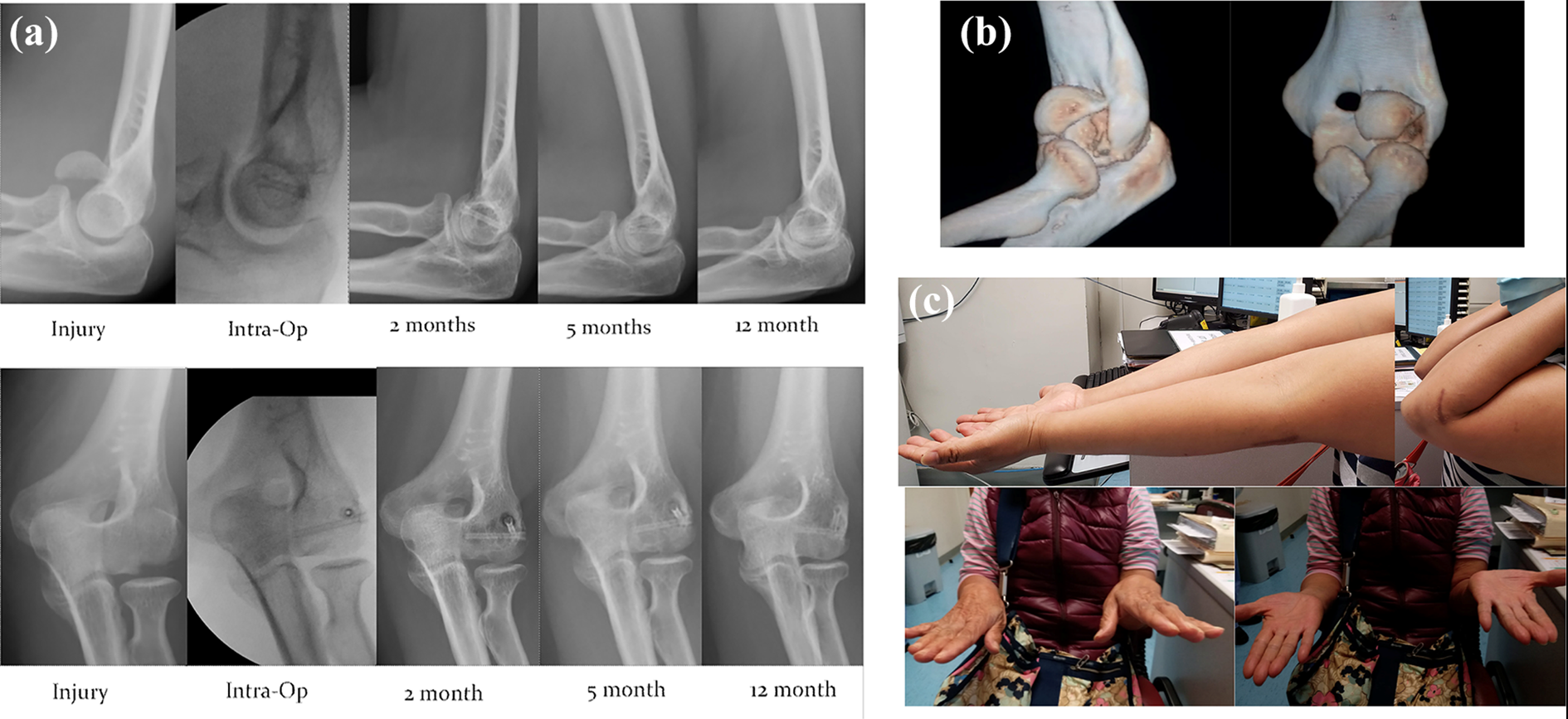
(a) Serial radiologic examination. (b) CT with 3D reconstruction of her right elbow at time of injury. (c) Clinical photo in 1 year post-operation.
Case 2: Bryan and Morrey type 4 capitellum fracture
A 44-year-old, right-handed male, with an unremarkable past health, was admitted for a closed fracture left capitellum. He fell from his bike and landed on his left elbow. An X-ray of his left elbow (Figure 2(a)) showed a capitellum fracture and a double arc sign. A CT scan with 3D reconstruction (Figure 2(b)) showed a type 4 capitellum fracture. Open reduction and internal fixation was performed under general anesthesia. The Kaplan approach to the elbow was adopted. One 2.7 mm Magnezix screw was inserted from lateral-to-medial to fix the trochlea fragment and two more magnesium screws were inserted over the capitellum directly from the articular surface anteriorly toward the posterior cortex. Rehabilitation regime was the same as case 1. He regained a full range of elbow movement with 130° of flexion, 0° of extension, 90° of supination, and 85° of pronation at 2 months post-operation (Figure 2(c)), and his Visual Analog Scale (VAS) pain 0 and DASH score was 1.7. The X-ray of his left elbow indicated some radiolucency at 2 months post-operation, most notably located at the screw head regions, but overall alignment was preserved. Subsequent X-rays of his left elbow showed gradual resorption of screws and loss of the radioluency. Radiologically, the fracture was healed at 5 months postoperatively.
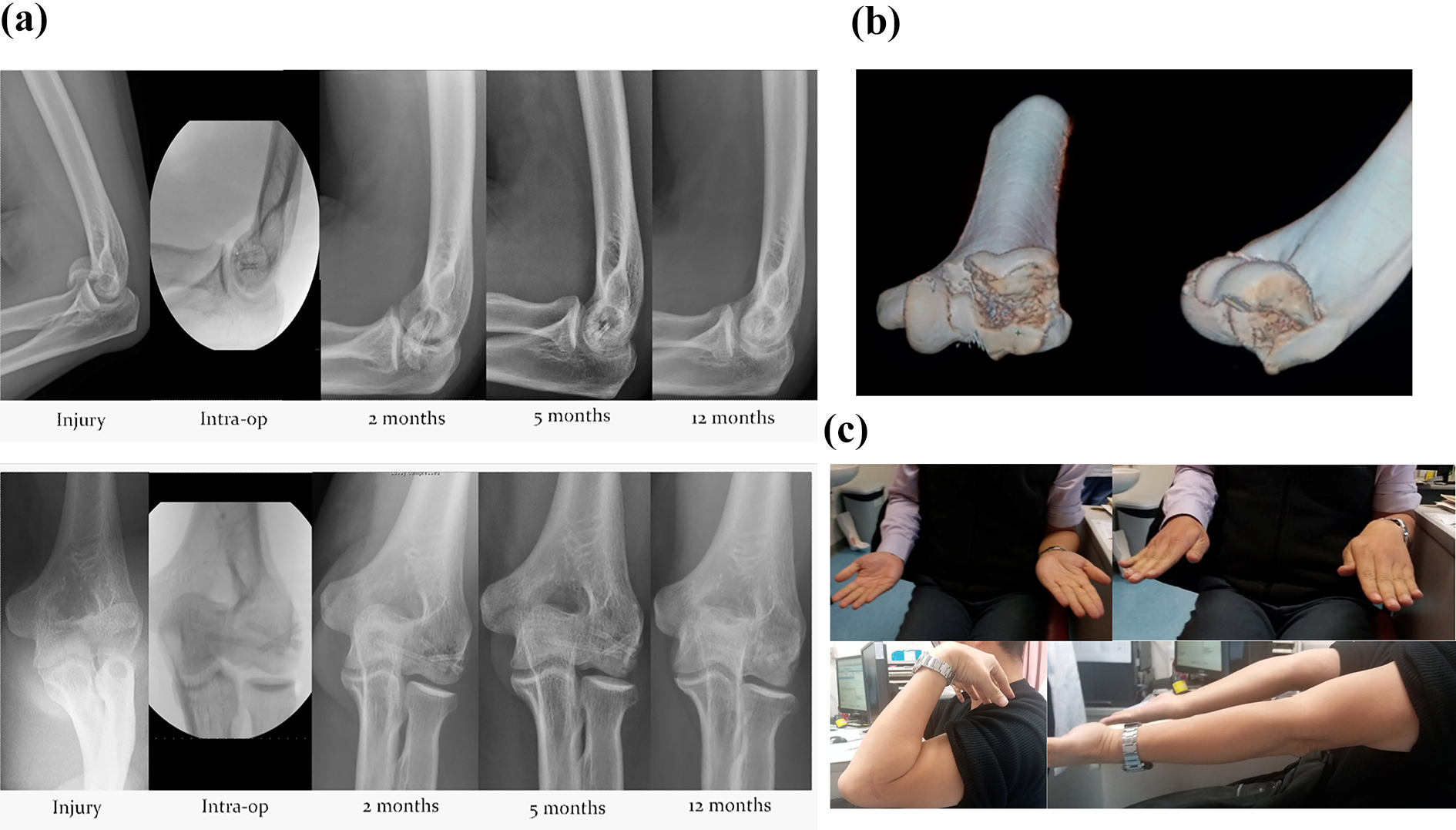
(a) Serial radiologic examinations. (b) CT with 3D reconstruction. (c) Clinical photos at 2 months post-operation.
Case 3: Mason type 2 radial head fracture
A 43-year-old, right-handed male slipped in the bathroom, while on duty, and landed on his outstretched right hand. He was admitted with right elbow swelling and the maximum tenderness was over his radial head. There was a mechanical block with limited flexion range from 20°-60° and limited supination and pronation range of around 30° respectively. An X-ray of his right elbow (Figure 3(a)) showed a Mason type 2 fracture of his right radial head. A CT scan with 3D reconstruction (Figure 3(b)) further delineated the fracture pattern. Using the Kocher approach, open reduction and internal fixation was performed under general anesthesia. Two 2.7 mm Magnizix screws were applied at the subchondral bone, parallel to the articular surface and compression was applied radially to fix each of the depressed fragments toward the intact part. Same rehabilitation protocol to Case 1 and 2 was given. Follow-up examination of his right elbow at 1 year post-operation revealed 140° of flexion, 5° of extension lag, 90° of supination, and 85° of pronation (Figure 3(c)) and DASH score was 0. At 2 months post-operation, an X-ray of his right elbow showed some radiolucency around the screw head, which again disappeared at 1 year post-operation.
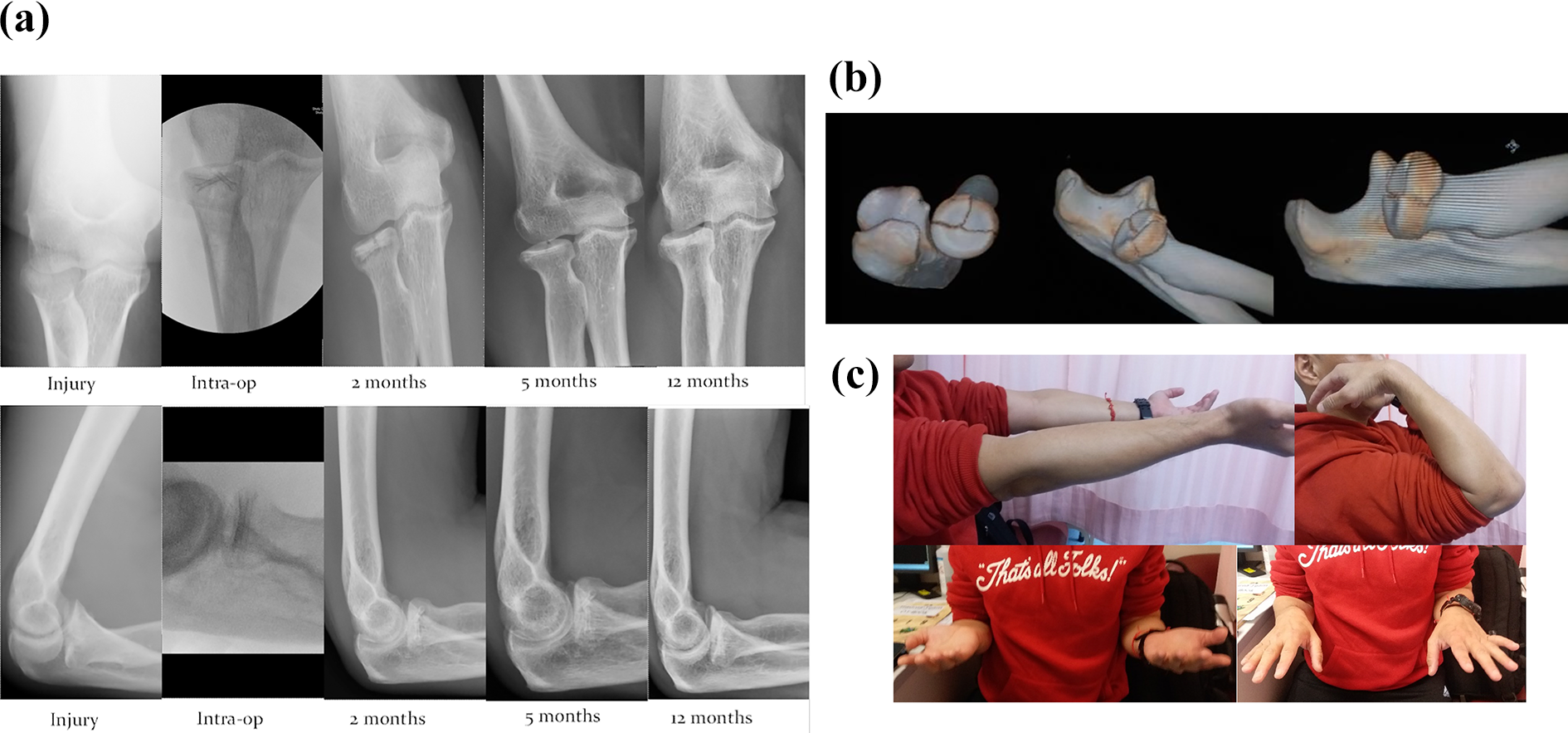
(a) Serial radiologic examinations. (b) CT with 3D reconstruction. (c) Clinical photos in 1 year post-operation.
Discussion
Ideally, a biodegradable magnesium-based orthopedic implant should have a controlled degradation pattern. It should have enough initial mechanical strength to secure the fractured bone firmly in the early healing stages, while degrading at a rate that matches the healing process of the fractured bone. In our clinical cases, direct compression headless screws had been applied from the articular surface toward the subchondral bone without worry of implant impingement. Fracture union was obtained without displacement throughout the follow-up period. Furthermore, no complication occurred, which shows that the magnesium screw is a promising alternative to current orthopedic implants. However, whether the strength of the implants is suitable in all fracture locations still requires more extensive clinical studies.
A radiolucent zone surrounding the magnesium screws was noted on the radiographs of all patients. The phenomenon was most noticeable in the second postoperative month, but gradually reduced in size and completely disappeared, along with fracture consolidation at 1 year post-operation. It did not appear to interfere with fracture healing and there were no corresponding clinical signs or symptoms. Similar radiolucencies have also been reported in other studies. According to Meier and Panzica, five patients with scaphoid fractures were treated with magnesium-based screws. Based on CT scans and X-rays, the authors suspected that cysts were formed in the early postoperative period. In light of this radiological phenomenon, they advised against the use of magnesium screws, although follow-up X-rays showed that all patients achieved fracture union and obtained excellent functional results. 4
Radiolucencies may result from corrosion of the implant during the degradation process. Magnesium screws undergo gradual degradation, which is accompanied by formation of corrosion products and hydrogen. Interestingly, corrosion rates vary even among different parts of the magnesium screw. An in vivo study of magnesium plate and screw degradation revealed that the head of the screw has a significantly higher corrosion rate than the shaft of the screw. 5 This phenomenon was also observed in our cases where there is more radiolucency around the screw head region (Figure 4).
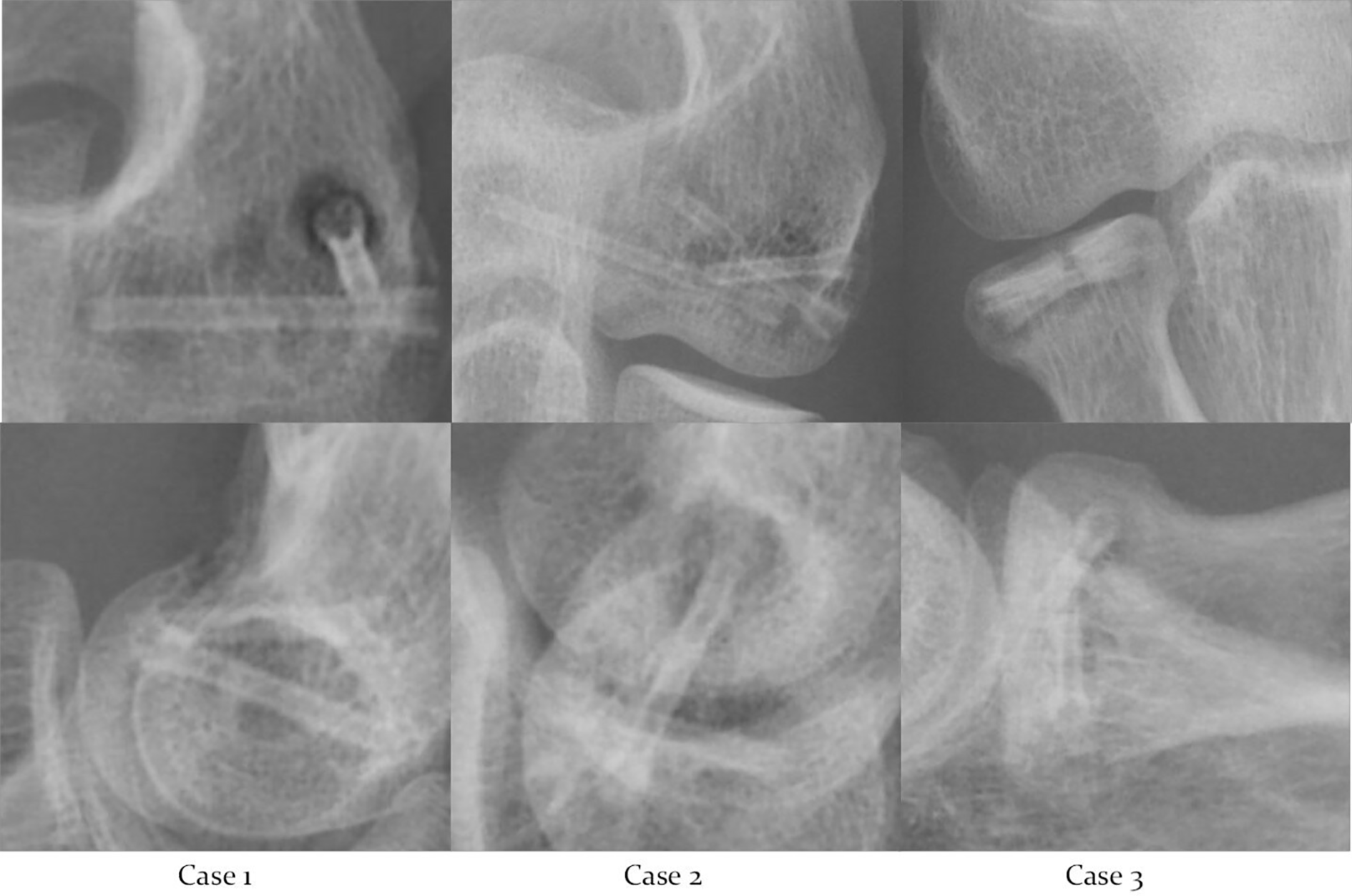
Magnified X-rays of our cases at 2 months post-operation.
Degradation of MgYREZr is known to produce hydrogen, which can form cavities within the tissue and likely accounts for the radiolucency. However, when coupled with the production of magnesium ions, the hydrogen gas, as a novel antioxidant, could prevent osteoporosis while in favors of osteogenesis or new bone formation. 6 As excessive Mg ions travel through the circulatory system and are ultimately excreted in the urine and feces, this has not been reported to pose any adverse effect. 7
Recent studies show that magnesium implants are biocompatabile and even have osteogenic potentials. In fact, comparing the use of magnesium-based intramedullary nails (Mg-IMN) with the use of stainless steel intramedullary nails (IMN) in femoral fracture fixation in rats, the callus in the Mg-IMN-implanted group were significantly larger and wider at 4 weeks post-implantation. 8 In view of these potential benefits, a randomized control trial is ongoing in Germany, comparing the use of magnesium screws with the use of titanium screws in fixation of scaphoid fractures. 9
Currently, the challenge of using magnesium screws is the possibility of degradation before the fracture heals, as fixation failure may occur. An in-vivo study of biodegradable orthopedic screws (MgYREZr-alloy) in a rabbit model showed that the metallic part of the implant degraded by 50% after 12 weeks. In other words, the half-life of magnesium implants is around 12 weeks. 10 Surgeons using this innovative implant should closely monitor the radiolucency surrounding it in the early stage of fracture fixation and focus on loss of reduction, failure of fixation and fracture union. The authors believe when more clinical studies become available concerning the strength of magnesium implants, they may play a significant role for fracture fixation in the future, particularly for the non-weight-bearing regions such as in the upper limb.
Conclusion
This is the first clinical case series in the use of bioabsorbable magnesium screws in the treatment of capitellum fractures and radial head fractures, and results were encouraging. Despite the radiolucency around the screw, it did not appear to impact on early phases of fracture union and there was no loss of reduction or implant failure. There is promising future in the development and clinical application of magnesium implants, especially in upper limb fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval has been obtained for the study (2020.290). This study protocol complied with the Declaration of Helsinki. Informed consent was exempted by the Research Ethics Committee (REC) because of its retrospective study design to review the existing data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.