
Abstract
Background:
A large number of ruptures of the Achilles tendon occurs in the watershed hypovascular region (zone II) of the tendon which is approximately 2–6 cm proximal to the insertion of tendon at calcaneum. Chronic Achilles tendon rupture in the watershed area makes end to end repair of tendon less feasible and the neglected distal stump is often inapt for repair. A number of surgical techniques have been described for repair of chronic Achilles tendon in zone II. Our study was conducted with the objective of determining the efficacy and functional outcome of Bosworth’s technique that involves gastrocnemius-soleus turndown of proximal Achilles tendon.
Materials and Methods:
The study was conducted in a total of five patients with chronic tear of Achilles tendon and the Bosworth technique was used for repair in all the patients. All the patients were followed up for a period of 1 year and the functional outcome was assessed by scoring system devised by Leppilahti et al.
Results:
four out of the five patients showed excellent functional at the end of 1 year follow up. A good functional outcome was seen in one of the patients. All the patients were able to resume work 6 months postoperatively.
Conclusion:
The Bosworth’s technique is an excellent surgical procedure for repair of chronic Achilles tendon rupture in the watershed zone of the tendon.
Introduction
The Achilles tendon despite being the strongest and largest tendon in the human body is most frequently ruptured. 1,2 The cases of rupture of Achilles tendon have seen a substantial rise in yesteryears with approximately 75% of the ruptures associated with recreational and sporting activities. Ruptures though commonly seen in middle aged men (30–50 years) can also occur in the elderly with underlying tendinopathies. 1 The zone II of Achilles tendon (2–6 cm from the calcaneal insertion) which is also the watershed area of the tendon is often involved in ruptures. 1 Acute rupture of the tendon is easily diagnosed clinically although a considerable number of cases are neglected and tend to become chronic. 3 Histological studies have shown that the earliest evidence of chronic healing of tendon is demonstrated at 4 weeks and as such chronic rupture is defined by most authors as rupture of the Achilles tendon that is diagnosed 4–6 weeks after injury. 4 A palpable gap between the tendon ends is elicited during physical examination with the patient complaining of pain, ankle stiffness, inability to raise the heel or climb stairs, decreased plantar flexion strength and fatigue. 1
Chronic rupture of Achilles tendon in zone II poses a wide variety of problems as often the neglected distal stump is not suitable for surgical repair. Also, the wide separation of tendon ends make end to end anastomosis less feasible. Various surgical techniques for repair of the zone II ruptures using tendon transfer, auto graft or synthetic ligament have been described. 5 –7 A number of grafts such as one or more Achilles tendon strips, the fascia lata, local tendon strips such as that of peroneus brevis (PB) or flexor hallucis longus (FHL) have been utilized in surgical procedures. 8 –11 Synthetic materials such as dacron polyster, polyglycol threads, carbon fiber composites have been used as scaffolding for the repair process. 12 Other surgical techniques such as gastrocnemius-soleus turn down of proximal Achilles tendon described by Bosworth and others like Coughlin, end to end repair as in V-Y plasty have also been accentuated upon in literature with the primary goal of restoring the function and strength of gastrocnemius-soleus complex by reinstating the optimal length-tension relationship. 13,14
The prime objective of our study is to determine the efficacy of Bosworth’s procedure in chronic Achilles tendon tear where end to end repair is not possible.
Materials and methods
Patients
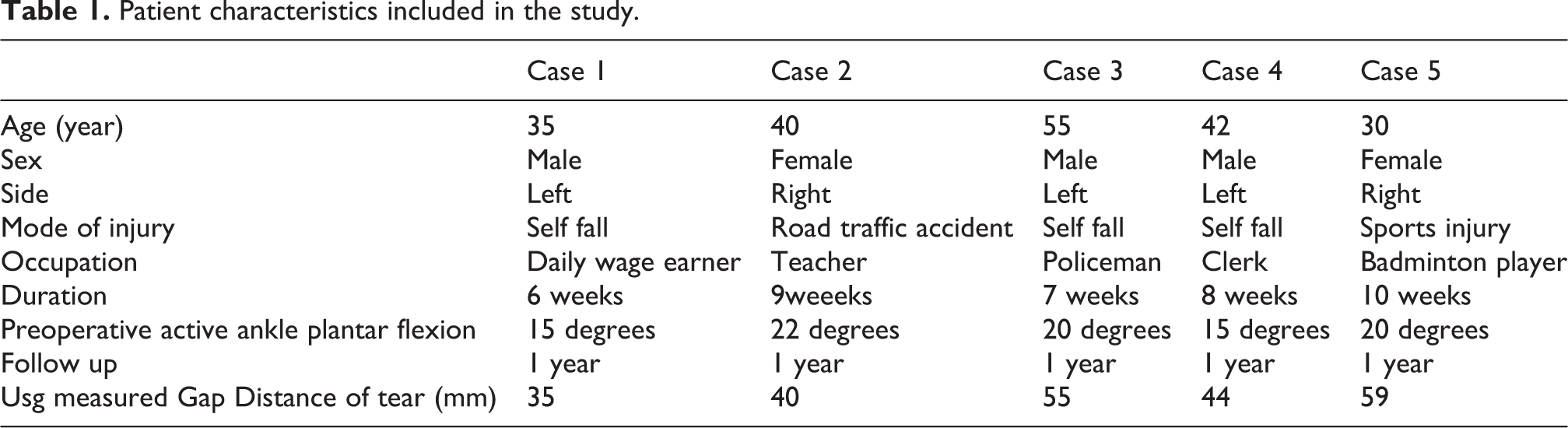
The study was conducted in the Department of Orthopaedics, Gauhati Medical College and Hospital, Guwahati, during 2018 (April–October) after taking institutional ethical clearance. A total of five patients (three male, two female) were included in the study and informed and written consents were taken. Patients were followed up for a period of 1 year (Table 1). All the patients had a positive Thompson’s test (plantar flexion of foot could not be elicited on squeezing the calf). All the patients underwent an USG to document the tear.
Inclusion criteria: chronic rupture of Achilles tendon in Zone II
Exclusion criteria: compound injuries
Patient characteristics included in the study.
Surgical procedure: Bosworth’s technique 13 (a schematic representation of technique is provided in Figure 1)
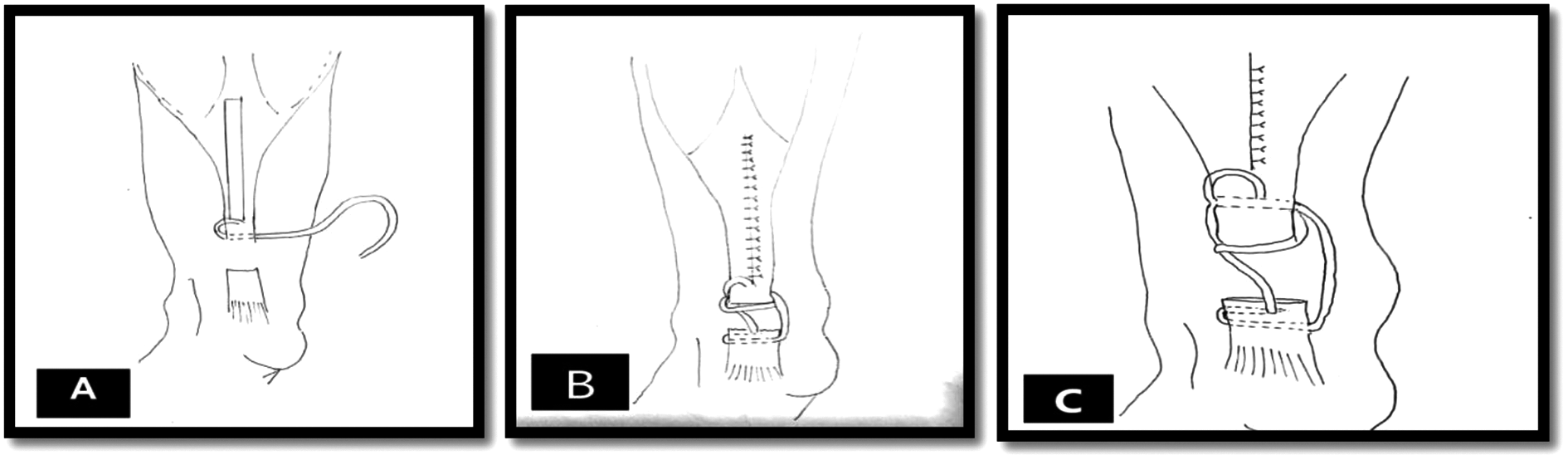
(A, B, C) Schematic diagram illustrating the Bosworth’s technique.
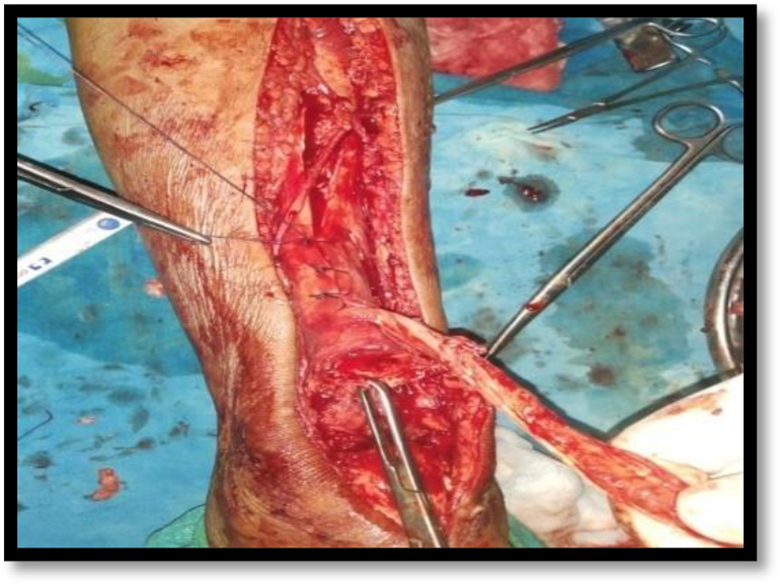
General or spinal anesthesia was given to the patient followed by prone positioning. In the prone position, two bolsters were applied to support the patient; one under the pubic symphysis and the other under the chest. Pneumatic tourniquet was applied on the thigh of the operated site. A posterior longitudinal midline incision was given which extended from calcaneal tuberosity to proximal one third of leg and the ruptured tendon was exposed subsequently. This was followed by excision of scar tissue at the end of tendons (Figure 2). A strip of tendon approximately 1.5 cm wide and about 22.5 cm long was freed from the median raphe of gastrocnemius muscle. This tendon strip was left attached to the proximal site and thereafter turned distally and passed transversely through proximal tendon and anchored there with absorbable suture (Figure 3). The strip was then passed transversely through the distal end of ruptured Achilles tendon and then passed again from this end from anterior to posterior direction. Knee was held in 90 degrees of flexion and ankle in plantar flexion, the fascia strip was drawn tight and anchored with chromic catgut sutures. The strip was then passed proximally and passed transversely through the proximal end of the tendon and thereafter carried distally and sutured on itself (Figure 4). The wound was closed (Figure 5) and a long knee cast was applied with knee in flexion and ankle in plantarflexion.

Excision of scar tissue at tendon ends.
A strip of tendon from median raphe of gastrocnemius harvested and sutured to proximal tendon.

The tendon strip passed through proximal and distal tendons and sutured on itself.

Wound closed in layers.
Post-operative care and follow up
The sutures were removed at 2 weeks and long knee cast with ankle in maximal plantarflexion was continued till 6 weeks. 4 weeks after suture removal (6 weeks after surgery), the above knee cast was changed to below knee cast applied in plantigrade position. The below knee cast with ankle in plantigrade position was continued for another 2 weeks and removed 8 weeks after surgery. Physiotherapy was initiated at this stage and full weight bearing was allowed as per tolerance. Dorsiflexion stretching, slowly graduated resistance exercises were allowed. After 12 weeks, toe raising exercises and proprioceptive exercises were started. Full unrestricted activity was allowed 6 months after surgery.
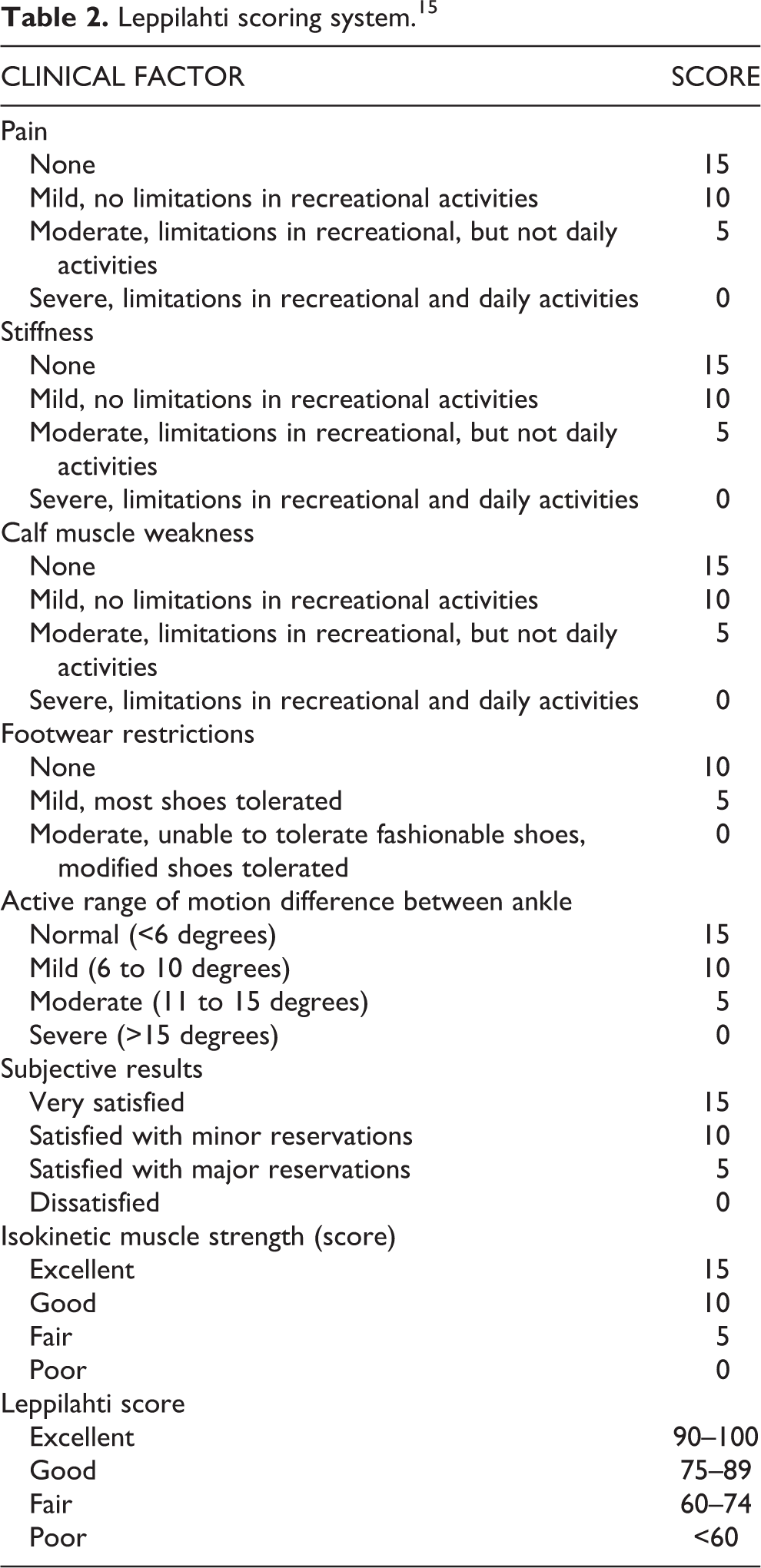
The functional outcome was assessed at 1 month, 6 month and 1 year after surgery in accordance to the scoring system devised by Leppilahti et al. (Table 2). 15 The Leppilahti scoring system includes subjective factors such as pain, stiffness, muscle weakness, footwear restrictions; subjective outcomes along with active range of ankle motion and isokinetic muscle strength. The maximum score of the scoring system is 100 and results can further be graded as excellent (≥90 points), good (75–89 points), fair (60–74 points) or poor (<60 points).
Leppilahti scoring system. 15
Result
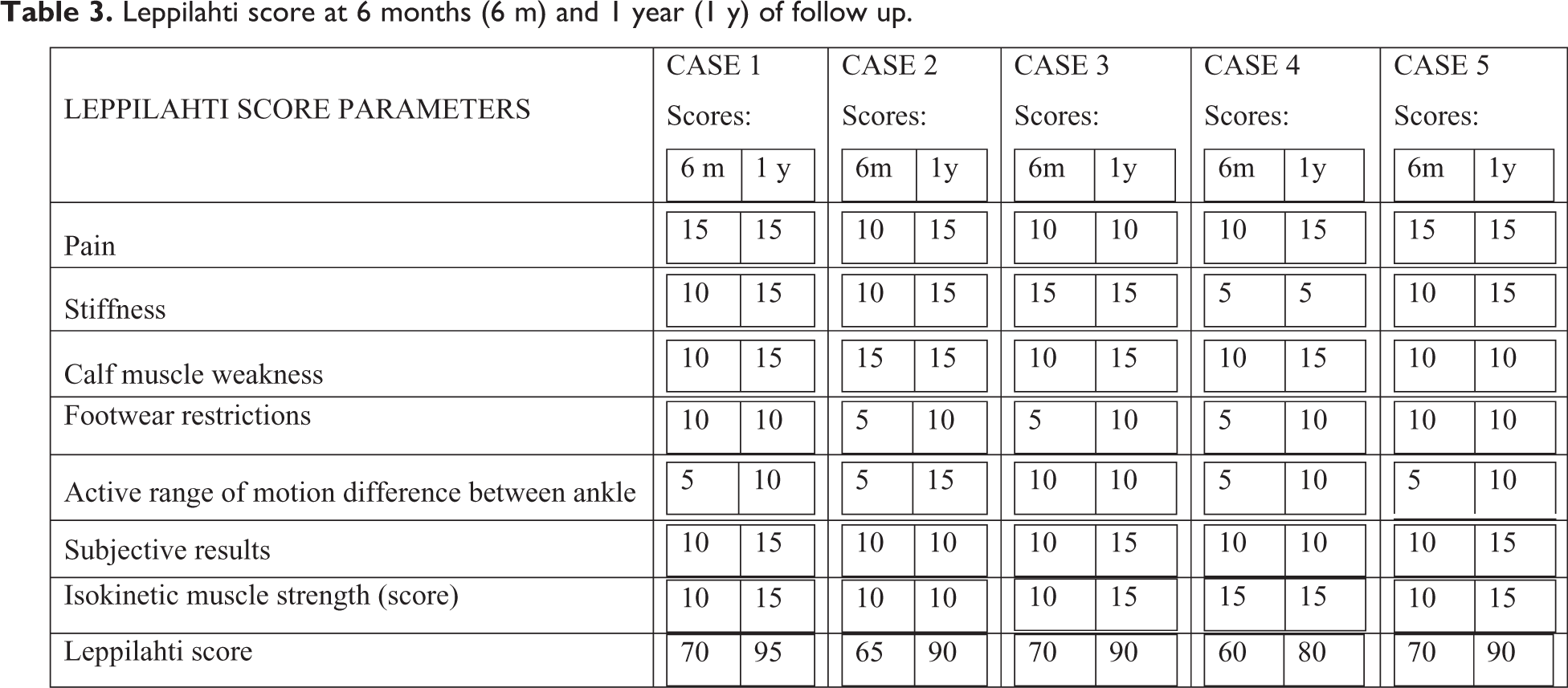
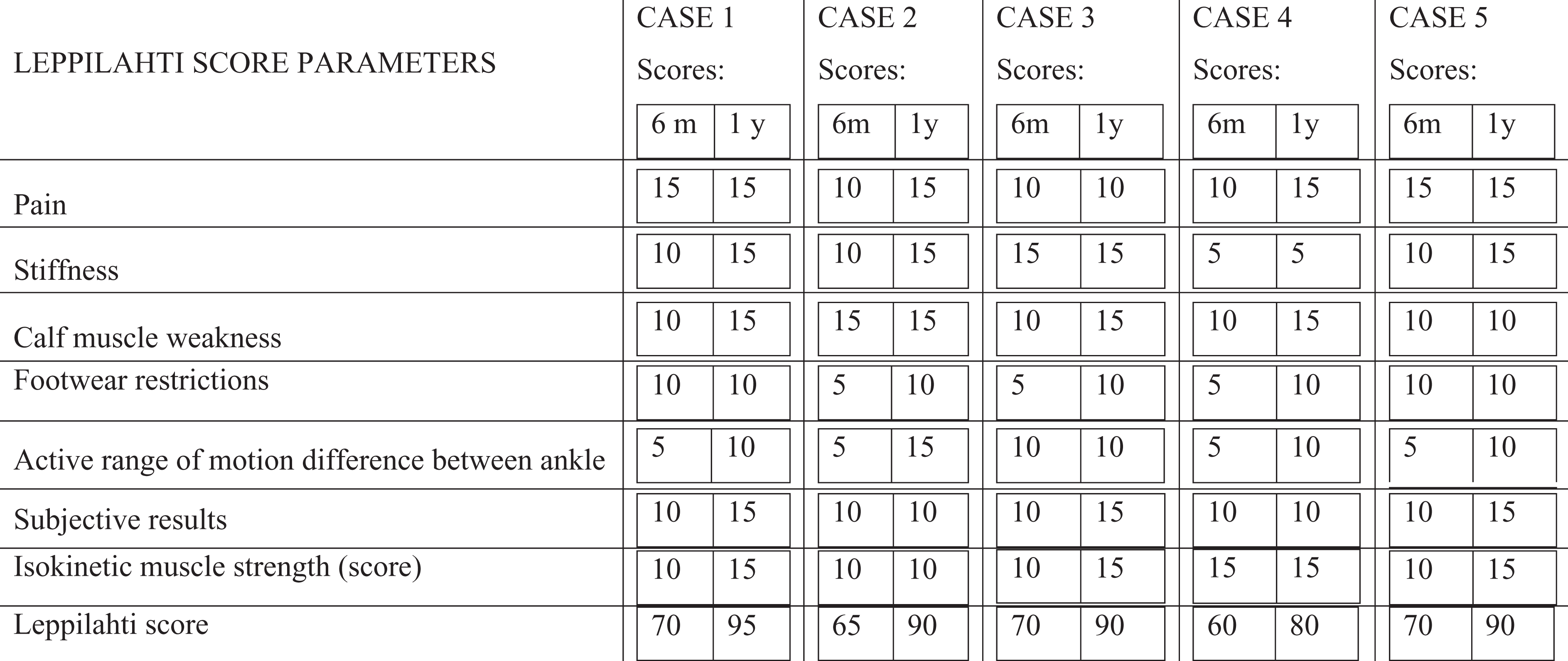
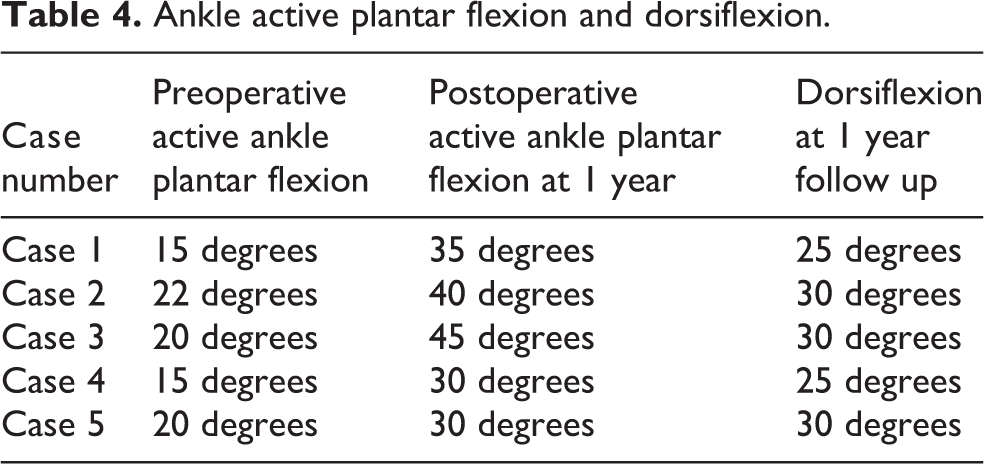
Five Patients (three male; two female) were included in the study. All the patients had chronic rupture of Achilles tendon in the watershed Zone II region and were operated by Bosworth’s technique described above. Out of the five patients, three had rupture of Achilles tendon of left side and two had rupture of the tendon of right side. All the patients were followed up for a period of 1 year. The functional outcome at 6 months and 1 year follow up assessed by Leppilahti scoring system as well as preoperative and postoperative range of ankle motion is depicted in Table 3 and Table 4 respectively. Four out of the five patients had excellent outcome; one had good outcome at the end of 1 year. All the patients resumed work at the end of 6 months postoperatively and all had normal walking and stair climbing. There was a significant improvement in ankle range of motion postoperatively (Figure 6). Only one patient complained of moderate ankle stiffness at the end of 1 year. Complications in our series included superficial infection seen in one of the cases that was controlled with injectable antibiotics and regular dressings. No case of re-rupture was reported in our study.
Leppilahti score at 6 months (6 m) and 1 year (1 y) of follow up.
Ankle active plantar flexion and dorsiflexion.

Active plantarflexion at the end of 1 year follow up.
Discussion
The rupture of Achilles tendon is on the rise and can be attributed to increased sports participation in the recent decades. In 2002, Schepsis et al. observed that the rupture of Achilles tendon is observed in the fourth to fifth decades of life with male to female ratio ranging from 2:1 to 12:1. 16 Activities such as running, sprinting, jumping and agility exercises are the usual mechanism leading to rupture. In our study, all the five cases of rupture had history of ankle trauma which is consistent with the study conducted by Suchak AA et al. in 2005 17 and Ahmed et al. in 2017. 18 Other factors such as chronic degenerative changes in the ankle may also predispose to ruptures. 19 In a study conducted by Maffulli et al. in 1998 and White et al. in 2007, two drugs namely corticosteroids and fluoroquinolones were implicated in delayed healing and necrosis at the site of tendon. 11,20 As high as 25% of cases of Achilles tendon ruptures can be missed on initial presentation owing to lack of pain and an intact active plantarflexion attributable to partial ruptures, recruitment of plantar flexors, and an intact plantaris muscle. 21
A delayed repair or reconstruction is indicated if the posterior heel pain and the functional impairment is disabling. A multitude of Achilles tendon repair options have been described in literature that is mainly guided by the size of defect. Percutaneous suture methods, Krackow technique, Bunnel and modified Kessler techniques can be utilized if the defect is not major. 22 In case of a major gap between the ends of the tendons ruptured, bridging of the gap either by tissue or synthetic material is warranted. For this, Lindholm technique, Bosworth technique, and V-Y repair are popularly done. 13,14,23 For a gap of less than 6 cm, peroneus brevis tendon graft is indicated but if the gap is more than 6 cm a semitendinosus transfer is recommended. 24 Classically, V-Y plasty is appropriate for a loss of 3–5 cm loss and Bosworth’s technique is generally utilized for a defect of greater than 5 cm. 25
Our study utilized the Bosworth’s technique for repair of neglected Achilles tendon tear in zone II and achieved good functional outcomes as 4/5 had excellent results and 1 patient had good functional outcome. Results are in cohesion with studies conducted by Ahmed et al., 18 Agarwal et al. 26 No dreaded postoperative complication were seen in our study although a number of studies have reported variable rates of infection, wound dehiscence. 27 Ascertaining the exact size of the graft to restore the length of tendon can be tricky using the Bosworth’s technique. As it involves flap turndown, there is a potential issue of subcutaneous volume effect in the turndown area that can lead to cutaneous traction in the area causing hindrance in closure of incision. 25 Our study did not utilize any tendon grafts and thereby no tendon function was compromised. In his study on repair of Achilles tendon rupture using flexor hallucis longus tendon graft on eight patients, Wapner et al. observed that the tendon was very thin in diameter and as such inadequate. 8 Likewise tendon transfers using peroneus brevis and flexor digitorum longus poses concerns of loss of eversion strength and weakened flexion of toes respectively. Teuffer described passing the peroneus brevis tendon through the calcaneum across the repair site and suturing it the proximal Achilles tendon. Turco and Spinella modified the technique described by Teuffer by passing the peroneus brevis through the distal tendon stump rather than calcaneum. However, this technique could not replicate the normal medial pull of Achilles tendon and caused eversion weakness. 28,29
The limitations of our study lies in the methodology adopted by us. Comparative studies with a longer duration of follow and larger sample size are warranted to further accentuate upon the efficacy of Bosworth’s technique in repairing chronic tears of tendoachilles.
Conclusion
The Bosworth’s technique is a simple, predictable and reliable procedure to reconstruct the ruptured Achilles tendon with the only limitation of requirement of distal stump. The technique is ideal for zone II ruptures. The non-requirement of additional incisions that may jeopardize nerve and artery in the vicinity, simpler operative technique and excellent functional outcomes give an edge to this procedure over other surgical techniques.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.