
Abstract
Purpose:
One in 10 patients presenting for total hip arthroplasty (THA) will have significant osteoarthritis in both hips. In appropriately selected individuals, one-stage bilateral THA is a treatment option. This study aims to compare outcomes of one-stage bilateral THA with two-stage procedure.
Methods:
A retrospective review of a single surgeon series was conducted comparing One-stage bilateral THA (n = 59) with two-stage bilateral THA (n = 50). The primary outcomes were post-operative complication and the Oxford Hip Score. The secondary outcome was a financial analysis.
Results:
Complications were infrequent and comparable between both groups. Oxford hip scores were slightly higher in the one-stage group. One-staged bilateral THA had a lower cost but hospital tariff is higher for two-stage bilateral THA.
Conclusion:
In appropriately selected patients with bilateral hip arthritis, one-stage bilateral THA gives good clinical outcomes. However, the current payment system in the NHS makes two-stage bilateral THA more financially viable to the hospital.
Introduction
Total hip arthroplasty (THA) has been quoted as the operation of the century. 1 It is one of the most cost-effective interventions performed in medicine and attains one of the best values of cost per quality-adjusted life years (QALY). 2 Over 100,000 THA procedures are performed annually in the UK. 3 The numbers of THA are steadily increasing with significant financial implications on the National Health Service (NHS). 4 The UK National Institute for Health and Care Excellence (NICE) recommends that health care providers adopt cost-effective models for their practice. 5
Approximately one-third of patients with primary osteoarthritis have involvement of both hip joints, and 10% require contralateral hip replacement within 1 year. 6 The current Literature reports various advantages and disadvantages of one-stage bilateral THA. Earlier studies have shown an increased requirement of blood transfusion with one-stage bilateral THA. 7 –9 Two Scandinavian studies have shown superior patient outcomes with one-stage THA in relation to shorter recovery times, better walking capacity and improved Harris Hip Scores (HHS). 10,11 Finally, significantly shorter hospital stay and subsequent lower costs have been reported in an American study with one-stage procedures. 12 A recent analysis utilising UK registry data concluded that one-stage bilateral THA carries a higher risk of complications than staged hip procedures. 13 This conclusion however was only relevant to patients with higher risk (co-morbidities and age) and units performing low case numbers. Further investigation of the safety and effectiveness of one-stage bilateral THA performed within the National Health Service (NHS) in a high-volume unit with an effective enhanced recovery programme is required. In order to control for the variance in both surgeon and unit pathway approaches, a single unit, single pathway, single surgeon analysis is warranted.
The current funding for hospitals in the UK is through payment by results (PBR). 14 Part of the objectives of this financial system is to ensure fairness, to encourage efficiency, and support patient choice. One of the principles of the policy direction states that money should be spent wisely and efficiently. It defines the ‘tariff’ as the new basis of funding for the NHS. These principles comply with and underline the NHS England directive of Getting It Right First Time (GIRFT). 15 It is therefore important to assess the cost-effectiveness of one-stage bilateral THA with regards to the issued tariff.
The aim of this study is to compare the outcomes of one-stage with two-stage (within 12 months) bilateral THA in patients presenting with bilateral hip disease. The primary outcomes were post-operative complications, hospital length of stay and functional scores. The secondary outcome was a cost comparison between one-stage and two-stage bilateral THA.
Methods
A retrospective study was conducted on 109 patients of a single surgeon (SKY). All patients who had bilateral symptomatic hip disease with ASA grade 1 or 2 were offered both the surgical options. Patients’ choice dictated whether one- or two-stage surgery was performed. Between 2012 and 2019, 59 patients underwent one-stage bilateral THA while 50 had bilateral two-stage hip arthroplasties performed within 12 months. Primary and secondary outcomes were compared between the one- and two-stage groups. Cases were excluded if they had previous joint surgery, e.g. dynamic hip screw. The mean time between surgeries was 6.8 months.
Pre-operative radiographs and electronic records were assessed to confirm the presence of arthritis in the contralateral hip before the first surgery in the two-stage group. All surgeries were performed by a single surgeon, through posterior approach and had the same cementless, fully hydroxyapatite (HA) coated titanium stem with an uncemented cup (CORAIL®/PINNACLE®, DePuy Synthes, Leeds, UK). Prophylactic antibiotics and post-operative anticoagulation were similar in both groups. All patients had identical enhanced recovery pathways and discharge criteria. 16 Patients were permitted full weight-bearing immediately post-operatively, and were reviewed at 6 weeks, 1- and 5-year follow-up. Pre-operatively patients with a Hb level of less than 120 mg/dL were treated medically prior to surgery. The post-operative protocol for initiation of blood transfusion was a Hb of 70 mg/dL or symptomatic requirement. No post-operative heterotrophic ossification (HO) prophylaxis was administered.
The operative time was calculated in both groups to include anaesthetic and surgical time. Post-operative complications are reported in terms of pre and post-operative haemoglobin levels, the need for blood transfusion, incidence of chest infection, acute kidney injury (AKI), deep vein thrombosis (DVT) and pulmonary embolism (PE). The 1-year radiograph was used to assess for the presence of HO with classification according to Brooker et al. 17 The Oxford Hip Score (OHS) was used to evaluate patients reported functional outcomes at 1-year post-surgery. Mean OHS are presented post both surgeries in the two-stage group. The length of hospital stay (LOS) was calculated in days, from the day of surgery to discharge from the hospital; no patients were discharged to rehabilitation facilities. The combined hospital stay for both episodes in the two-stage group is presented.
Statistical comparison of patient demographics, OHS and LOS were performed using paired t-tests (Mann Whitney U test). The chi-square analysis (2 × 2 table) was performed to assess differences in gender. Statistical analysis was performed using SPSS Statistics for Windows software (SPSS Inc., Chicago, Ill., USA) with a significance level of p = <0.05.
The cost calculation included the theatre cost, the cost of the prosthesis and the day rate for in-patient stay. The appropriate tariff was applied for each surgery and used for the financial assessment (Market Forces Factor 2019/20). The total cost was deducted from the given tariff for both procedures to calculate the hospital’s net income.
Results
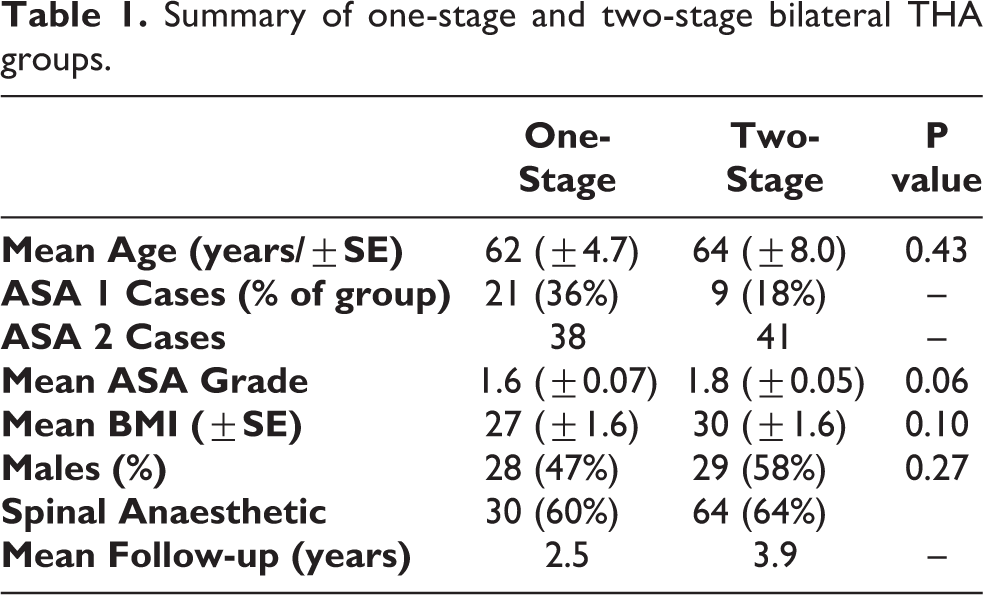
During this period 8.7% of patients presenting for THA had both sides done within a year in our hospital. Patient characteristics of the two groups were comparable with a slightly higher but non-significant mean age, ASA grade and BMI for two-stage group (Table 1). Operative time for the two-stage group (two episodes combined) was 33% higher compared to the one-stage operative time.
Summary of one-stage and two-stage bilateral THA groups.
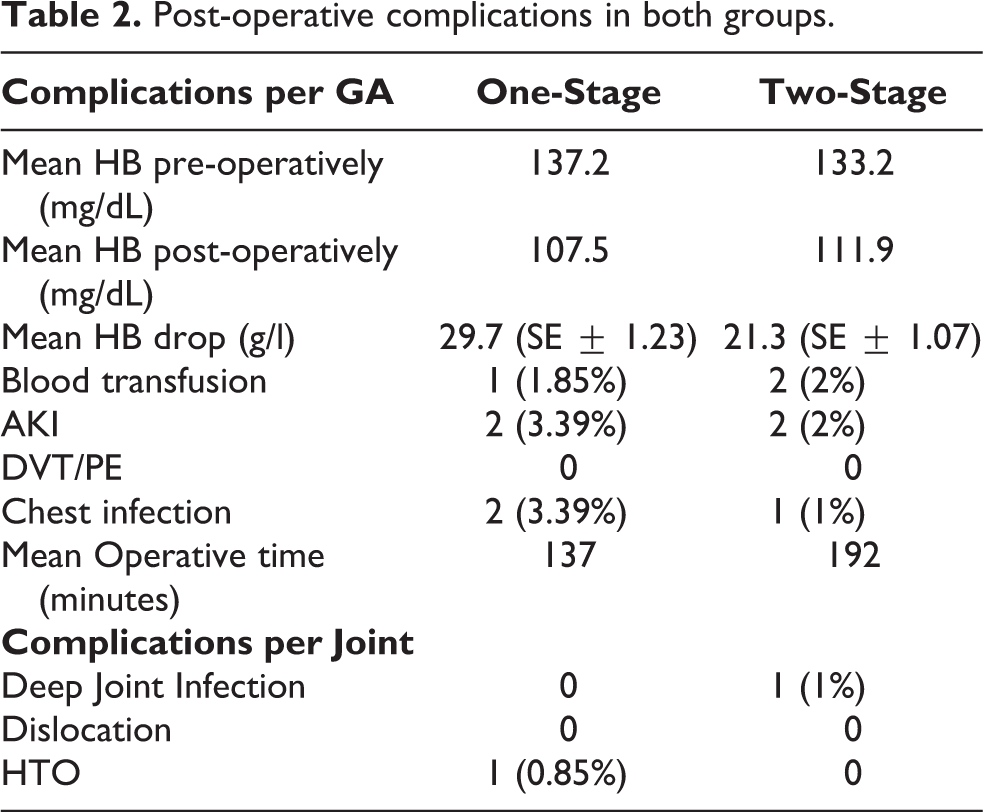
The complication rate between the two groups was comparable (Table 2 and 3). Despite a significantly higher mean HB drop in the one-stage group (p value 0.0001), only one patient required blood transfusion compared to two patients in the two-stage group. A total of four patients developed AKI, evenly split between the two groups. There was one case of deep infection in the two-stage group and one case of heterotopic ossification (Brooker stage II) 17 in the one-stage group. There were no dislocations, DVT, PE, intensive care unit admissions, or mortalities recorded.
Post-operative complications in both groups.
Details of complications encountered.
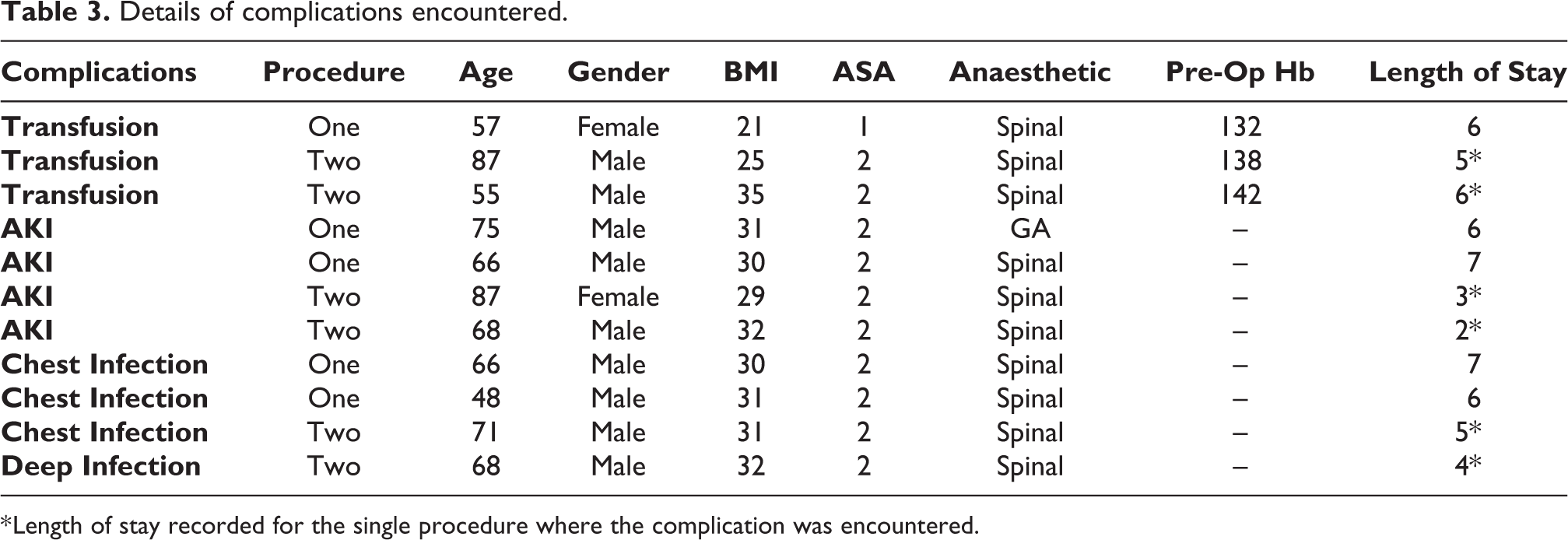
* Length of stay recorded for the single procedure where the complication was encountered.
The mean OHS in the one-stage group was 43.7 (31–48). In the two-stage cohort, the mean OHS following the first THA was 39.5, and 40.2 following the second THA. The mean OHS for two-stage THA is significantly lower than the one-stage THA, 39.8 compared to 43.7 (p = 0.018; Mann Witney U Test) (Figure 1).
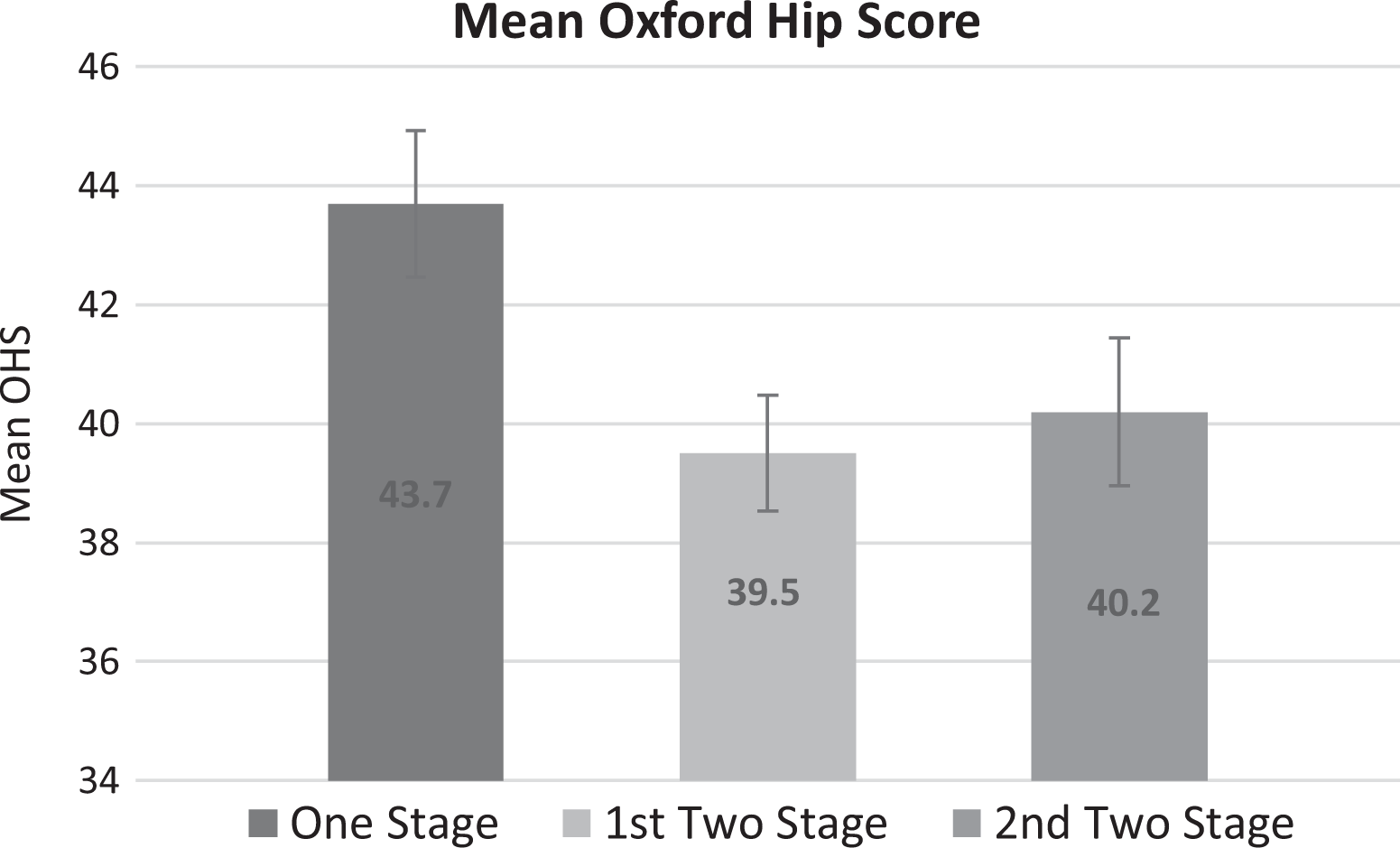
Mean Oxford hip score for both groups.
In the two-stage cohort, the mean LOS for the first procedure was 3.1 days, and 2.6 days for the second procedure. The mean LOS was significantly shorter in the one-stage group (3.9 days ±1.6) compared with two-stage group (5.7 days ± 4.6), p = 0.007 (Figure 2).
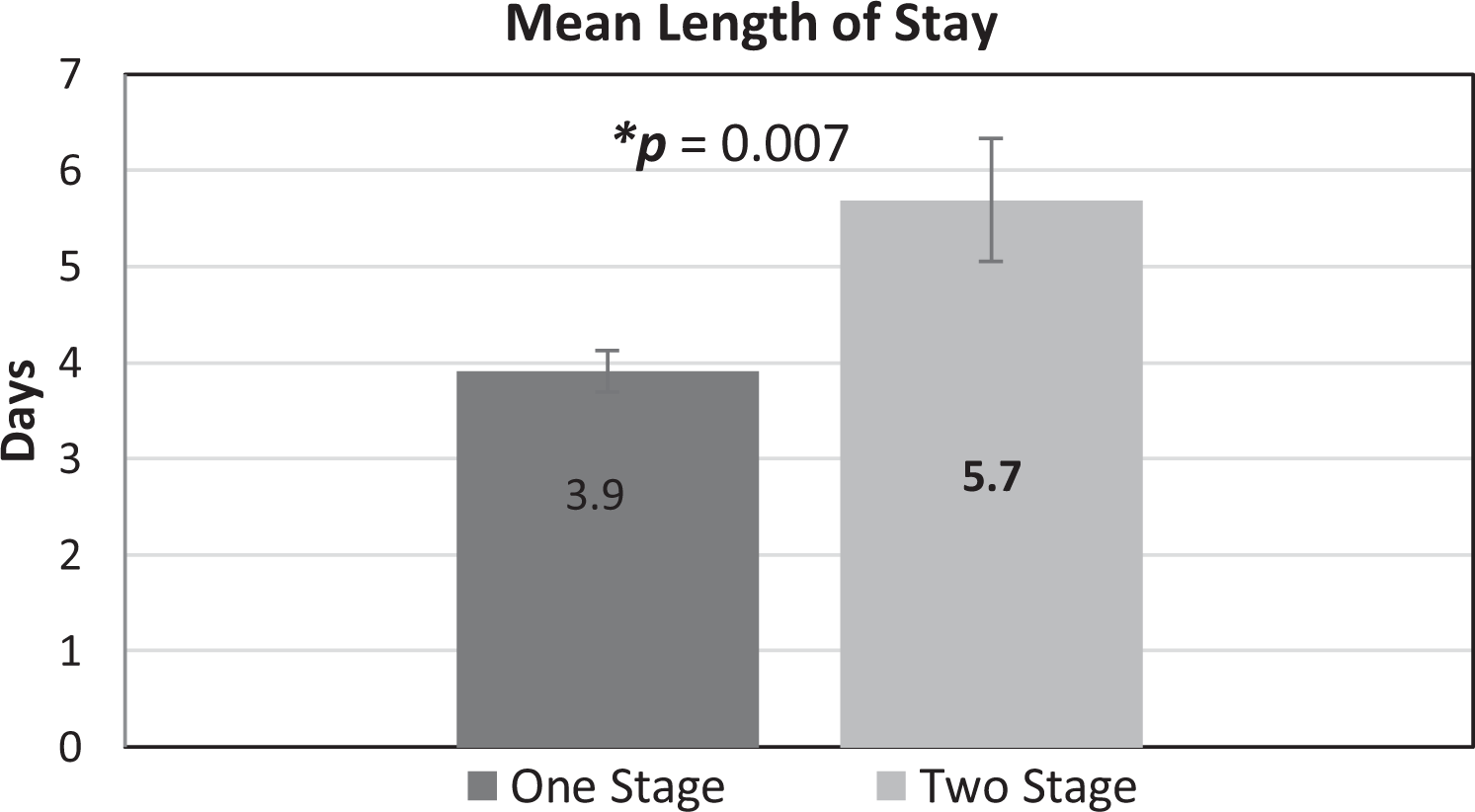
Mean length of stay for both groups (two-stage THA; combined hospital stay for the two episodes).
The calculated total cost of one-stage bilateral THR was £8,633 compared to £11,373 for two-stage bilateral THA. These figures included the prosthesis cost, ward cost, theatre cost, and other expenses (Table 4). The cost reduction is £2,740 in favour of one-stage procedure. The mean tariff for one-stage bilateral THA was £8,683 compared to £12,828 for two-stage bilateral THA. The current tariff and costs generate an excess of £50 for one-stage bilateral THR in comparison to an excess of £1,455 for the two-stage bilateral THR. Consequently, making one-stage bilateral THA a more cost-effective but less profitable procedure.
Breakdown of costs as per tariff.
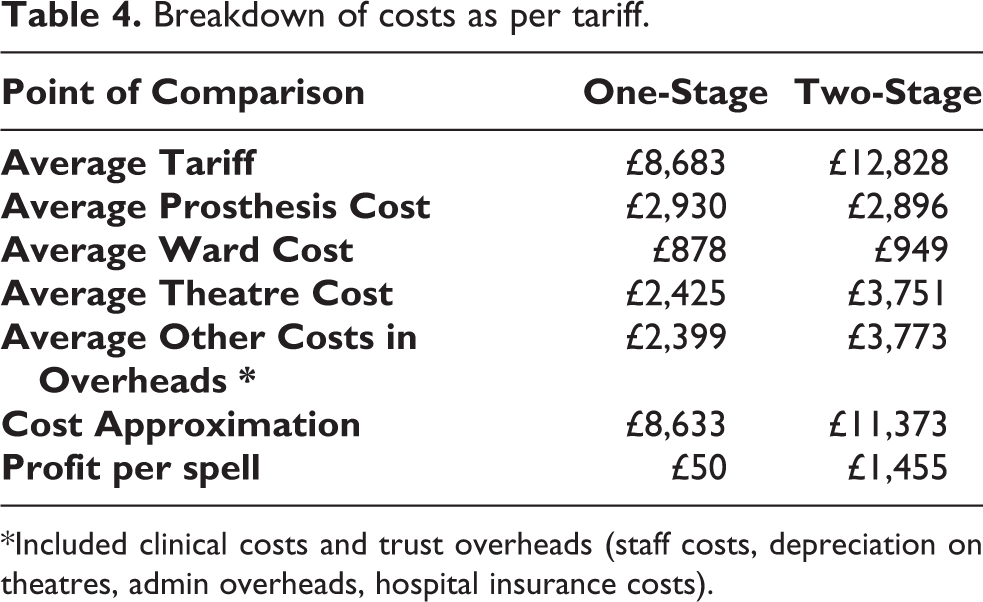
*Included clinical costs and trust overheads (staff costs, depreciation on theatres, admin overheads, hospital insurance costs).
Discussion
Bilateral one-stage total hip replacement was historically considered with caution due to concerns of increased risks for perioperative complications. 18 More recent literature however has shown good outcomes and comparable complication rates. 10 –12 This change is likely a result of advances in anaesthesia, operative technique, and early mobilisation post-operatively. 19 Our findings are in line with the recent reports concluding no increased risk of complications in low risk patients (ASA grade 1–2) from high-volume units. 13,20 –22 A recent study utilising national registry data concluded one-stage bilateral THA in higher risk patients (older age and greater co-morbidities) from low volume units (<5 cases per year) had significantly higher complication rates compared to two-staged surgery (separated by 3–6 months). 21 The authors of this study acknowledge they did not report the type of anaesthetic, length of procedure, blood loss, or transfusion rate, which may have influenced the risk of cardiac events, renal failure, and chest infection. Furthermore, the mean length of stay reported in this study for both single and two-stage surgeries was over 9 days, more than double that reported in our study. This demonstrates a considerable difference in the pathway management of this patient group. Moreover, this paper used the ‘Charlson co-morbidity index’ (CCI) to grade patient general health status. This prognostic mortality indicator does not account for some co-morbidities such as hypertension. The CCI is not routinely used in practice in the UK and has recently been demonstrated not to be comparable at predicting 12-month mortality in hip fractures and it is not a valid alternative to ASA grading system. 23 For example, patients with some co-morbidities which are not included in the CCI may be considered low risk, while with using the ASA system the same patient may be considered as high risk. Therefore, it may not be possible to infer from these results in practice or to compare co-morbidity status between CCI and ASA grades.
Our study supports the safety of single-stage bilateral THA in appropriately selected patients as long as the operating surgeon and the centre is performing the procedure in adequate numbers and if there is a well-developed enhanced recovery pathway in use in order to manage this patient group appropriately. The complication rates reported in our cohort are comparable to a recent report of unilateral THA through the same surgical (posterior) approach. 24
Tan et al. reported blood transfusion rate to be five times higher in the one-stage bilateral THA group (50% vs 10%). 25 This difference is possibly a result of cases with more significant co-morbidities, as the one-stage cohort had 14% cases with an ASA grade of 3 or 4 compared to 8% in the two-stage THA group. In our cohort of one-stage bilateral THA we report considerably lower rates of blood transfusion in comparison to Tan et al., this may be explained in that all cases in our study were low risk (ASA 1 or 2) and the standard usage of other perioperative measures like hypotensive anaesthesia, infiltration of local anaesthetic with adrenaline and IV Tranexamic acid in our protocol. Although there was a greater HB drop in the one-stage group, transfusion rates were comparable, most likely due to the fact that the mean pre-operative Hb level was high enough to not require a blood transfusion.
In this study we have only included low risk patients (ASA 1 and 2). Despite a discrepancy in ASA grades for the cohort, the subgroup analysis revealed that the complications encountered were more prevalent in ASA 2 cases for both one-stage and two-stage procedures. In ASA 2 cases, the one-stage group complications occurred in 4 out of 72 joints (5.6%) compared to six complications in 82 joints (7.3%) in the two-stage group. In ASA 1 cases, there was only one complication in the one-stage group (42 joints), this was a requirement for blood transfusion due to persistent bleeding from the surgical site with no predisposing co-morbidity. While there was no complications occurring in ASA grade 1 in the two-stage group (18 joints). This demonstrates a comparable complication rate for one- or two-stage procedures when independently considered relative to the ASA grade. There was also a trend for complications to be more prevalent in males and in older patients.
The functional outcomes assessed using the Oxford Hip Score shows a trend for superior outcomes at 1 year in the one-stage procedures. Length of hospital stay was significantly shorter in the one-stage group (p = 0.07). The reduction of LOS contributed to a considerable decrease in the overall costs. The mean LOS for unilateral THA in our hospital was 2.8 days. This is shorter than the mean LOS reported in the literature in the UK. 26 In this series, using identical enhanced recovery pathways for both groups, one-stage THA led to a reduced overall LOS in comparison to two-stage surgery
In most studies, there is a direct cost saving by reduction in length of stay comparing one-stage THA with a cumulative length of stay for two-stage THA. However, the way hospitals get incentivised for these procedures can have significant impact on the profitability of the hospitals. This is apparent in literature demonstrating contrasting cost-benefit outcomes around the world. For example, in China, Tan et al. found no difference in cost between one- versus two-staged bilateral hip replacements. 25 In America, there is conflicting evidence, with one study showing no difference in the total episode cost, 27 whereas two other studies concluded cost savings with bilateral one-stage hip arthroplasty. 12,28 A Canadian study comparing one- with two-stage bilateral THA, all performed through a direct anterior approach, found a significant cost saving in the one-stage group bilateral THA group. 29 Financial superiority with a one-stage approach has also been reported in Korea with bilateral THA through two-incision minimally invasive technique. 30
The cost of surgery in this study was significantly lower in the one-stage bilateral THA group; cost based on the length of stay, prosthesis, and theatre cost. This cost reduction benefit has been proven in other studies. Despite this cost-benefit for the one-stage THR, when the costs are deducted from the tariff for each procedure the two-stage procedure becomes financially more profitable for hospitals in the UK. Tariff for bilateral two-staged THR in patients with ASA 1 or 2 was £12,828 and the average cost was £11,373. This generates £1,455 profit for the hospital. Despite the total cost of one-stage THR reduced by 24% (£2740) per patient compared to two-staged surgery, the net margin we report for two-stage bilateral THA is £1405 greater than for one-stage bilateral THA (£1,455 versus £50). This may discourage some centres from adopting the one-stage practice and consequently increasing the overall costs to the NHS. Increasing the tariff to a rate that would achieve equal incentive for hospitals to offer one-stage bilateral THR to eligible patients would result in a positive impact on lowering the overall cost of treatment and bed space demand on hospitals for this commonly performed surgery.
A secondary benefit that was not equated in the cost analysis of this study is the utilisation of the reduced total anaesthetic and operative time which was 55 minutes shorter in the one-stage procedure. Furthermore, an even greater cost reduction may be reflected in the socioeconomic effect in the community with shorter rehabilitation, faster recovery, and early return to work. This may be particularly important in the younger population in full time employment. In this study, over two thirds of the patients were under the retirement age at the time of surgery. With only one episode of leave from work, one can calculate, based on UK national sick pay rate of £94.25, that taking 6–12 weeks off work only once would save between £565.50 and £1,131 for employers. Perhaps more critically, it would reduce the time patients were away from work and not earning their regular salary.
The limitation of this study is that the costs and tariffs change on a regular basis and depend on the activity volume. This may have implications on the exact figures published in this work. However, these changes occur in both groups and are relatively subtle. Therefore, it would have not significantly changed the considerable difference between the two compared surgical options. A second limitation to this study is that intra-operative blood loss was not recorded. We report pre-operative Hb levels, collected at their pre-operative appointment 4–6 weeks prior to surgery. This may permit a degree of error in HB drop calculations that are reported. Another limitation is that this study was retrospective with no pre-operative Oxford scores and only included patients with low risks (ASA 1 and 2). Since not all studies support the safety of one-stage bilateral THR in high risk patients, further research is needed to confirm its outcomes and study the cost-effectiveness in this patient group. In addition, further research is required to reveal the advantages of the earlier return to work after one-stage bilateral THR in patients below retirement age. A prospective, multi-centre randomised control trial with an adequate sample size to ensure the appropriate statistical power is the next step in determining if one-stage bilateral THA is effective and efficient in a modern-day health service is thus warranted. Our study acknowledges its limitations with regards to sample size, however we believe the strengths of a single surgeon comparison from a single high-volume centre with patients following the same pathway and discharge protocol gives confidence and value to our conclusion.
In conclusion, this study shows that bilateral uncemented one-stage THA is safe and provides good functional outcomes in patients with low risk and presenting with bilateral hip disease in a high-volume unit. It reduces the length of hospital stay and consequently the overall costs however this may not be cost-effective since the tariff is less for one-stage bilateral surgery. It may be reasonable to increase the tariff for bilateral one-stage surgery to encourage more centres to offer this for patients in order to reduce the costs to the NHS.
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by MH, FS, AU,PS, and SY. The first draft of the manuscript was written by MH and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.