
Abstract
Extrusion of bone is a rare situation in open fractures due to high energy trauma. There are few studies, reporting successful reimplantation of the extruded bone segment using various sterilization and fixation protocols. However, there are no definitive treatment strategies for this challenging situation. We report a case of 30-year-old male patient with grade IIIB compound right distal femur fracture with an extruded long bone segment, who was treated with successful sterilization and immediate reimplantation of an extruded long diaphyseal segment of distal femur following extensive cleaning with sterile normal saline, removal of debris with scrubbing by sterile brush, soakage in the broad-spectrum antimicrobial solution for 30 min, sterilization by autoclaving at 121°C for 45 min, and reimplantation during stable internal fixation with lateral distal femur locking plate using Arbeitsgemeinschaft für Osteosynthesefragen techniques. At 3 months, iliac crest bone grafting, osteoperiosteal flaps, and augmented fixation with a medial locking plate were performed through a subvastus approach for a void in the medial supracondylar femur region. Intraoperatively, punctate bleeding was observed from the reimplanted fragment. Infection was ruled out with normal leukocyte count, C-reactive protein marker, no evidence of unhealthy granulation tissue, and a sterile culture report from the fracture site. The fracture healed in 12 months and the patient had good functional outcome with a lower extremity functional score of 80% and knee range of motion of 110° at short-term follow up of 2 years without any complication. Decision of reimplantation is individualized depending on the time of presentation, contamination, and comminution of extruded fragment with scarce literature on standard treatment strategies. In our case, early presentation, meticulous debridement, unique sterilization technique, immediate reimplantation, and augmented dual distal femur plating with bone grafting aided in achieving successful union with good functional outcome and knee range of motion, avoiding any complications.
Keywords
Introduction
High-energy compound distal femur fractures with bone loss is a challenging situation for the orthopedic surgeon especially when an extruded long bone segment has been retrieved from the vicinity of the accident. This situation faces difficult decisions in terms of reimplantation of extruded bone fragment or delayed limb reconstruction. Principle management consists of thorough irrigation of the wound, meticulous debridement, and removal of devitalized soft tissue and bone. 1 Various reconstructive methods like bone transport, cancellous bone grafting, free fibula strut grafting, and vascularized fibular grafting have been described for the management of bone large bone defects. 2 –6
Discarding a large bone segment results in a significant shortening of the limb and will need a lengthy limb reconstruction surgery, which is also a financial burden to the patient. There are certain benefits and risks with the reimplantation of an extruded contaminated large bone segment. Benefits include maintaining the skeletal and soft tissue length, avoiding the morbidity of prolonged treatment with bone transport. 7 The major risk includes infection in an already elevated infection risk associated with open fractures, which can be avoided by meticulous debridement of the wound, complete removal of devitalized musculoskeletal unit, and adequate sterilization technique for contaminated extruded bone and immediate reimplantation. Due to the rarity of this situation, there are no strategies for the reimplantation process. However, there are various case reports, describing various methods of sterilization with a 10% povidone–iodine solution, 8 2% chlorhexidine, 9 4% chlorhexidine, 7 and subcutaneous bone pouch. 10
We report our experience of immediate sterilization and reimplantation of two extruded bone segments in grade IIIB compound distal femur fracture with the successful union and good functional range of motion without infection and shortening. A written informed consent was taken from the patient regarding publishing the case information and was informed regarding the need of publishing this case report.
Case report
A 30-year-old male presented to our emergency department 4 h after a road traffic accident when his motorcycle rammed into a heavy vehicle. He was conscious on arrival with stable vitals. Clinical and radiological findings confirmed Gustilo-Anderson type IIIB compound right distal femur fracture with articular comminution and significant diaphyseal bone loss of approximately 12 cm (Figure 1(a)) and 5 × 4 cm2 wound over the anterior aspect of the distal thigh (Figure 1(b)) without any neurovascular compromise. The wound was initially sutured elsewhere with a superficial saline wash. He suffered with no other injuries. Two extruded contaminated bone segments measuring 8 × 3 cm2 and 10 × 5 cm2 were brought wrapped in cloth by the relatives found on the road at the accident scene (Figure 2). After initial evaluation and stabilization in the emergency room, the patient was given intravenous antibiotics (cefuroxime 1.5 g, amikacin 750 mg, and metronidazole 500 mg), tetanus toxoid, and tetanus immunoglobulin. Minimal wound contamination, age of the patient, no comorbidities, and timing of presentation favored our decision for immediate reimplantation. While the patient was being prepared for the surgery, sterilization procedure for the extruded bone segments was started. Bone segments were thoroughly cleaned with a sterile surgical brush and irrigated with normal saline for 30 min. It was then soaked in a sterile container containing broad-spectrum antimicrobial solution (isopropanol 45% and 1-propanol 30%) for 30 min. The thoroughly cleaned bone segment was then autoclaved at 121°C for 45 min. On completion of this process, the patient was taken for the surgery. During the intraoperative period, there was minimal contamination of the submuscular region and adjacent to the bone. The sample was taken to assess for any microbial contamination, which was negative for any growth after 48 h of incubation. The initial surgery consisted of meticulous debridement, removal of devitalized soft tissue and bone, and thorough irrigation of the wound with 9 L of normal saline. Bone segments were reimplanted and fixed with shaft using interfragmentary screws, the articular surface was restored, and fracture fragments were stabilized with 4.5-mm lateral precontoured locked plate using Arbeitsgemeinschaft für Osteosynthesefragen (AO) techniques (Figure 3). The wound was primarily closed over a negative suction drain.
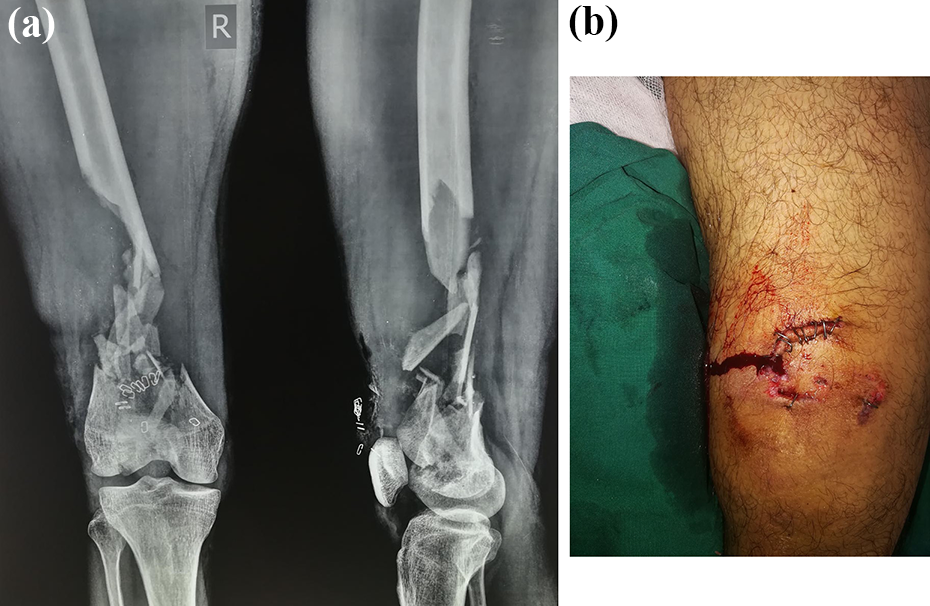
(a) Right distal femur fracture with articular comminution and significant diaphyseal bone loss of approximately 12 cm. (b) 5 × 4 cm sutured wound over anterior aspect of distal thigh.

Two extruded contaminated bone segments wrapped in cloth.
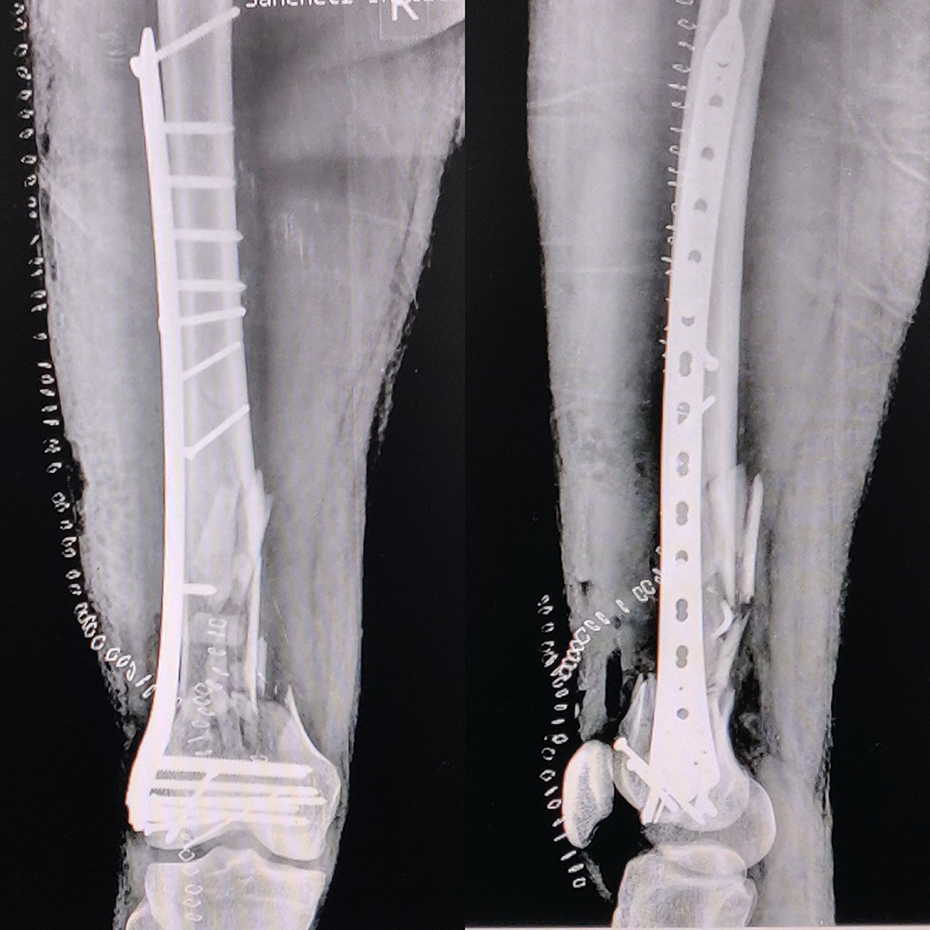
Immediate postoperative radiograph showing fixation using AO techniques.
Postoperatively, antibiotics were given as follows: intravenous cefuroxime 750 mg thrice daily, intravenous amikacin 750 mg once a day, and intravenous metronidazole 500 mg thrice daily for 1 week, and then, oral cefuroxime 500 mg twice daily for 2 weeks. He was observed for any local and systemic signs of infection. Postoperative knee range of motion and quadriceps activation was started on postoperative day 2. Nonweight-bearing walking was initiated and the patient was discharged after a week with no signs of local infection. Suture removal was done on postoperative day 14. At 3 months, radiographs showed improvement in callus formation, incorporation of the reimplanted fragment to shaft but with a void in the medial supracondylar femur region (Figure 4). At this stage, the patient was advised bone grafting and augmentation of medial supracondylar femur region through a subvastus approach. Infection was ruled out as a potential cause of this delayed healing with normal leukocyte count, C-reactive protein marker, no evidence of unhealthy granulation tissue intraoperatively, and a sterile culture report from the fracture site. Osteoperiosteal flaps were raised proximally and distally. Proximally, punctuate bleeding was observed from the reimplanted bone fragment, indicating revascularization and viability of the fragment. Cortico-cancellous iliac crest bone grafting was performed and the medial column was augmented with 3.5-mm reversed lateral proximal tibial locked plate with proximal screws into the reimplanted fragment (Figure 5). Active knee exercises and partial weight bearing were started on postoperative day 1 and the patient was discharged 3 days later. Suture removal was done postoperative day 14. The patient was followed up regularly to assess the union status and any signs of infection. Radiographs at 12 months follow-up showed complete union with the incorporation of reimplanted bone segments to the shaft and distal fragments and well reconstructed medial and lateral columns (Figure 6). The patient was able to walk independently without the support and had a good functional outcome with a lower extremity functional score of 80%. He had a knee range of motion of 0–110° without any signs of local infection at the final follow-up of 2 years (Figure 7).

Radiograph at 3 months showing incorporation of reimplanted bone fragments with shaft with void in the medial supracondylar region.
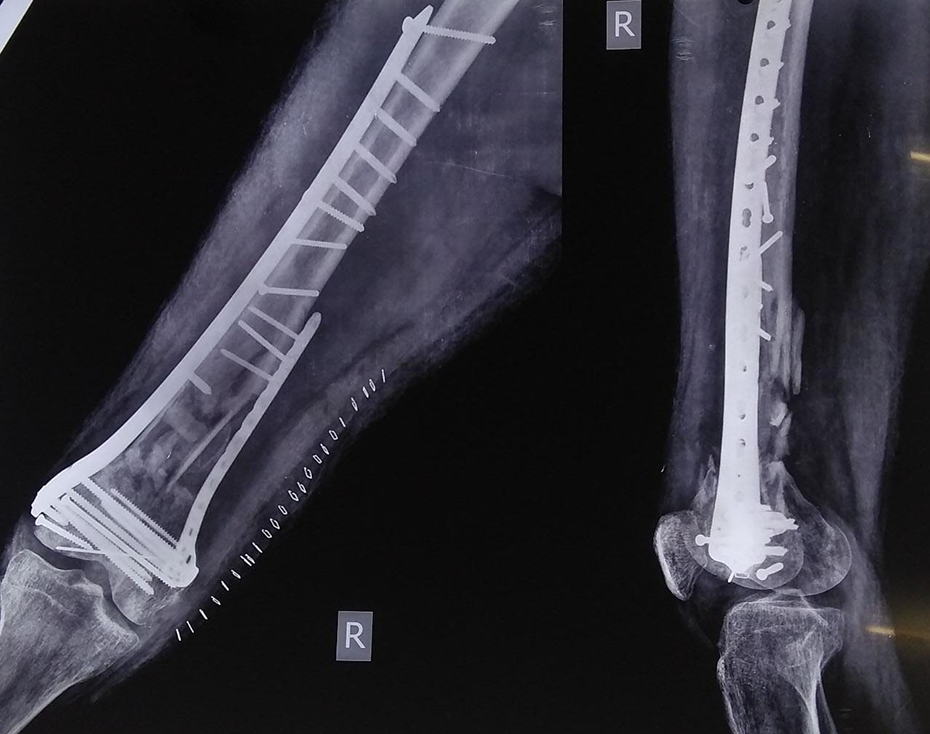
Radiograph after iliac crest bone grafting and augmentation of medial column with reversed lateral proximal tibial locked plate.

Radiographs at 12 months showing complete union and incorporation of reimplanted bone segments to the shaft and distal femur.

Knee range of motion at 2 years follow-up.
Discussion
Open fractures with extruded bone fragments with bone loss is a rare and challenging situation for the trauma surgeon. This situation involves the decision making in terms of assessment of contamination of the extruded bone, sterilization process, timing of reimplantation, and modality of fixation. Ilizarov ring fixator or limb reconstruction system, fibular strut grafting, cancellous or cortical bone grafting are the conventional methods of managing bone defects, 11 –14 however, discarding long segment of reimplantable bone leads to significant limb shortening requiring lengthy procedures for limb reconstruction, the morbidity of bone grafting procedures, and financial burden to the family. Masquelet and Begue developed a two-staged antibiotic cement spacer and induced membrane bone grafting for the management of long bone defects, which is conventionally utilized mostly for infected gap nonunions. 15 Kasha et al. showed good results with the union in all cases with Masquelet’s technique in the treatment of 28 open fractures with bone loss. However, they do mention that a long time to the union is a limitation. 16 Induced membrane technique comes with its own complications like pseudoarthrosis, hardware migration and irritation, and toe clawing, as reported by Mühlhäusser et al. 17
The benefits of reimplanting extruded fragments are anatomic reduction, maintaining musculoskeletal tissue length and avoiding lengthy bone transport procedures. 7 Alternatively, Lindvall et al. showed the “autosterilization” effect by placing the devascularized bone fragments in a sterile subcutaneous location other than the traumatized region and found it to be a safe procedure in series of eight cases. 10
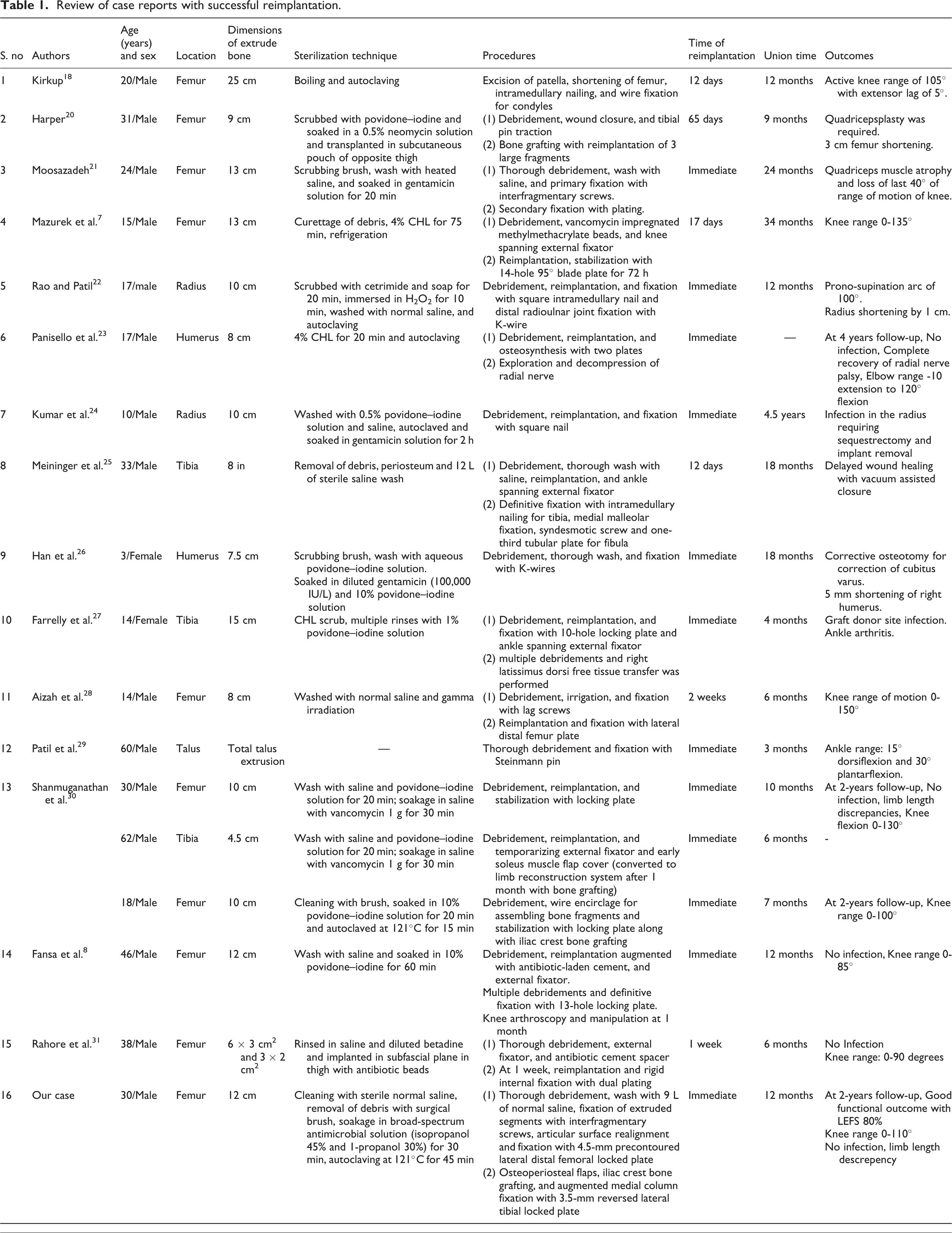
A most important step in the management consisted of thorough irrigation of the wound, meticulous debridement, and removal of devitalized soft tissue and bone. 1 Kirkup was the first to report on the reimplantation of extruded femoral bone fragment. 18 Large-free fragments have been used to achieve an anatomic reduction in reimplantation surgeries, as advocated by Barei et al. 19 Since then, several authors have described their experiences with different sterilizing techniques like boiling, autoclaving, gamma irradiation, and soaking with 2% and 4% chlorhexidine, 10% povidone–iodine solution and antibiotic solution. However, there is no universal treatment strategy and method of sterilization for reimplantation. Current literature suggests a case-based approach to various sterilization processes and the timing of reimplantation. Table 1 summarizes the case reports of successful reimplantation with a wide variety of sterilization techniques, the timing of reimplantation and fixation protocols. In our case, bone segments were thoroughly cleaned with a sterile surgical brush and irrigated with normal saline for 30 min, soaked in a broad-spectrum antimicrobial solution (isopropanol 45% and 1-propanol 30%) for 30 min, and then autoclaved at 121°C for 45 min. This process is an alternative to those reported in the literature and further studies are needed to prove its superiority over others.
Literature in Table 1 reports the timing of reimplantation ranging from immediate within hours to 65 days after injury. We preferred immediate reimplantation since our patient presented within 4 h of the injury.
Review of case reports with successful reimplantation.
Supracondylar femur fractures with medial bone loss are particularly at risk of delayed healing, nonunion, and a collapse in varus with lateral implant failure. 32 In our case, the fragments incorporated proximally to the shaft at 3 months, as shown in the radiograph with a void in medial supracondylar femur region, which is a known entity in distal femur fractures. To prevent the above complications and accelerate fracture healing, we followed the current indications of bone grafting laid down in the literature that supports iliac crest bone grafting for structural support, particularly in the medial supracondylar femur region that is recommended 4–8 weeks after injury prior to the diagnosis of a definite nonunion. 32 Infection was ruled out as a potential cause of this delayed healing with normal leukocyte count, C-reactive protein marker, no evidence of granulation tissue intraoperatively, and a sterile culture report from the fracture site.
The most feared complication of reimplantation is infection. The extruded fragments are prone to devastating infections especially due to contamination, which allows bacterial adhesion and colonization. Kumar et al., Meininger et al., and Farrelly et al. reported infection and delayed wound healing in their cases requiring subsequent secondary procedures for reconstruction. 24,25,27 We believe that infection in our case was avoided by meticulous initial debridement, unique sterilization technique, and immediate reimplantation complemented by empirical intravenous antibiotics.
Summary
Given a rare situation with an extruded long segment in open fractures, the decision of reimplantation is individualized depending on the time of presentation, contamination, and comminution of an extruded fragment. In our case, meticulous debridement, unique sterilization technique, immediate reimplantation, and augmented dual distal femur plating with bone grafting aided in achieving successful union with good functional outcome and knee range of motion, avoiding the risks of infection. Further studies are required to validate this unique sterilization protocol in similar compound fractures with an extruded bone fragment.
Author’s recommendations
Given that there is no adequate evidence for the best treatment strategy for decontamination of the extruded bone fragment, we recommend the following steps in managing similar cases based on the available literature through case reports/series: Most important standard surgical step is thorough irrigation of the wound, meticulous debridement, and removal of devitalized soft tissue and bone. Evaluation of the extruded bone fragment for contamination and comminution (to assess for adequacy of structural integrity). Adequate cleaning of the extruded bone fragment with surgical brush (to remove the foreign bodies), irrigation with sterile saline for 30–45 min, and disinfecting with any one or combination of bacteriocidal agents like povidone–iodine, antibiotic concentrated solution, and chlorhexidine or isopropanol for another 30–45 min. Adequate sterilization by autoclaving at 121°C for 30–45 min. Immediate reimplantation within 18–24 h of injury. Extruded bone segments can be autosterilized in subcutaneous bone pouch for delayed reimplantation up to 1 month. This delay can be utilized for the reimplantation versus limb-salvage decision. Decision on mode of fixation (internal vs external) can be made based on the contamination and size of the wound. Following antibiotic prophylaxis is recommended: intravenous cefuroxime 750 mg thrice daily, intravenous amikacin 750 mg once a day, intravenous metronidazole 500 mg thrice daily for 1 week, and then oral cefuroxime 500 mg twice daily for 2 weeks. In the case where delayed healing is anticipated, biological augmentation procedures like bone grafting can be performed at 8–12 weeks from the index surgery. Salvage procedures are recommended in cases of compound fractures with bone loss with severe comminution and delayed infection.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.