
Abstract
Adhesive capsulitis (AC) is a painful and debilitating condition of the glenohumeral joint and has been described as self-limiting. However, recent reports suggest that up to 40% of patients report persistent symptoms, therefore intervention strategies are needed to improve function and quality of life. One such intervention is the hydrodilatation of the glenohumeral joint with a high-volume injection, comprising of local anaesthetic, corticosteroid and normal saline, making a total volume of up to 40 ml. This service evaluation assessed the outcomes in 28 patients (23 females and 5 males; mean age 54.29 years) with AC who underwent ultrasound-guided (USG) hydrodilatation in a clinical outpatient setting. There was a statistically significant improvement in pain and all shoulder movements (all changes p value < 0.01). No adverse effects were encountered. Therefore, the USG glenohumeral joint hydrodilatation procedure in a clinical outpatient setting is a safe and effective intervention for AC.
Background
Adhesive capsulitis (AC), also referred to as ‘frozen shoulder’ and ‘pericapsulitis’, is characterised by progressively worsening stiffness and inflammation of the soft tissues of the glenohumeral joint, resulting in symptoms of localised pain and restricted active and passive range of motion (ROM). 1 The most common form of the condition is primary AC, which manifests insidiously in patients with an unknown pathogenesis. 2 Alternatively, secondary AC can develop in patients as a result of joint diseases such as osteoarthritis, or following an acute injury to the shoulder joint. 3 Typically, AC presents clinically with three distinct phases – an early painful phase known as ‘freezing’, an intermediate stiff phase known as ‘frozen’ in which the pain is less pronounced and, finally, a recovery phase known as ‘thawing’ where movement is gradually restored. 4 The duration of specific phases often differs on an individual basis, with some studies reporting a self-resolution of overall symptoms within 2 years. 5 However, more recent reports have documented the condition remaining beyond 3 years, with up to 40% of patients experiencing persistent symptoms. 3 Despite much research and advocation for treatment modalities such as corticosteroid injections, mobilisations and acupuncture, optimal management protocol for AC is not clearly defined, with no specific guidelines for clinicians to follow when faced with a patient. 6 The current proposed management protocol is illustrated in Figure 1.
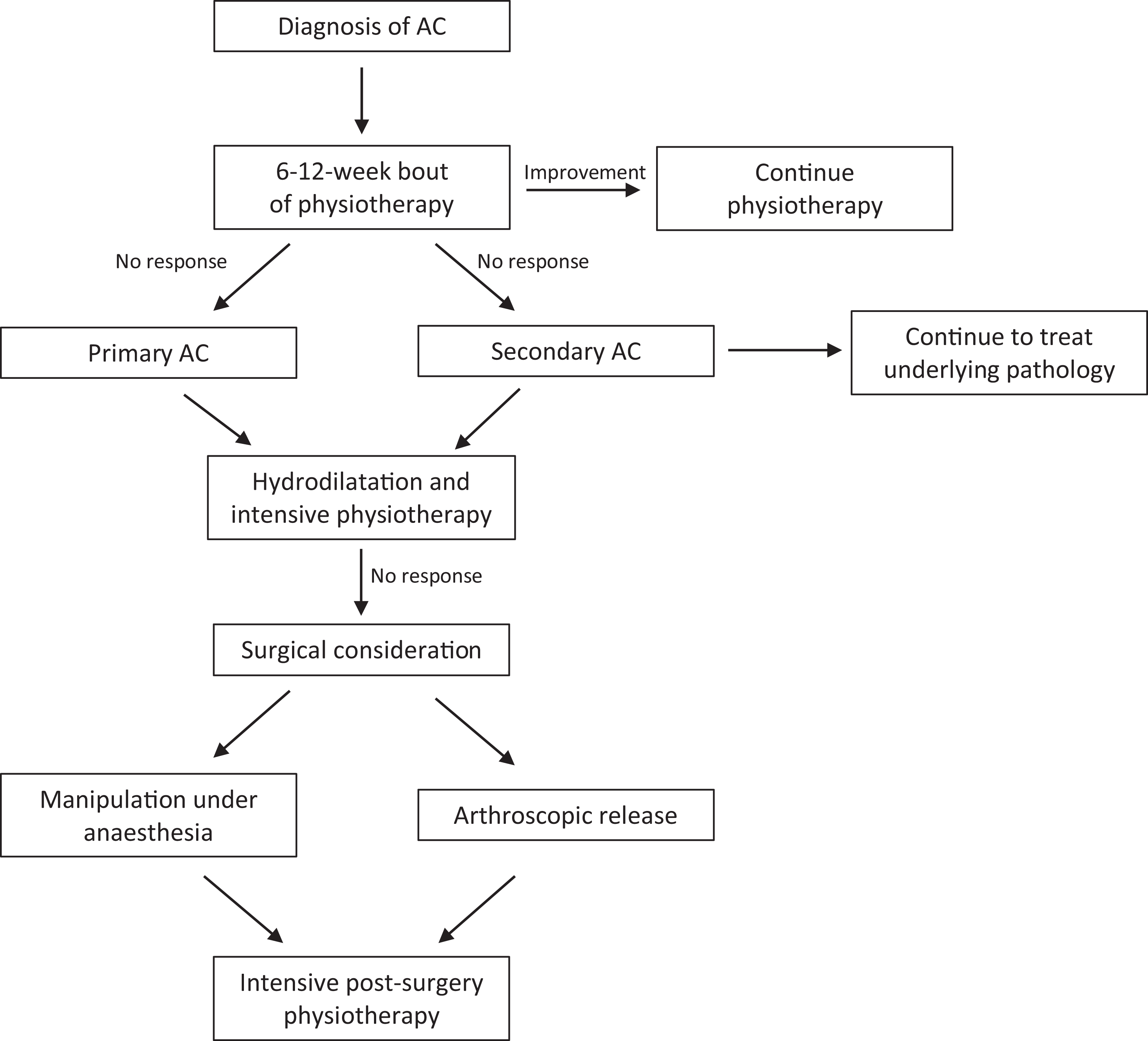
A flow chart depicting the suggested treatment protocol for AC, adapted from Robinson et al. (2012) 2 AC: adhesive capsulitis.
The hydrodilatation procedure is a high-volume intra-articular injection consisting of around 10–90 ml of solution, which includes local anaesthetic, corticosteroid and saline. 7 The procedure is commonly employed as non-surgical intervention following an unsuccessful bout of conservative treatment, often being favoured due to the ability to be performed in an outpatient setting. 2 It is increasingly becoming a common procedure across National Health Service (NHS) practices and can be performed either under fluoroscopic or under ultrasound guidance. The proposed mechanism of action is the mechanical distension of the joint space, ideally rupturing the tight, fibrotic joint capsule that develops during AC. 6 Moreover, hydrodilatation is more cost-effective than common surgical intervention strategies, only costing approximately £280 compared to around £1440 and £2200 for manipulation under anaesthesia and arthroscopic capsular release, respectively. 8 This means a significantly lower economic burden on health-care providers and surgical waiting lists if similar outcomes can be achieved. Cost estimates were calculated from a combination of the material and procedure costs.
This service evaluation aimed to determine the safety and efficacy of ultrasound-guided (USG) hydrodilatation procedures on pain and shoulder ROM in patients with AC of the shoulder in an outpatient clinical setting. Researchers also wanted to assess whether age, diabetes status and duration of symptoms influence the outcomes of pain, shoulder ROM or requirement for further intervention following hydrodilatation, as these factors have not yet been established.
Methods
This was a retrospective service evaluation study of patients seen in the musculoskeletal service of the NHS community health-care trust. Data on USG hydrodilatation procedure carried out by a single clinician (MS) were recorded over an 18-month period. Patients with a clinical diagnosis of AC were referred to the clinician by extended-scope physiotherapists when not responding to ROM exercises and steroid injections in some cases. The diagnosis of AC was confirmed by clinical examination and ultrasound examination in clinic by MS. A total of 39 patients underwent the USG hydrodilatation procedure over an 18-month period, however, follow-up data were available only for 28 (23 female, 5 male) of these patients, with 11 patients being lost to follow-up. Repeat procedures were considered for patients who did not exhibit improvements during the 6-week follow-up, with surgical intervention considered for patients with worsening symptoms or those who underwent multiple hydrodilatation procedures. A summary of baseline patient characteristics can be seen in Table 1.
Baseline characteristics and measures of 28 patients with AC.
SD: standard deviation; AC: adhesive capsulitis.
The inclusion criteria for the USG hydrodilatation procedure included an unsuccessful bout of conservative treatment lasting at least 6 weeks, debilitating pain and restricted shoulder ROM in ≥2 planes, no contraindications such as an allergy to local anaesthetic or anticoagulant therapy. Pain scores were recorded before the procedure and upon follow-up using patient-reported pain on the numerical rating scale (NRS) scores. Shoulder flexion, abduction, external rotation and internal rotation were also measured to the nearest 5° by MS before the procedure and upon follow-up using a manual goniometer.
The patients were placed in the lateral lying position, and the procedure was performed via a posterolateral approach. On ultrasound imaging, the borders of the humeral head and infraspinatus tendon are used to identify the joint capsule which appears as a white triangle in between the structures. This can be seen in Figure 2. Then, 2 ml of 1% lignocaine (local anaesthetic) was used for skin anaesthesia. A 22-gauge needle was used to gain access to the joint capsule, and hydrodilatation was performed with a solution consisting of 40 ml of normal saline, 40 mg of kenalog (corticosteroid) and 2 ml of 0.25% marcaine (local anaesthetic). The procedure lasted until all of the solution was injected into the joint, or if the patient was under too much pain to continue.
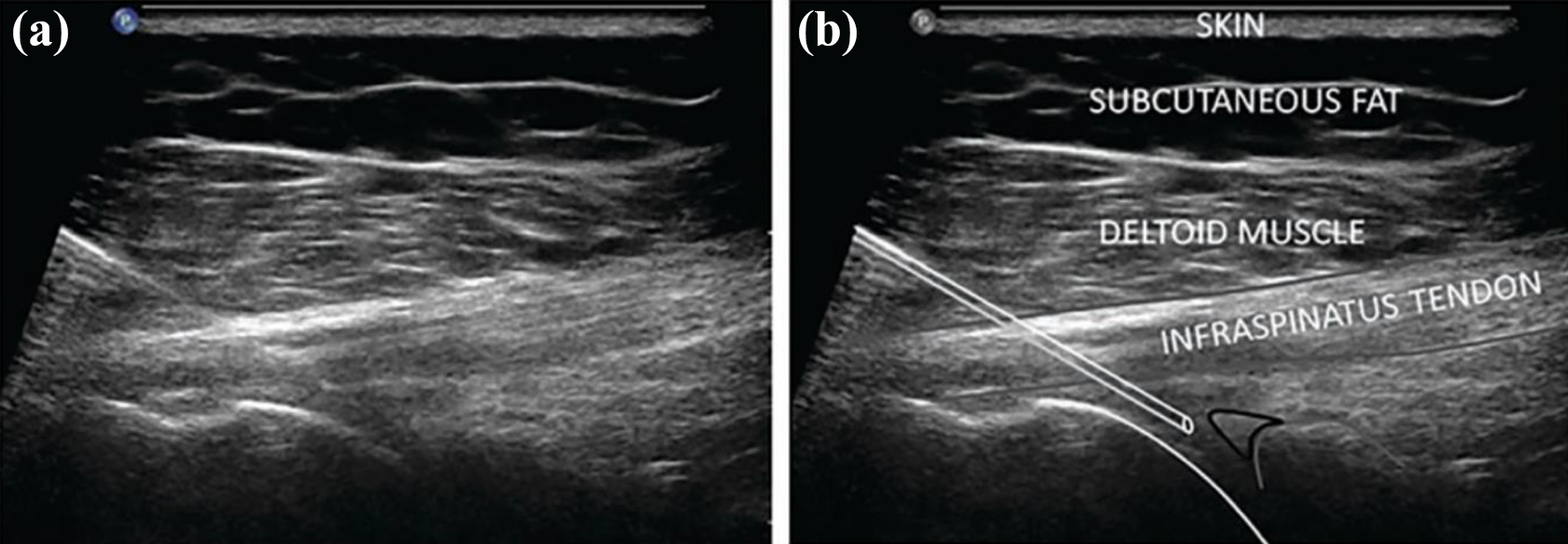
(a) Ultrasound image showing needle tip positioning into the glenohumeral joint. (b) Corresponding image annotating anatomical structures, humeral head and needle outlined in white, glenoid in grey and posterior labrum in black, adapted from Sinha et al. (2017). 8
Patients were recommended exercises to do at home following the procedure, which consisted of standard abduction and flexion wall crawl exercises and ROM exercises in different movement planes using a stick for assistance. An example of this can be seen in Figure 3. Follow-up dates were set for approximately 6 weeks post-procedure whereby outcome measure testing was repeated.

An example of the wall crawl exercise. The patient walks their fingers along the wall until a stretching sensation is achieved where it is held for 15 s before being repeated, adapted from Boland (2016). 9
Patient consent was not required due to the retrospective nature of the service evaluation, although patients had previously given consent to their data being collected by the NHS. However, ethical considerations exist around the access to confidential patient data, therefore ethical approval was granted from NHS research and development, as well as The University of Leeds (ethical reference number: BIOSCI 18-019).
Primary outcome measures for the study included patient-reported pain score using the NRS pre-procedure and upon follow-up; shoulder ROM in abduction, flexion, external rotation and internal rotation, measured in degrees using a manual goniometer pre-procedure and upon follow-up; any further interventions required to resolve patient symptoms, which were determined upon follow-up. The NRS employed in the study was a scale of 0 to 10, with 0 being no pain and 10 the maximal pain. An independent researcher extracted the data from records and was able to provide an independent analysis without bias of the treating clinician MS.
All analysis of data was carried out through the IBM SPSS Statistics analysis software (version 25). A statistical significance level (p) of 0.05 was employed throughout the analysis. After assessing normality of data using Shapiro–Wilk tests, pre-procedure and follow-up pain score and ROM were compared using either paired-sample t-tests if normality was assumed, or Wilcoxon signed-rank tests if normality could not be assumed. Multiple linear regressions were used to assess the influence of predictor variables of age, diabetes status, and duration of symptoms on outcome variables of pain score and total shoulder ROM. A one-way analysis of variance (ANOVA) was used to determine the influence of predictor variables on the requirement for further intervention.
Results
Tests of normality concluded that all variables were not normally distributed (p < 0.05), except total ROM pre-procedure and upon follow-up, as well as follow-up abduction and flexion (p > 0.05). The results of the paired-sample t-test and Wilcoxon signed-rank tests all yielded statistically significant differences when comparing pre-procedure to follow-up measures (all p < 0.01), as seen in Table 2. This demonstrates a decrease in pain scores and an increase in available ROM following the hydrodilatation procedure, as seen in Figure 4.
Comparisons of pain score and ROM of different shoulder movements.a
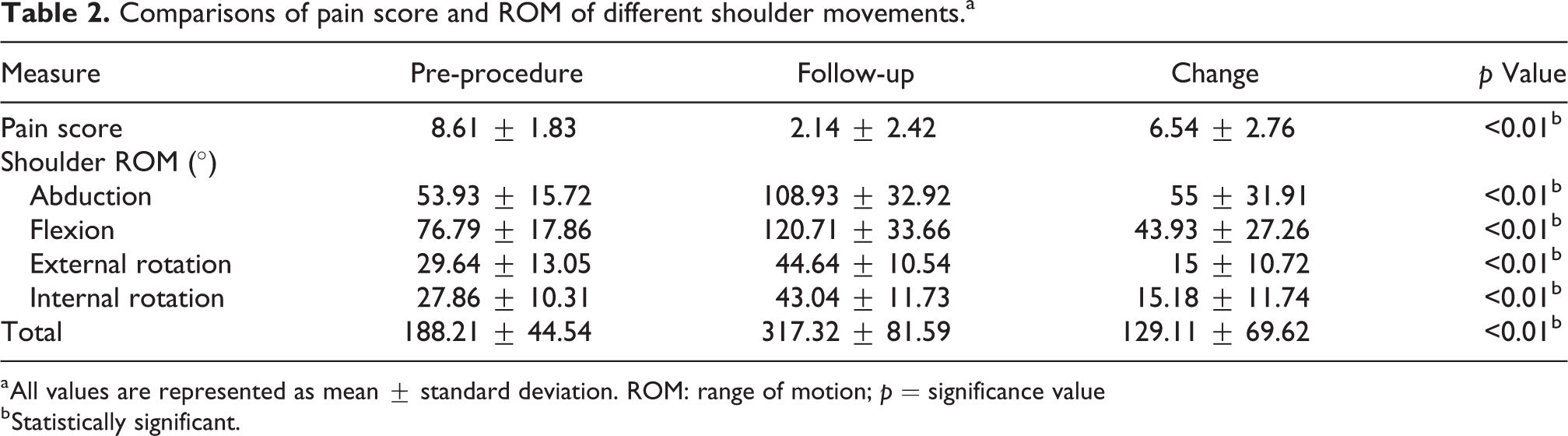
a All values are represented as mean ± standard deviation. ROM: range of motion; p = significance value
b Statistically significant.
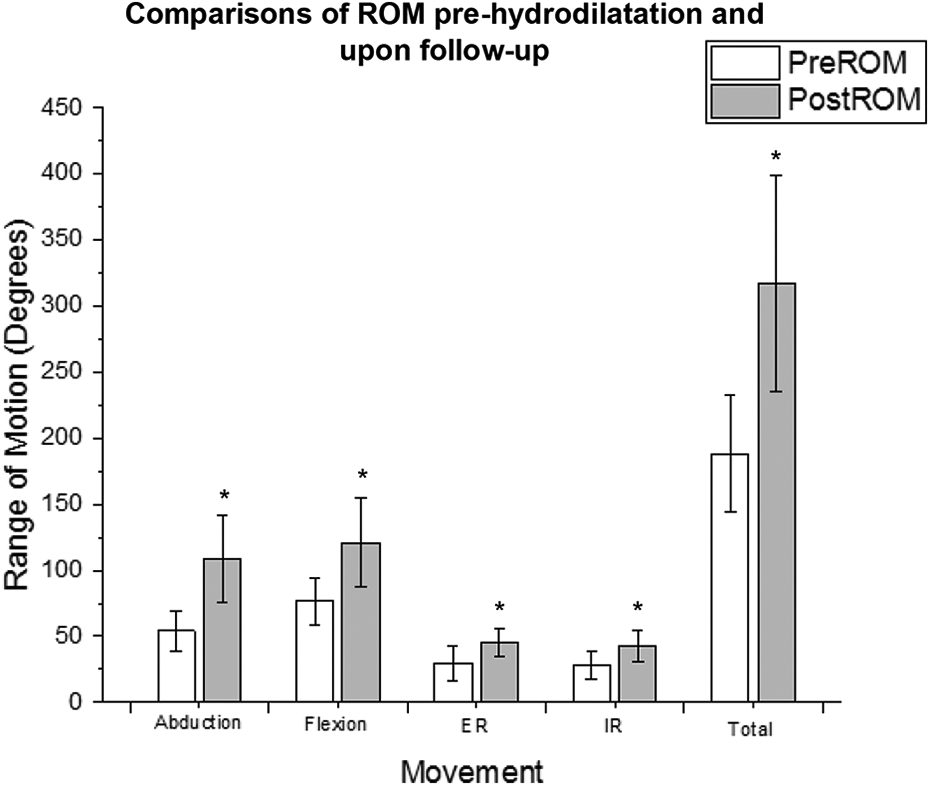
A bar chart illustrating the change in ROM pre-procedure and upon follow-up in each movement plane. Asterick (*) indicates significant difference. ER: external rotation; IR: internal rotation; Pre-ROM: pre-procedure range of motion; Post-ROM: follow-up range of motion.
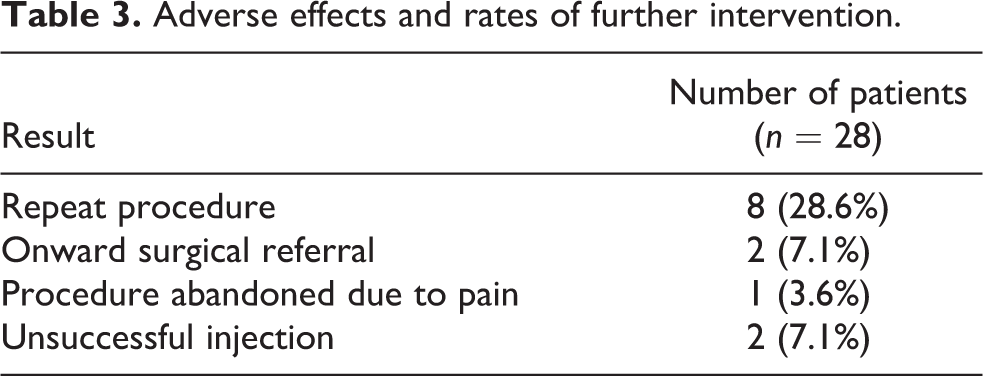
Of the 28 patients, the procedure was unsuccessful in 2 patients as distension of the capsule could not be achieved, and the procedure had to be abandoned in one case because of pain (Table 3). One of these patients required onward surgical referral and the other had symptoms resolved following a repeat procedure. Eight cases had partial improvement and requested a repeat procedure that provided satisfactory results.
Adverse effects and rates of further intervention.
The results of the multiple linear regressions and one-way ANOVA concluded that the predictor variables of age, diabetes status and duration of symptoms did not have a statistically significant influence on both the change in pain score (F(3, 24) = 0.769, p = 0.52, R2 = −0.26), change in total shoulder ROM (F(3, 24) = 1.31, p = 0.29, R2 = 0.033) or requirement for further intervention (F(1, 11) = 0.98, p = 0.34) following the hydrodilatation procedure. In addition, none of the three predictor variables individually added statistically significant influence on either of the outcome variables (p > 0.05). A summary of the significance values of these tests can be found in Table 4.
Statistical significance values of the influence of predictor variables on outcome variables.a
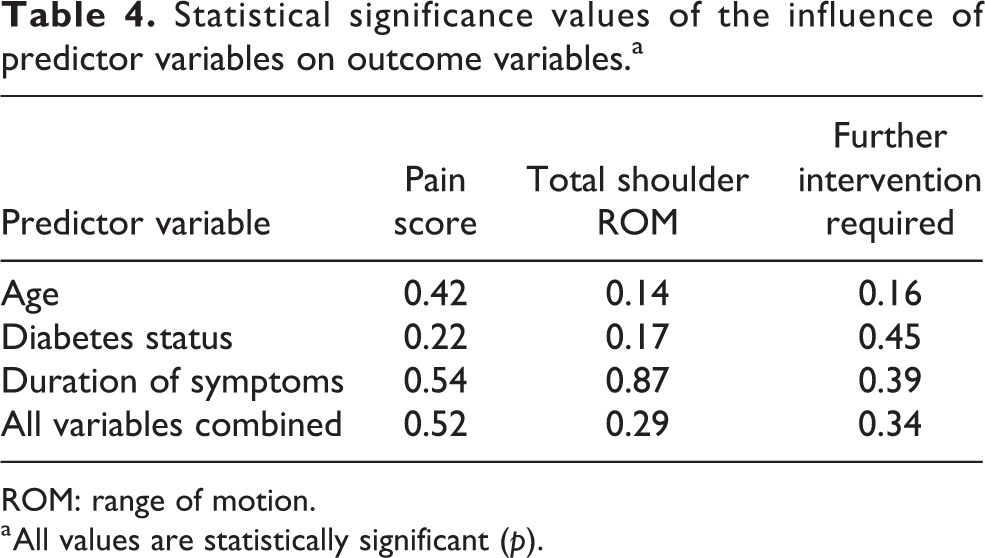
ROM: range of motion.
a All values are statistically significant (p).
Discussion
It is evident from the results of this retrospective service evaluation that the USG hydrodilatation procedure is a safe and effective intervention for AC that can be performed in an outpatient clinical setting. There were statistically significant improvements in both pain and ROM in all shoulder movements. The ability to administer the injection in an outpatient setting would also have a positive economic impact on the health-care services, with estimated savings of £1160 when compared to manipulation under anaesthesia and savings of £1920 when compared to arthroscopic capsular release. Twenty five of the 28 patients in the sample had symptoms of AC resolved by hydrodilatation. This finding has a significant impact on recommendations of intervention strategies that clinicians consider when facing a patient daignosed with AC. A clinician should consider the hydrodilatation procedure before referring to surgery as symptoms can be resolved from a less expensive outpatient procedure, whilst avoiding added risks of general anaesthesia. Results of the current study also suggest that the improvements in pain and total shoulder ROM, as well as the requirement for further intervention, were not influenced by patient age, diabetes status or duration of symptoms. This is significant in terms of the natural history of AC, as it implies that hydrodilatation is suitable for patients at later stages of the condition, as improvements were observed in patients who were symptomatic for up to 24 months before the procedure was carried out.
Results of the current study are in keeping of those of many other existing studies also observing positive short- to medium-term effects in pain and shoulder ROM. This adds to the current evidence base advocating the hydrodilatation procedure as an effective intervention for AC, potentially giving diagnosed patients a means of retaining quality of life without surgical intervention. A study by Quraishi et al. 10 found similar outcomes in pain and shoulder ROM when comparing hydrodilatation with manipulation under anaesthesia, as well as a higher rate of treatment satisfaction in patients within the hydrodilatation group. Comparable outcomes between hydrodilatation and arthroscopic capsular release at 6 weeks were found by Gallacher et al., 7 although arthroscopy was found to be more beneficial after 6 months. The risks associated with the hydrodilatation procedure include allergic reactions to medication used, skin colouration changes, as well as ligament and tendon weakness due to potential leaking of medication into the surrounding structures. 8
The volume of solution used for hydrodilatation remains varied in literature, with studies of higher volumes often trending towards positive outcomes. A study by Haughton et al. 6 investigating the relationship between shoulder function and volume of solution injected found the greatest improvements between the volumes of 30–50 ml. These findings are supported by the improvements found in the current study using 40 ml of solution, suggesting the optimal volume for the procedure may be within this range. Haughton et al. 6 recommend individualising hydrodilatation by injecting fluid until capsular rupture is achieved, rather than targeting a specific volume for the procedure. This could be a direction for further research to confirm the mechanism of capsular rupture by comparing outcomes of procedures using standardised volumes against those with volumes individualised for capsular rupture. As the proposed mechanism of hydrodilatation is the mechanical effect of distention through large volumes of saline, this raises enquiry to whether the corticosteroid or local anaesthetic is required to benefit from the procedure. Therefore, another area of further research would be to compare the effects of hydrodilatation with an intra-articular high-volume injection using only saline to determine the influence of the added corticosteroid and local anaesthetic.
There are a number of limitations to this study. The retrospective study design is not ideal for controlling the confounder variables and accurate capture of data. Although standardised data were available for all patients, additional information such as the effect on activities of daily living, exercise adherence and tolerance, and symptoms other than pain and reduced ROM were unavailable. Furthermore, the study included no control or placebo group, as well as the clinician not being blinded during the recording of outcomes, which subsequently reduces the reliability of data. The small sample size of 28 reduces the generalisability of outcomes observed in this study. The small sample size for men (n = 5) led to the exclusion of gender comparisons in statistical analysis.
In conclusion, the results of this study support the use of USG hydrodilatation procedure as a safe and effective intervention for AC patients resistant to conservative treatment. Improvements in shoulder ROM and pain were evident in the short-term (6 weeks), supporting its utilisation before surgical consideration.
Footnotes
Acknowledgements
We would like to extend our sincere gratitude to colleagues in Leeds Community Healthcare NHS Trust and The University of Leeds who have aided the process of this research project, particularly the supervisors of the MSc Sport and Exercise Medicine course – Dr Carrie Ferguson, Professor Stuart Egginton and Dr Camilla Nykjaer.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.