
Abstract
Background/Purpose:
Open reduction of acute avulsion of posterior cruciate ligament (PCL) fragment may be achieved through direct posterior approach or posteromedial approach. The aim of our study was to compare these two techniques for fixation of avulsed PCL fragment. Our primary study objective was to study that which of the above techniques provides a better screw placement on post-operative radiographs. The secondary objectives were to study any statistically significant differences in surgical time, blood loss, incidence of neurovascular injury, bone union and functional knee scores in the above two techniques.
Materials and methods:
This is a prospective, comparative, interventional, single tertiary referral centre-based study from November 2014 to May 2019. Patients in the direct posterior group were treated with the approach described by Abbott and Carpenter, and patients in the posteromedial group were treated with the approach described by Burks and Schaffer. Screw placement was assessed on anteroposterior (AP) and lateral knee X-rays. Blood loss was studied using haemoglobin balance method. Functional scores were recorded preoperatively and at 1-year follow up using Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) knee scores.
Results:
The posterior group showed better screw placement angle compared to the posteromedial group. In the AP plane, the mean angle of screw placement and fracture line was 83° compared to 59° in the posteromedial group. Average fracture union time, post-operative range of motion and post-operative WOMAC scores were not statistically different in both groups. There were no cases of neurovascular complication, deep vein thrombosis and superficial or deep surgical site infection in any group.
Conclusion:
Direct posterior approach to PCL avulsion provides better screw placement angle compared to the posteromedial approach, which might result in better interfragmentary compression at the avulsion site. However, the two approaches did not differ statistically in terms of functional scores of patients reported at 1 year.
Introduction
Posterior cruciate ligament (PCL) plays a pivotal role in maintaining knee stability. It is the primary restrain for preventing posterior subluxation of tibia over femur and its deficiency causes posterior instability with increase in patellofemoral joint pressure. Long-standing PCL-deficient knees are prone for degenerative osteoarthritis. 1,2 Its avulsion from the tibial side is usually seen in younger patients and is a result of high-velocity trauma. Most authors agree that reduction of avulsed fragment and its fixation to its original tibial site is the treatment of choice for acute PCL avulsion. 3 –6 This can be achieved through minimally invasive techniques using arthroscopy or open techniques. 2,7 Although arthroscopic repair is minimally invasive, the technique has posed several limitations, including the fact that such fixation and reduction are more challenging to perform than open surgery. The long learning curve and a requirement for specialised equipment for arthroscopic technique make it difficult to implement in primary-level hospitals. For these reasons, still many hospitals treat PCL avulsion fractures of the tibia with open techniques. 2
Open reduction may be achieved through direct posterior approach or posteromedial approach. 8,9 The aim of our study was to compare the two techniques for fixation of avulsed PCL fragment. Our primary study objective was to study which of the above techniques provides a better screw placement on post-operative radiographs. The secondary objectives were to study any statistically significant differences in surgical time, blood loss, incidence of neurovascular injury, bone union and functional knee scores in the above two techniques. We hypothesised that the two techniques would not differ significantly in any of our study parameters.
Materials and methods
This is a prospective, comparative, interventional, single tertiary referral centre-based study from November 2014 to May 2019. Approval of institutional review board was taken prior to study. All patients between 20 years and 50 years with isolated PCL avulsion from the tibial site were included in the study (Figures 1 and 2(a) and (b)).
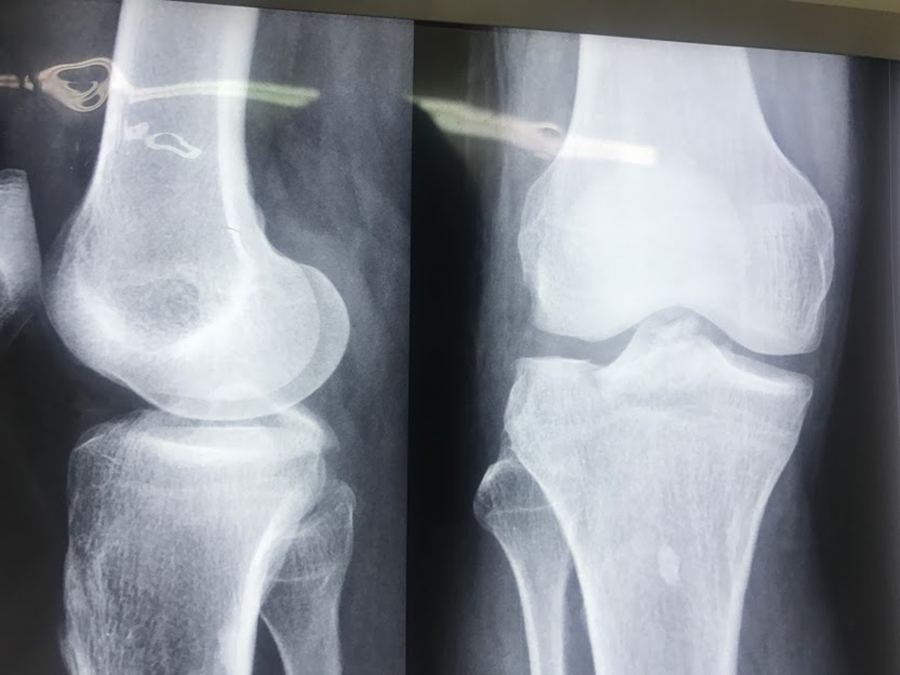
X-ray AP and lateral view of knee joint showing isolated PCL avulsion fragment from the tibial side. AP: anteroposterior; PCL: posterior cruciate ligament.
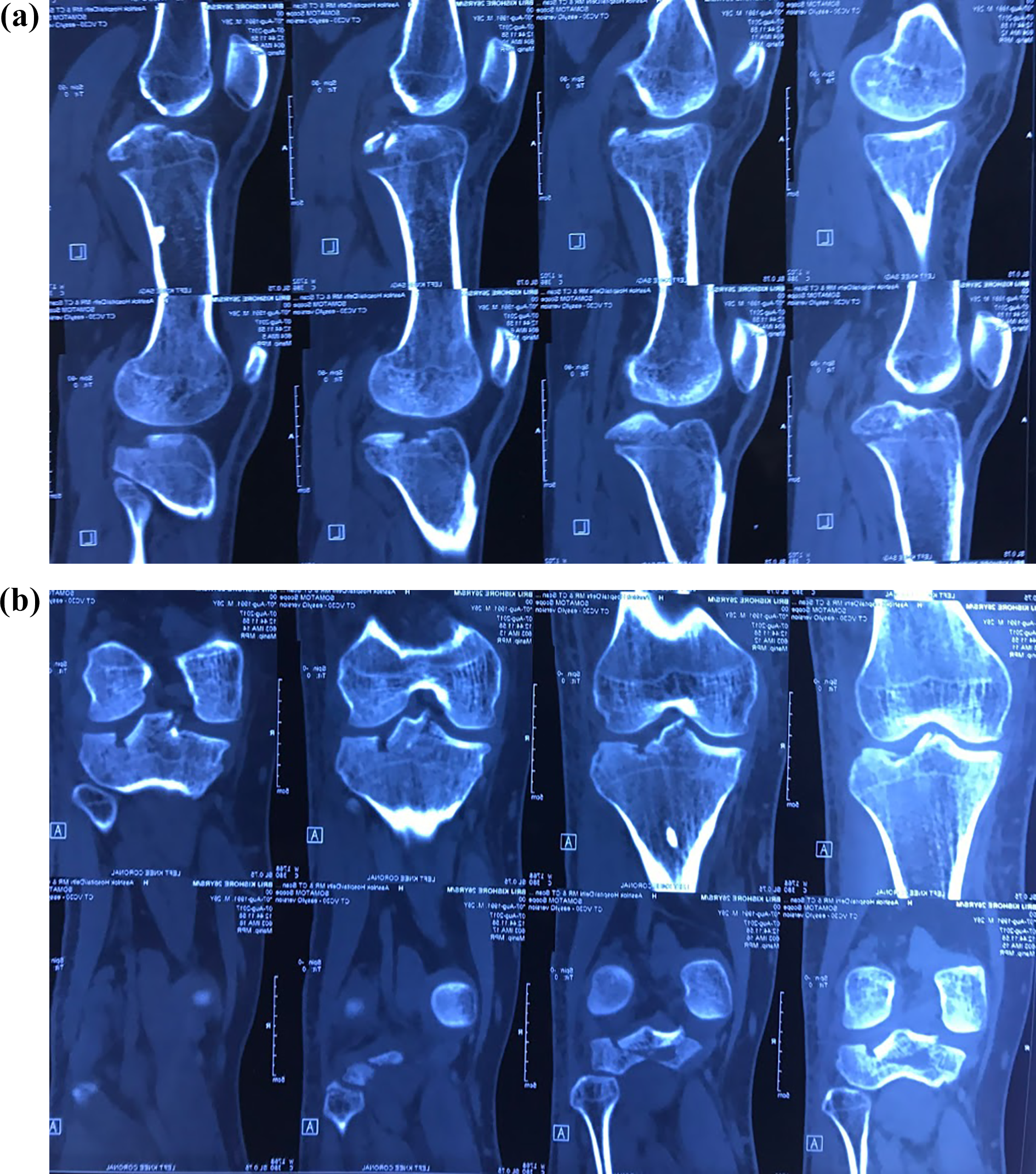
(a) Sagittal CT films of a 28-year-old male with avulsed PCL fragment from tibial side. (b) Coronal CT films of a 28-year-old male with avulsed PCL fragment from the tibial side. CT: computed tomography; PCL: posterior cruciate ligament.
Patients with other significant ligamentous injuries of the same knee were excluded from the study. Patients with less than 1-year follow-up were also excluded from the study. Patients were randomised based on their registration number which was given by the clerical orthopaedic staff not involved in the study. This ensured proper blinding and minimised selection bias. Patients with even registration number were operated by direct posterior approach and those with odd registration number were operated by posteromedial approach.
Informed consent for participation of the study was taken by all patients. All surgeries were done under spinal anaesthesia with patients in prone position under pneumatic tourniquet. Preoperative antibiotic prophylaxis using ceftriaxone was given to all patients.
Patients in the direct posterior group were treated with the approach described by Abbott and Carpenter. 8 In this approach, skin incision was ‘S’ shaped with lateral proximally, crossing popliteal crease transversely and then extending medially in the distal part. Skin flaps were created, and the medial sural cutaneous nerve was identified in close relation to the small saphenous vein. The nerve was followed proximally back to the tibial nerve between the two heads of gastrocnemius, and the neurovascular bundle was approached which lies in close relation to the tibial nerve. The neurovascular bundle was retracted away from the surgical field. The avulsed fragment was approached by incising the posterior capsule, and the fracture was fixed using one or two 4-mm cannulated cancellous screws. The screws were aimed perpendicular to the fracture site for maximum compression (Figure 3(a) to (d)).
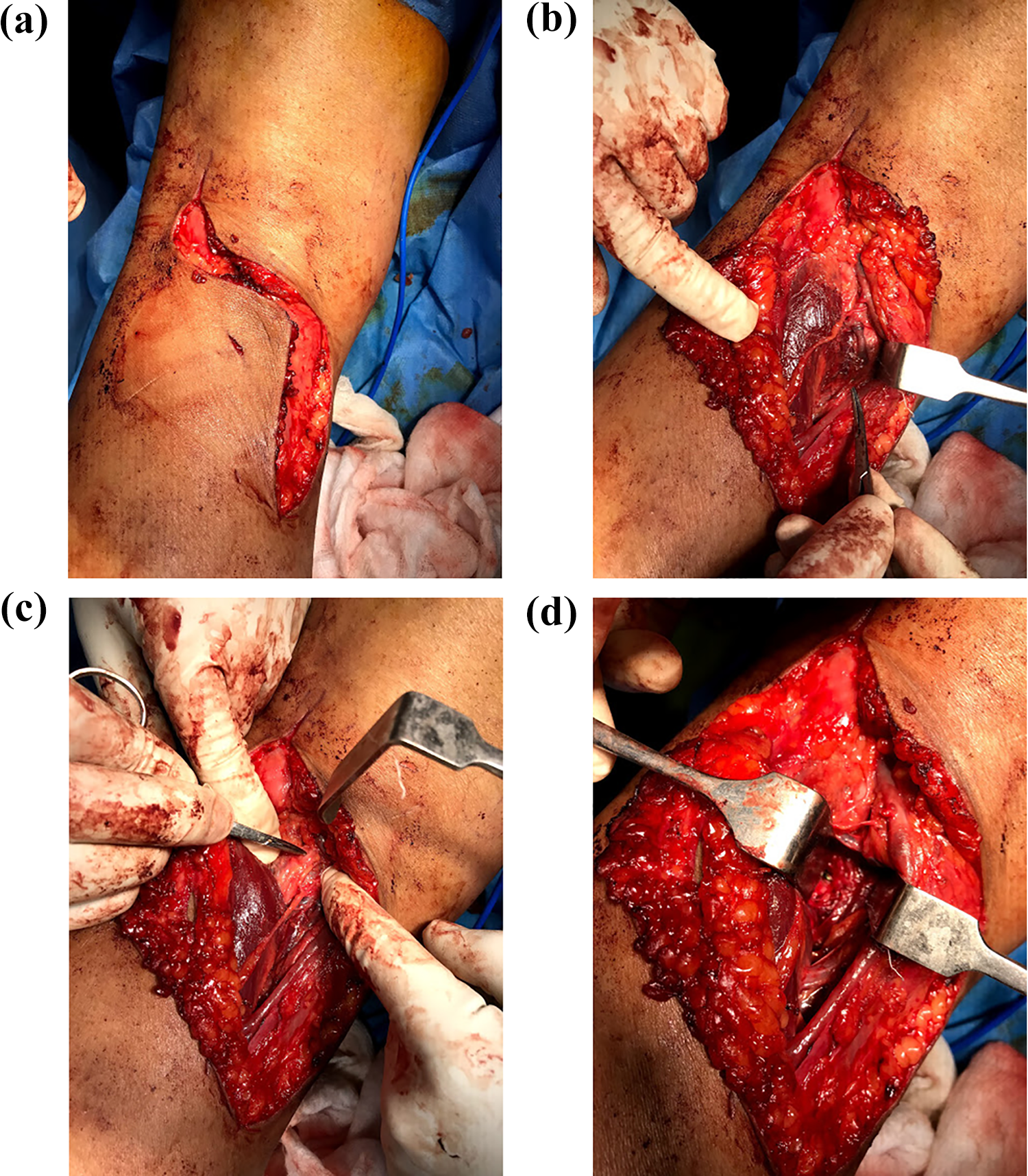
(a) ‘S’-shaped incision used in the direct posterior approach. (b) Intraoperative clinical photograph of the posterior approach after superficial dissection showing close relation of medial sural cutaneous nerve (pointed by haemostatic clamp) to small saphenous vein. (c) Intraoperative clinical photograph of the posterior approach showing the medial cutaneous sural nerve joining its origin to tibial nerve. (d) Intraoperative clinical photograph of the posterior approach showing PCL fragment fixed with screw. PCL: posterior cruciate ligament.
Patients in the posteromedial group were treated with the approach described by Burks and Schaffer. 9 An inverted ‘L’-shaped incision was used. Plane was created posteromedially between the medial head of gastrocnemius, and the semimembranosus and medial head was reflected laterally. Posterior capsule was incised over the avulsed fragment, and the fracture was reduced and fixed using one or two 4-mm cannulated cancellous screws. The screws were aimed perpendicular to the fracture site for maximum compression (Figure 4).
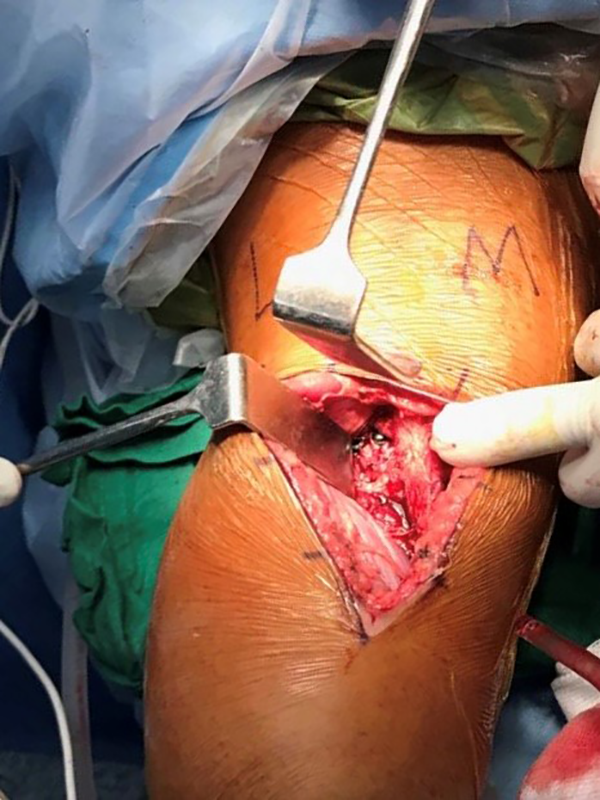
Intraoperative clinical photograph of the posteromedial approach showing PCL fragment fixed with two screws. The inverted ‘L’-shaped incision and retracted medial head of gastrocnemius is shown. PCL: posterior cruciate ligament.
Patients in both groups followed similar post-operative rehabilitation protocol. Blood loss was calculated using haemoglobin balance method. 10 The lowest post-operative haemoglobin of the patient on first four post-operative days was used for the above calculation. A posterior slab at 15° of knee flexion was given for 2 weeks. Patients were then started on knee mobilisation exercises under a trained physiotherapist. Patients were kept on partial weight bearing till fracture union.
Screw placement was assessed on AP and lateral knee X-rays. Angle between the fracture line and the screws was measured on both AP and lateral views (Figure 5(a) and (b)).
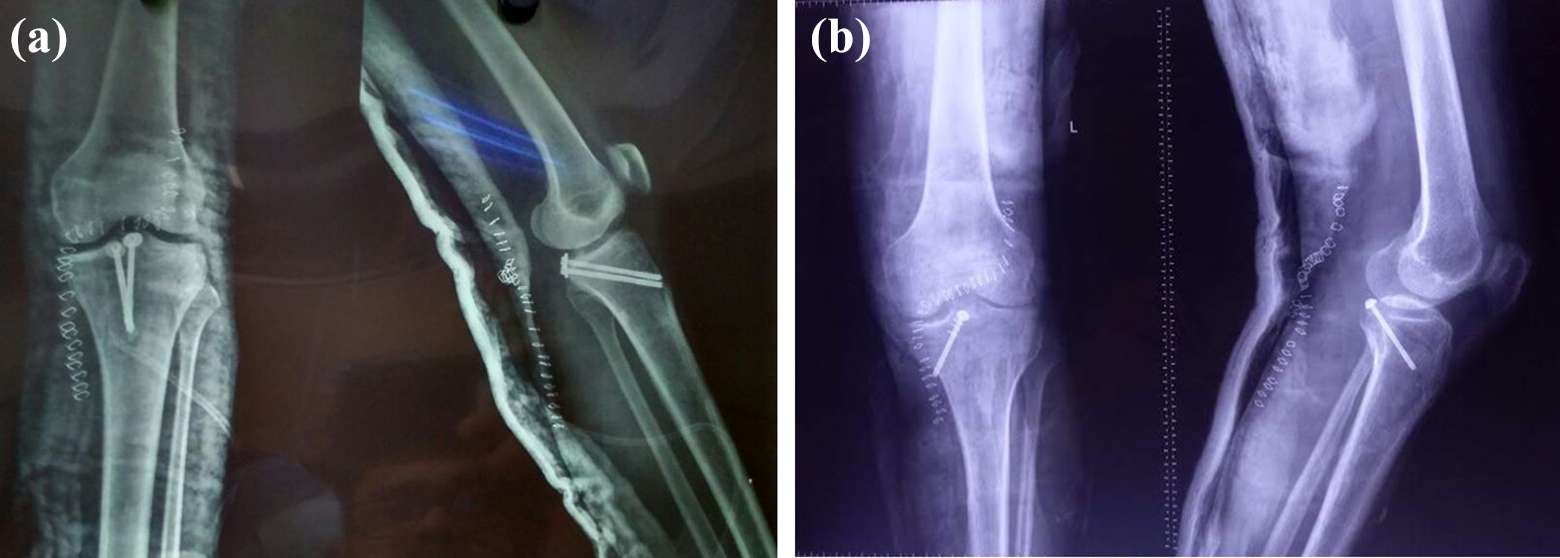
(a) Post-operative X-ray knee showing AP and lateral views after the posterior approach. It is noted that the position of screws is perpendicular to the fracture site. (b) Post-operative X-ray knee showing AP and lateral views after posteromedial approach. It is noted that the position of screws is not perpendicular to the fracture site. AP: anteroposterior.
These measurements were done by two independent orthopaedic fellows at three different occasions not involved in the study. The average of their values was used as the final value. Patients were followed up for a minimum of 1 year. The X-rays to assess union were done at 6- to 8-week interval. Functional scores were recorded preoperatively and at 1 year follow up using The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) knee scores. 11
Statistical analysis
All quantitative data were expressed as mean ± standard deviation. The patients were divided into two groups: the posterior approach group and the posteromedial approach group. Statistical significance of differences in the mean values of continuous variables were determined using Student’s t-test. The χ 2 test was used for categorical variables. Fisher’s exact test replaced χ 2 test when one of the cells in categorical variables was zero. SPSS version 14.0 (SPSS Inc., Chicago, Illinois, USA) was used for statistical analyses. A p value less than 0.05 was considered to indicate statistical significance. All aspects of the statistical analysis were reviewed by a statistician.
Results
A total of 37 patients, 17 by direct posterior approach and 20 by posteromedial approach, were operated for PCL avulsion during the study period. The mean age was 31.3 years. There were 26 males and 11 females in the study. Table 1 describes the preoperative demographics of patients in both groups. The patients had no statistically significant differences in their demographic characteristics.
Preoperative parameters of the direct posterior and posteromedial groups.
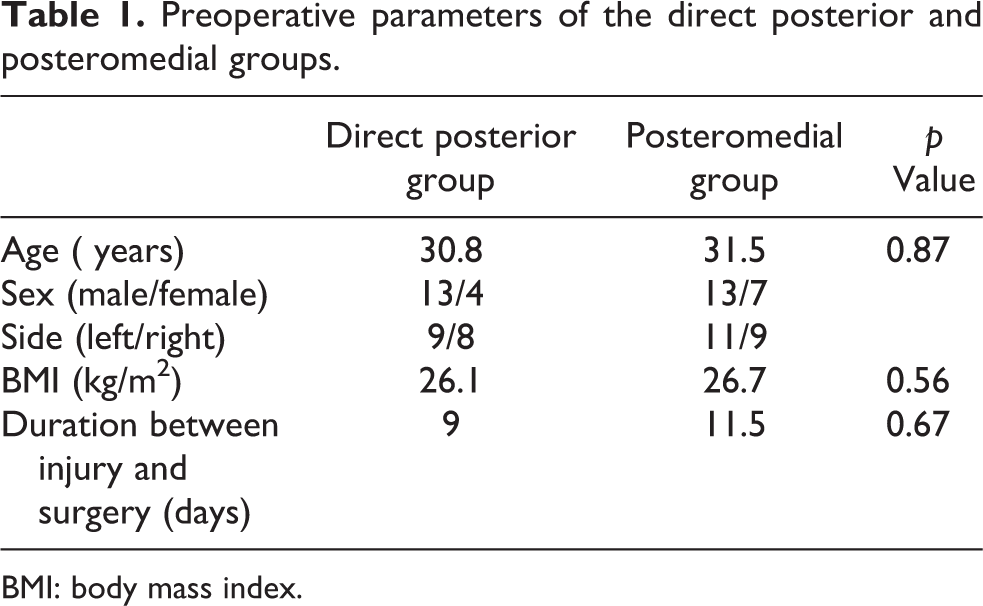
BMI: body mass index.
Table 2 describes the post-operative parameters in both groups. The mean surgical time and blood loss in the posteromedial group was 42 min and 210 ml, respectively, which was significantly less than the direct posterior group that required mean of 58 min for surgery and had an average blood loss of 360 ml (p = 0.03; p = 0.01). Two patients required blood transfusion in the direct posterior group, while none required any transfusion in the posteromedial group.
The posterior group showed better screw placement angle than the posteromedial group. In the AP plane, the mean angle of screw placement and fracture line was 83° compared to 59° in the posteromedial group (p = 0.00). However, on lateral view, the angles were not significantly different, with the posterior group having an angle of 84° compared to 81° in the posteromedial group.
The average fracture union time, post-operative range of motion and post-operative WOMAC scores were not statistically different in both groups. There were no cases of neurovascular complication, deep vein thrombosis and superficial or deep surgical site infection in any group. Three cases showed radiological non-union of PCL fragment in the posteromedial group; however, none of these patients had any complaints related to instability. None of the patients showed non-union in the posterior group.
Post-operative parameters of the direct posterior and posteromedial groups.
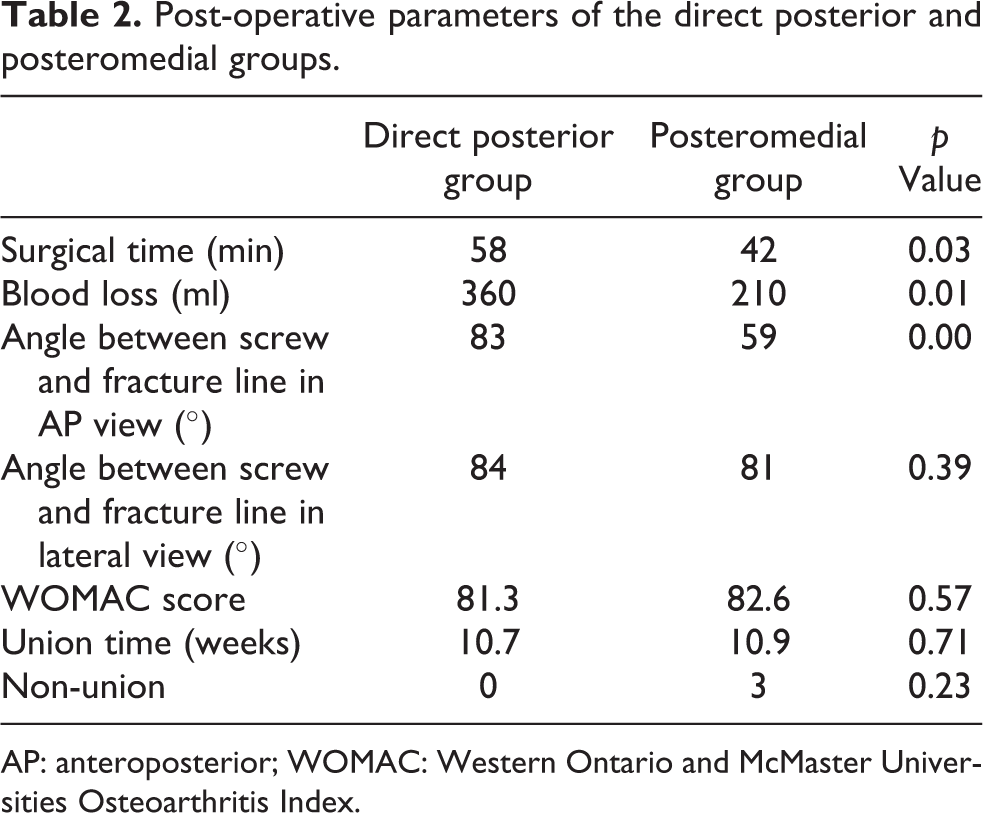
AP: anteroposterior; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Discussion
The most important finding of our study is that the screw placement was better and more perpendicular to the fracture site when operated from the direct posterior approach compared to the posteromedial approach. However, the surgical time and bleeding were less in the posteromedial approach. The clinical scores, time to fracture union and complication rates were, however, similar in both groups.
The fixation of PCL avulsion has been reported through various approaches. Classical posterior approach described by Abbott and Carpenter approaches the avulsed fragment directly between two heads of gastrocnemius. 8 Although this approach gives direct access to the fragment, it is very close to vital structures including popliteal artery and tibial nerve. To avoid these vital structures, various authors have proposed the posteromedial approach. This approach gives a good view, and many authors have successfully used this approach for fixation of PCL avulsion fragment. 4 However, reports of loss of reduction or less compression that potentially causes pseudarthrosis have been presented in the literature with this approach. 12 –14 This prompted us to compare the two approaches to find out whether there are statistically significant differences in results.
Compression of avulsed fracture fragment at the fracture site is one of the most important factors in achieving fracture union. Maximum compression can be achieved by placing the screws perpendicular to the fracture site. This criterion was more uniformly met through the direct posterior approach as it provides direct access to the fracture site with no hindrance of the neighbouring structures. The retracted gastrocnemius in the posteromedial approach limits the angle at which the screw can be placed (Figure 6(a) and (b)). Similar findings were observed by Ambra et al. in their cadaveric study, where they found that the direct posterior approach allows a greater degree of freedom compared with the posteromedial approach to reach the PCL tibial insertion, permitting the placement of fixation devices closest to right angles. 15
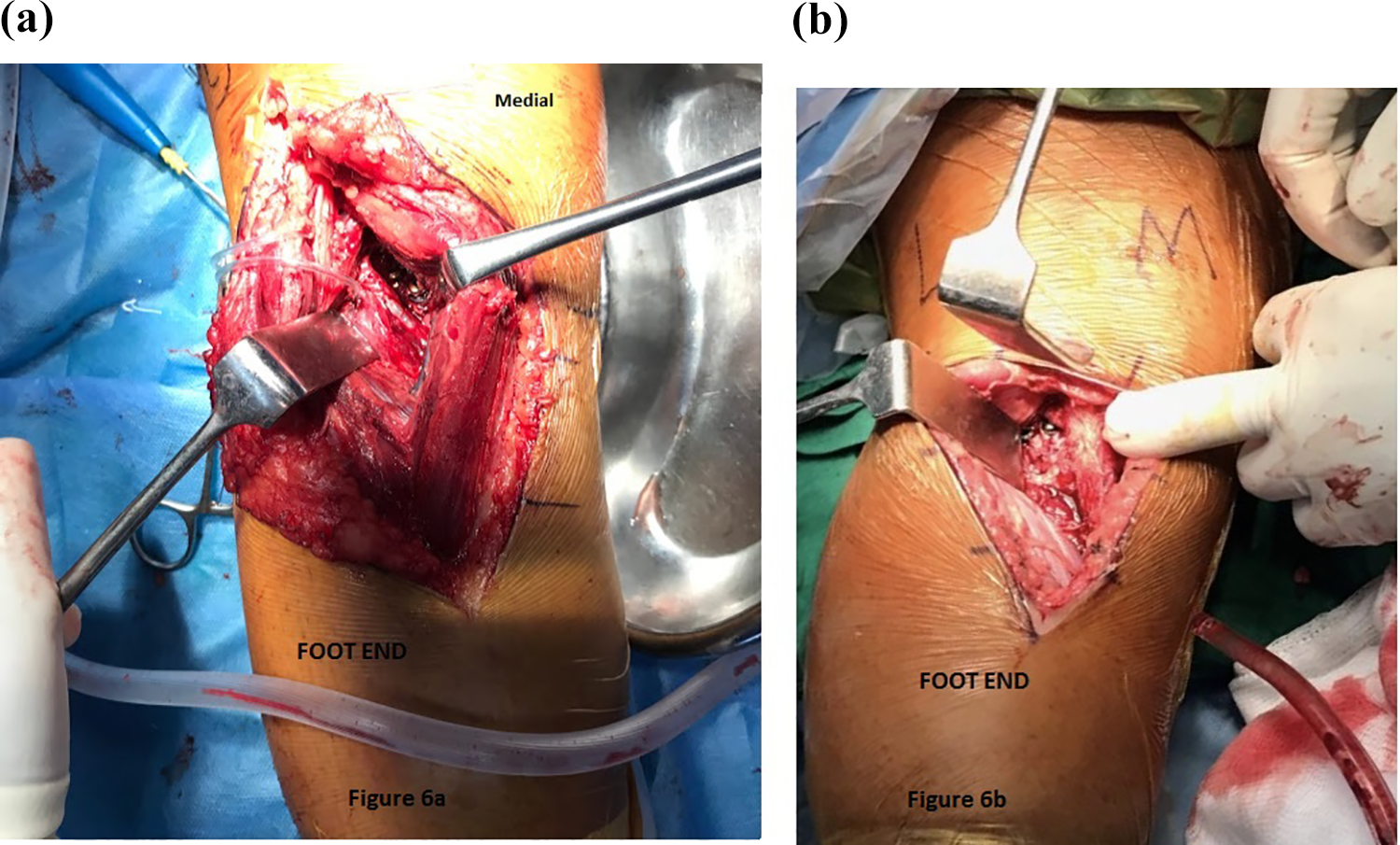
Intraoperative clinical photograph of the posterior (a) and posteromedial (b) approach. It is noted that in the posteromedial approach, the medial head of gastrocnemius provides hindrance for screw placement in contrast to the posterior approach which is relatively free after neurovascular dissection.
Even though the posterior approach allows better screw placement, it has the disadvantage of longer surgical time and blood loss. The isolation of neurovascular structures is time-consuming and has to be done meticulously. If carefully done, the chances of neurovascular damage in both approaches are similar.
Another important finding was that better screw placement did not extrapolate to better functional scores. Both groups had similar WOMAC scores at 1 year. It may be due to our small sample size or natural history of PCL injury which inherently has better chances of healing. Even the cases with radiological pseudarthrosis did not complain of instability, probably due to fibrous union of the avulsed fragment. However, authors strongly believe that this finding should not discourage surgeons to aim for perpendicular screw placement which is biomechanically stronger. Such screw placement is time tested.
The strength of our study is its prospective nature and blinding. The treating surgeon was unaware of the approach which was based on the registration number not in control of the surgeon. Further to the best of our knowledge, this is an uncommonly done attempt to compare the common approaches, and further studies in this regard would help to establish a more acceptable protocol. However, there are few limitations to the study. Firstly, the sample size is small, and therefore all inferences may not hold true for all patients. Secondly, it is a single-centre–based study with male predominance. Further studies on this topic from different centres may help to overcome this limitation. Thirdly, the follow-up period is small, and the results of surgery or approach on joint arthritis cannot be commented over such small period of time.
Conclusion
The direct posterior approach to PCL avulsion provides better screw placement angle compared to the posteromedial approach which might result in better interfragmentary compression at the avulsion site. However, the two approaches do not differ statistically in terms of functional scores of patients reported at 1 year.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.