
Abstract
Background/Purpose:
Total hip replacement (THR) is considered as one of the most successful orthopedic procedures. However, improperly placed components can lead to instability and accelerated wear. Acetabular cup inclination can be very well accessed by anteroposterior pelvis X-rays; for acetabular version assessment, computed tomography (CT) scan is the gold standard. CT scan is not readily available at many centers and the surgeon has to rely on X-ray methods for evaluation of acetabular version to audit results and to predict behavior of the surgical intervention. This prospective study was undertaken to compare Woo and Morrey’s and ischiolateral methods of assessment of acetabular version on cross-table lateral radiographs with CT assessment and to assess the validity of radiographic methods with respect to CT scan method.
Material and methods:
A prospective follow-up study was conducted for 18 months’ duration (October 2016 to March 2018) on 30 adult patients who underwent THR surgery. Cross-table lateral radiograph was obtained at 3 and 6 weeks in the postoperative period. Two observers made each observation at two different points of time. CT scan was performed at 3 weeks. Version as measured by radiographs and CT scan was recorded.
Results:
The major overlap in the distribution of the values of the Woo and Morrey method suggests that there is no significant difference between the observations. Distribution of the values of the ischiolateral view and the CT scan value distributions have a very small overlap and hence suggest a strong significant difference between the two.
Conclusion:
In this study, Woo and Morrey’s method and ischiolateral method of assessment of acetabular version were compared with CT assessment. We found that in Woo and Morrey’s method, values were comparable to CT scan values, when put on regression line. However, in situation of change in patient positioning, namely hip stiffness in contralateral hip, measurement of component changed in series of radiography due to differences in pelvis tilt. So, in these circumstances, we can use ischiolateral method which can give consistent measurement. But it will not be in concordance with CT scan values and Woo and Morrey values, as represented in regression line. The high intra-class correlation coefficients for both intra- and inter-observer reliability indicated that the angle measured with these methods is consistent and reproducible for multiple observers. CT, however, be considered as gold standard for measurement owing to control over pelvic rotation and/or tilt/patient positioning.
Introduction
Total hip replacement (THR) is a remarkably successful and predictable procedure that provides pain relief, functional improvement, and improved quality of life for several hundred thousand patients each year worldwide. 1,2
Knowledge of acetabular component position after THR is important because malposition has been associated with hip instability resulting in recurrent dislocation, impingement, and accelerated wear. 3,4
Acetabular version is defined as the angle between the axis of the component and the coronal plane of the patient body which is approximately 17° (range 11.5–28.5°). If the cup has been excessively anteverted, anterior dislocation can occur during hip extension, adduction, and external rotation. If the cup is retroverted, dislocation occurs posteriorly with flexion, adduction, and internal rotation. Excessive inclination of the cup can lead to superior dislocation with adduction, especially if there is a residual adduction contracture, or if the femur impinges on osteophytes left along the inferior margin of the acetabulum. Conversely, if the cup is inclined almost horizontally, impingement occurs early in flexion, and the hip dislocates posteriorly; this is accentuated if the cup also is in less anteversion. 3 –5
Cup position has been defined as radiographic, operative, and anatomical inclination and anteversion. 5 The two reference planes for measuring cup position are the anterior pelvic plane and the functional coronal plane (FCP) 6 (Figure 1). Cup position on plain radiographs has been defined as radiographic inclination and version relative to the FCP. Cup position on computed tomography (CT) scans must be measured using the same definition and reference plane to compare the accuracy of different plain radiography methods.
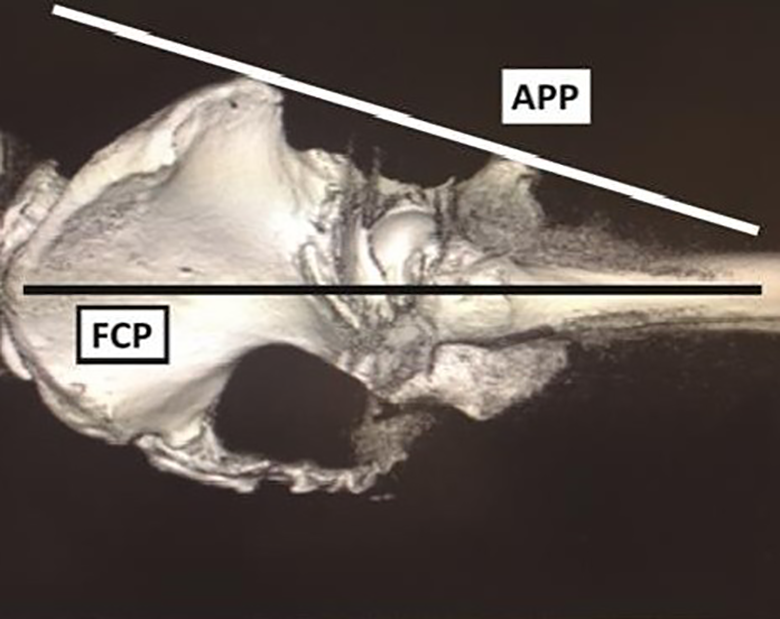
Reference planes for measuring cup position.
The cup inclination is easy to measure on plain anteroposterior (AP) radiograph but cup version is difficult to measure. Various radiological methods have been proposed in studies to measure cup version but none have been proved to be reliable and valid compared to CT scan which is the gold standard for measuring acetabular cup version. But CT scan is costly, associated with high radiation dose, and is not widely available.
In this study, Woo and Morrey’s 3 method and ischiolateral method of X-ray assessment of acetabular version are compared with CT assessment because these methods can differentiate anteversion and retroversion, moreover it does not require equations or conversion tables; additionally, these methods are convenient and fast.
The aim of this prospective study was to evaluate the version of the acetabular component following THR on conventional radiographs and CT scan and to assess the validity of radiographic methods with respect to CT scan method.
Materials and methods
Inclusion criteria
Postoperative THR patients who were operated between October 2016 and March 2018 were enrolled in the study.
Exclusion criteria
Previous surgical intervention of hip.
Congenital anomalies of hip.
A prospective follow-up study was conducted for 18 months’ duration (October 2016 to March 2018) on the adult patients who underwent THR surgery.
All postoperative THR patients (fulfilling the inclusion criteria) were recruited to participate in the study. Informed written consent was taken from all patients and subjected to a detailed history regarding previous dislocations, if any, and a local examination was performed documenting the range of motion of each hip joint. A thorough systemic examination was also performed.
Cross-table lateral radiograph was obtained at 3 and 6 weeks in the postoperative period.
Two observers made each observation at two different points of time. CT scan was performed at 3 weeks. Version as measured by radiographs and CT scan was recorded.
Method of measurement of acetabular version on cross-table X-ray
Cross-table lateral view described as lateral projection where the patient is supine and the contralateral hip is flexed. The X-ray beam is parallel to the table and effectively shoots through the groin without dorsal angulation. Such a view has been referred to as a cross-table or a shoot-through lateral view that displays the hip and pelvis at 90° from the AP radiograph. The hip to be imaged is internally rotated 15–20° for visualization of the femoral neck and the trochanters(Figures 2 and 3).

Positioning for cross-table radiograph.
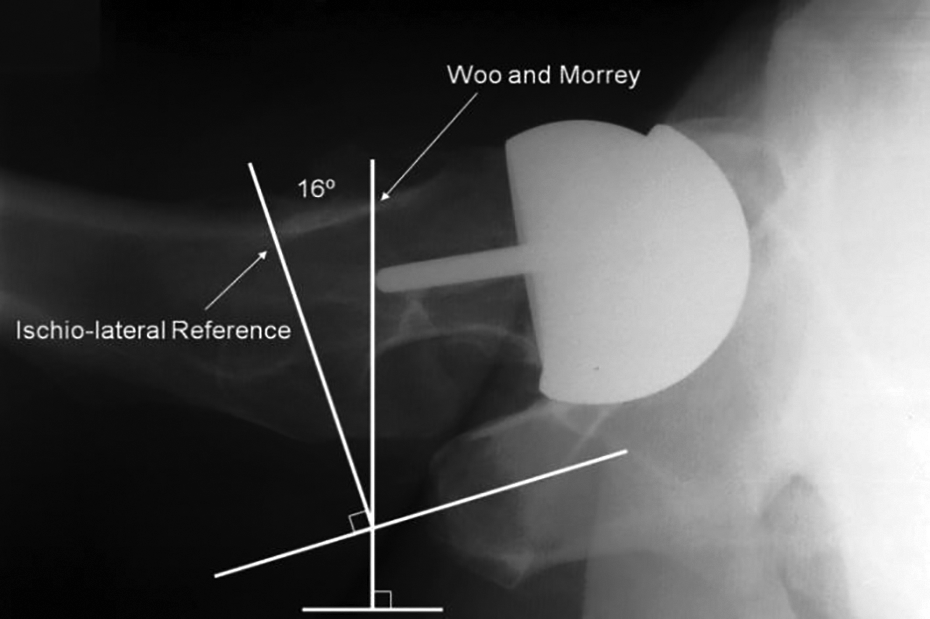
Cross-table lateral radiograph showing Woo and Morrey’s and ischiolateral method references. The measured difference between these references in this example is 16°. 7
Method of measurement of acetabular version by CT scan
CT scans were obtained in the supine position with hip joints in a neutral position. 8 The largest section of the acetabular component was selected in CT axial view. We then draw circles along the margin of the implant or of the acetabulum to set the true center of both hips. We then draw a first line connecting the centers of the two hips and a second line perpendicular to the first. Finally, we draw a third line from the most anterior point of the component to its most posterior point. We then measure the angle between the second and third lines and calculate the version (ø) (Figures 4 and 5). The version from CT scans was regarded as the reference standard for acetabular version.
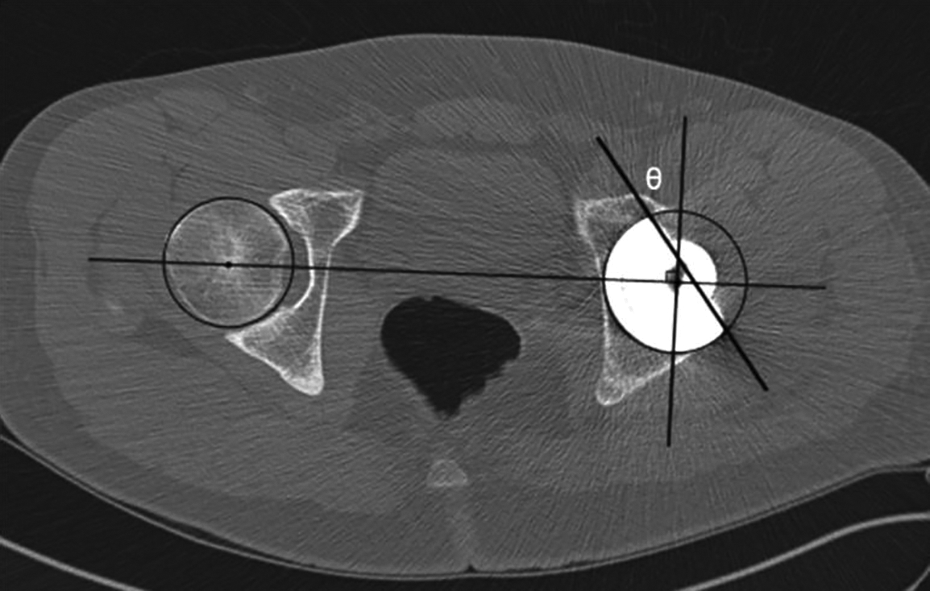
Recommended method of measurement of acetabular version by CT scan. 8 CT: computed tomography.
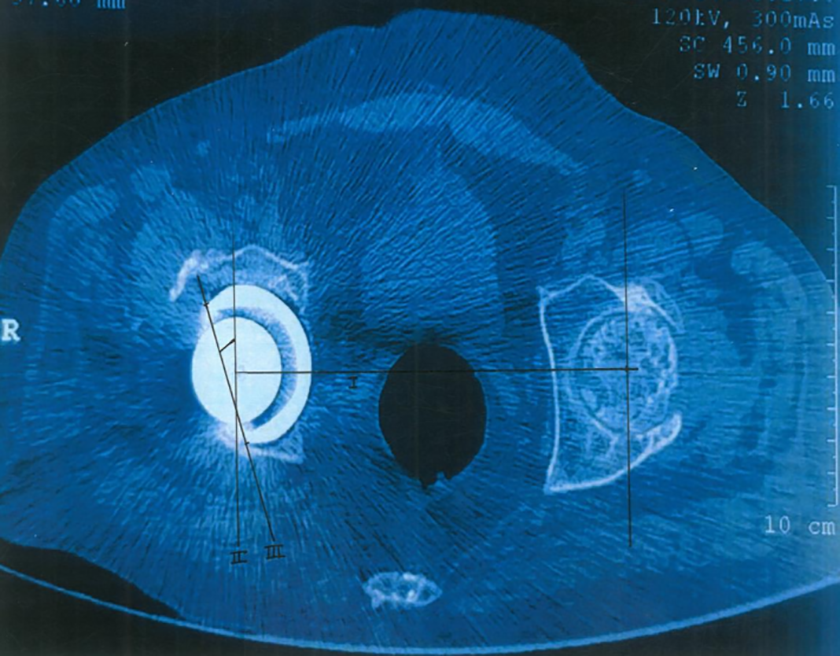
Method of measurement of acetabular version by CT scan. CT: computed tomography.
Then, two observers performed all cross-table lateral radiograph measurements independently, using the same protocols (Figures 6 and 7).
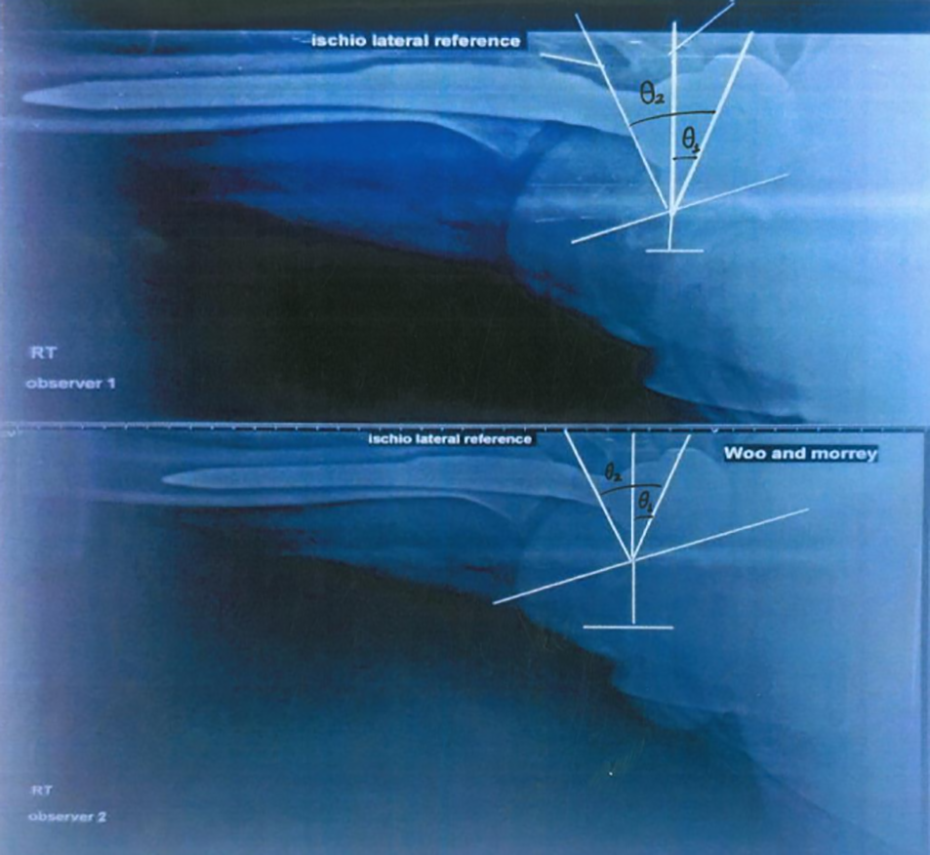
Cross-table lateral view at 3 weeks after THR. THR: total hip replacement.
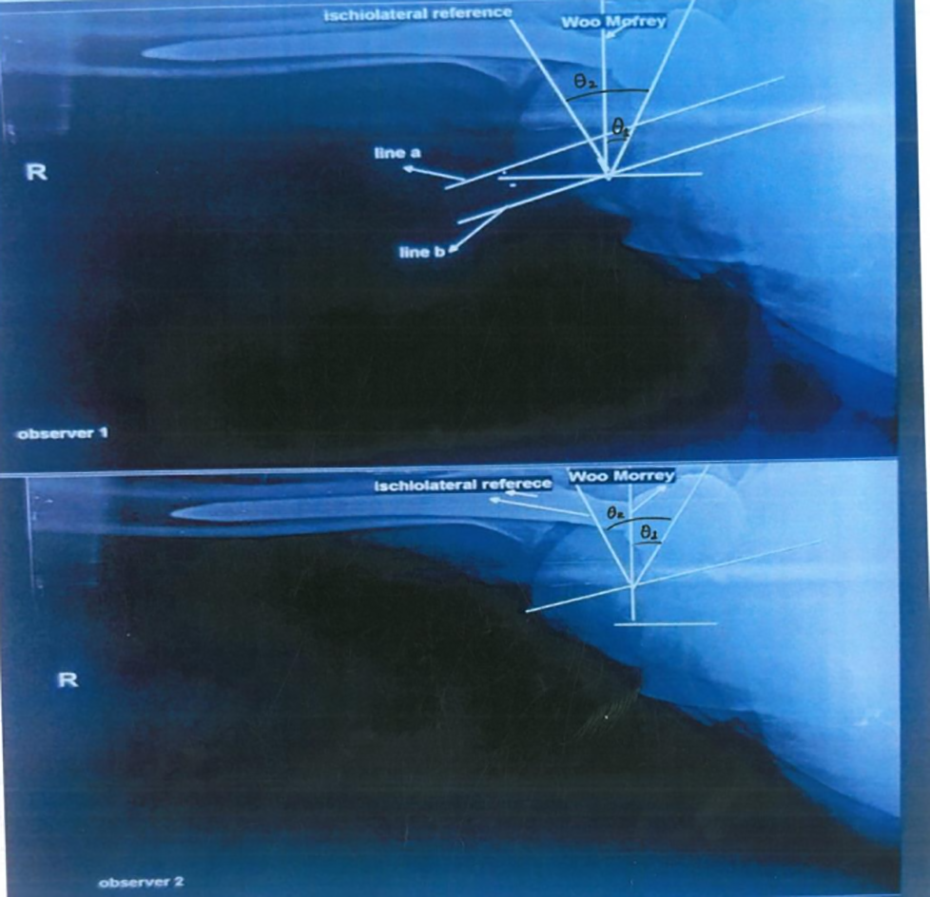
Cross-table lateral view at 6 weeks after THR. THR: total hip replacement.
To assess the intra-observer reliability of each method, one examiner measured all hips two times, with a 3-week interval between measurements, without comparison to the previous measurements.
The inter-observer reliability of each method was assessed by comparing the results of the two examiners. All measurements were made without knowledge of the patient’s clinical information or of the measurements assigned by other examiners.
Plain radiographs and CT scans were presented to each examiner in random order by a research assistant who did not participate in the reliability and accuracy sessions.
To assess the accuracy of measurements on plain radiographs, we compared the average of measurements on plain radiographs with the CT measurements. We calculated the difference between measurements on plain radiographs and CT measurements.
Results and observations
Distribution of the values of the Woo and Morrey method and the CT scan method is shown in Figure 8. The major overlap in the two difference suggests that there is no significant difference between the observations.
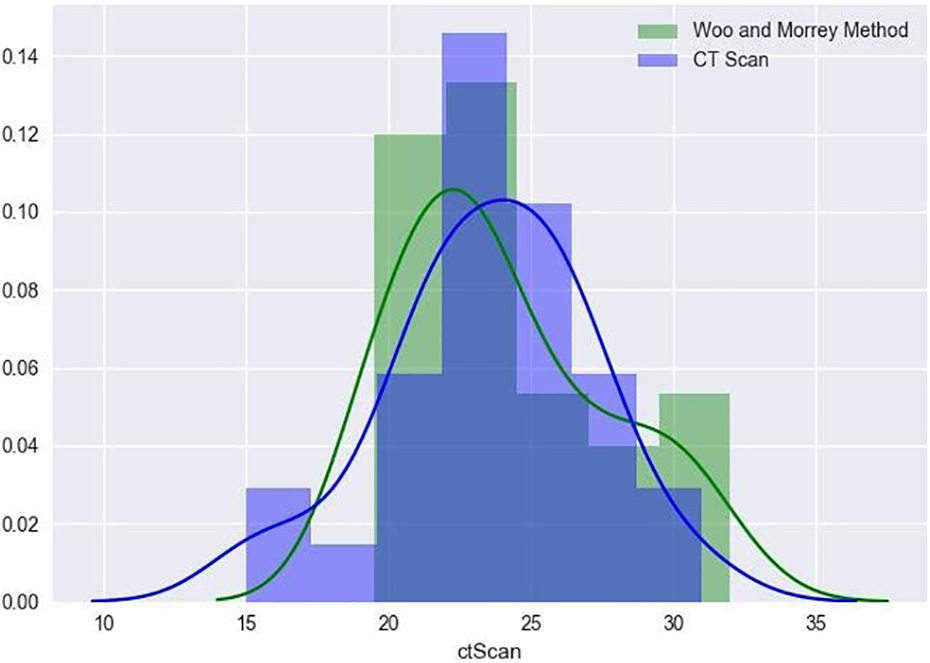
Distribution of the values of the Woo and Morrey method and the CT scan method.
With the help of a paired t-test with an α level of 0.05, we concluded that the difference between the two is not statistically significant (p = 0.272) (Figure 8).
Distribution of the values of the ischiolateral view and the CT scan values is shown in Figure 9. The distributions have a very small overlap and hence suggest a strong significant difference between the two.
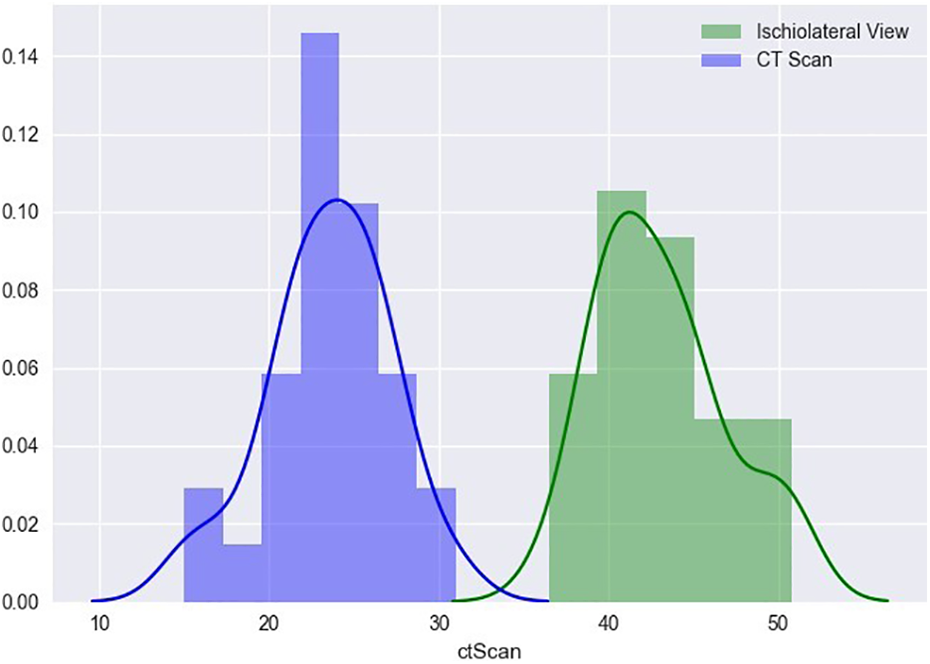
Distribution of the values of the ischiolateral view and the CT scan values.
The results of the paired t-test between ischiolateral views were T-statistic: 33.019 (p = 0.000).
Further, we also found that there was a clear difference between the distribution of the ischiolateral view and the distribution of the CT scan values. We found there was a statistically significant difference between the two distributions at an α level of 0.05 (p < 0.001) (Figure 9).
The relationship between the ischiolateral view and the CT scan method is shown in Figure 10. The regression line presented is y = 2.302 + 0.493 × x with a standard error of 0.066.
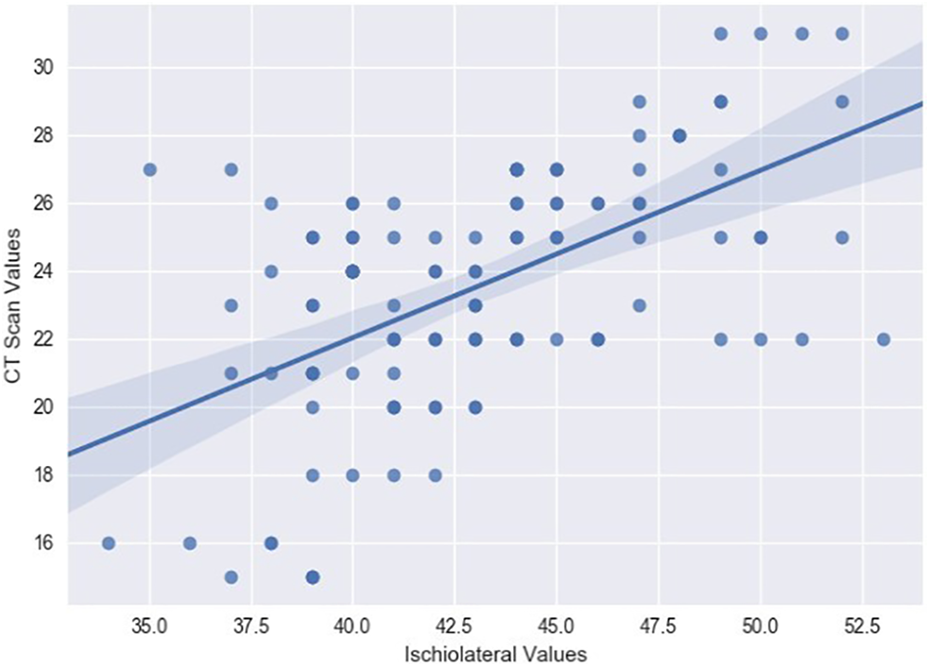
Relationship between the ischiolateral view and the CT scan method.
To study the relationship between the CT scan values (y, independent variable) and the values from the ischiolateral view (x, dependent variable), we calculated the regression line between the two (Figure 10). The regression line was found to be equal to 2.302 + 0.493 (with a standard error of 0.066).
The relationship between the ischiolateral view and the Woo and Morrey method is shown in Figure 11. The regression line presented is y = −9.475 + 0.774 × x (with a standard error of 0.045).
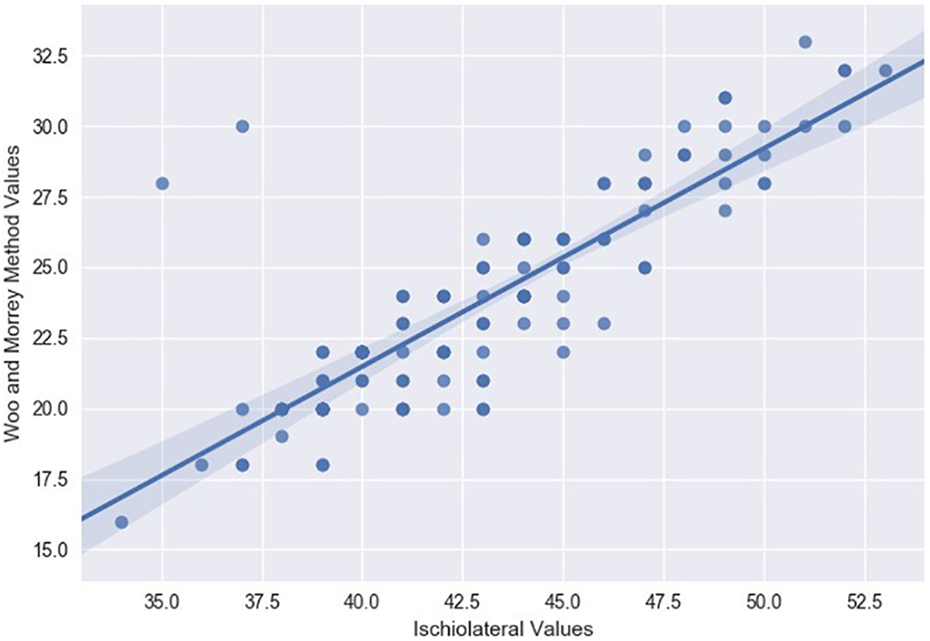
Relationship between the ischiolateral view and the Woo and Morrey method.
Further, we also calculated the regression line between Woo and Morrey method values (y, independent variable) and the ischiolateral view (x, dependent variable) (Figures 11 and 12). The following regression line was found: −9.475 + 0.774 (with a standard error of 0.045).
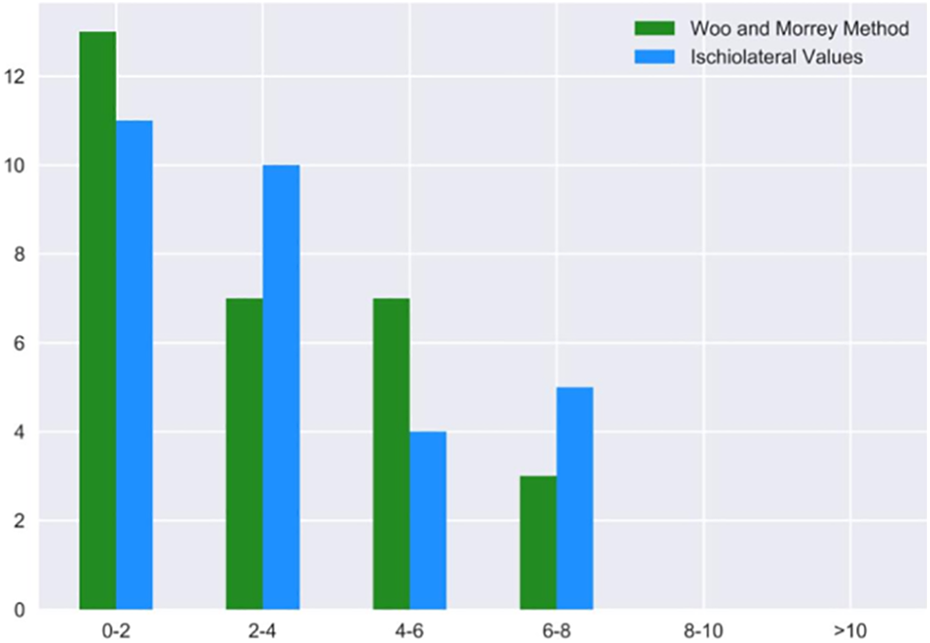
The number of patients on y-axis and standard deviation from the mean values of ischiolateral and Woo and Morrey method on x-axis.
To test the reliability of our observations, we calculated the intra-class correlation coefficient and the mean difference between different observers (inter-observer) and the same observer across different weeks (intra-observer). The results have been reported in Table 1.
Calculation of the intraclass correlation coefficient and the mean difference between inter and intra observer values.
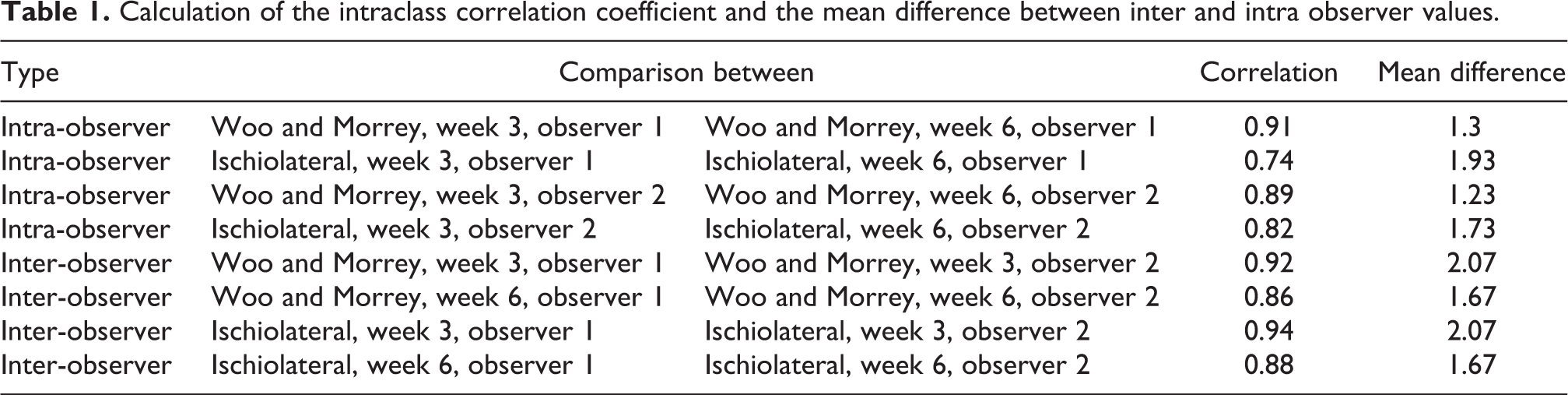
All the pairs were found to be strongly correlated (>0.8, p < 0.001) and the mean difference between the values in different cases was approximately between 1 and 2. This confirmed that the observations were reliable.
Discussion
Knowledge of acetabular component position after THR is important because malposition has been associated with hip instability, impingement, and accelerated wear. 3,4
Acetabular cup inclination can be very well accessed by AP pelvis X-rays; for acetabular version assessment, CT scan is the gold standard. CT scan is not readily available at many centers and the surgeon has to rely on X-ray methods for evaluation of acetabular version to audit results and to predict behavior of the surgical intervention.
Commonly used methods of version assessment on plain radiograph are Lewinnek et al., 4 Widmer, 9 Liaw et al., 10 Pradhan, 11 and Woo and Morrey 3 and ischiolateral method. 7
In this study, we had to determine a radiographical method (Woo and Morrey’s method/ischiolateral method) which is as comparable as CT scan results for the determination of cup version as radiographs are cheaper, associated with less radiation, and are widely available.
While assessing the accuracy of Woo and Morrey method, it was observed that the distribution of Woo and Morrey method values were similar to the distribution of the CT scan values. With the help of a paired t-test with an α level of 0.05, we concluded that the difference between the two is not statistically significant (p = 0.272).
While assessing the accuracy of ischiolateral method, we also found that there was a clear difference between the distribution of the ischiolateral view and the distribution of the CT scan values. We foundthat there was a statistically significant difference between the two distributions at an α level of 0.05 (p < 0.001).
We used the version measured on CT as the reference standard. Previous studies have shown that version of the acetabular component could be measured accurately using CT scans.
As stated in various studies, version measured on AP radiograph (Lewinnek et al.’s, 4 Malik et al.’s, 12 and Liaw et al.’s 10 ) have some limitations like retroversion cannot be detected on AP radiographs. To differentiate between ante- and retroversion, additional oblique or cross-table lateral radiographs are required.
Secondly, it is difficult to identify the apex of the ellipse on AP radiographs when a ceramic or metal liner is used and when the implant is excessively anteverted.
When a cemented ultra-high molecular-weight polyethylene acetabular component, with a radio-opaque circumferential wire, is used, it is easy to identify the apex of the ellipse in AP radiographs.
Woo and Morrey and ischiolateral methods have certain advantages over previous methods. It is easy to measure acetabular anteversion using Woo and Morrey’s method because it does not require equations or conversion tables. It is widely used because it is convenient and fast, and is also safer and more economical than CT. However, it has also some limitations—it is inaccurate when the pelvis is tilted and when the contralateral hip joint or the lumbar spine is stiff.
A limitation of ischiolateral method is that the ischium must be visible on the lateral radiograph. Discussion with the technician regarding the importance of including the ischium on this view should reduce the number of unusable films.
There are limitations to our study. First, there is no gold standard that can be used to validate radiographic or CT-based values in vivo. CT, however, can be considered an acceptable standard for measurement owing to control over pelvic rotation and/or tilt. Second, intraoperative measures of version were not recorded for this cohort of patients. Third, we did not perform multiple CT scans on the same patients because of concern for radiation exposure and availability of CT scan; thus, we have no repeatability data for the CT scans with which we can compare the cross-table lateral radiograph repeatability data.
Conclusion
The purpose of this study was to determine a radiographical method which is as comparable as CT scan results for the determination of cup version as radiographs are cheaper, associated with less radiation, and are widely available.
In this study, Woo and Morrey’s method and ischiolateral method of assessment of acetabular version were compared with CT assessment.
We found that in Woo and Morrey’s method, values were comparable to CT scan values, when put on regression line.
However, in situation of change in patient positioning, namely hip stiffness in contralateral hip, measurement of component position changed in series of radiography due to differences in pelvis tilt. So, in these circumstances, we can use ischiolateral method which can give consistent measurement. But, it will not be in concordance with CT scan values and Woo and Morrey values, as represented in regression line.
Also, in ischiolateral method, it is difficult to appreciate ischium axis on some radiographic films.
The high intra-class correlation coefficients for both intra- and inter-observer reliability indicated that the angle measured with these methods is consistent and reproducible for multiple observers.
CT, however, be considered as gold standard for measurement owing to control over pelvic rotation and/or tilt/patient positioning.
Footnotes
Authors’ Note
Manish Raj is now working as a freelancer.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.