
Abstract
Objectives:
Spinal fusion is an effective treatment for degenerative lumbar spine; however, conflicting results exist regarding the best procedure. This study compares the clinical and radiological outcomes of transforaminal lumbar interbody fusion (TLIF) versus instrumented posterolateral fusion (PLF) in patients of degenerative lumbar spine disorders.
Methods:
Of the total 37 patients, 16 patients were operated with TLIF and 21 were operated with instrumented PLF with bone grafting. Duration of the study was from June 2017 to June 2019. Patients fulfilling the inclusion criteria were included in the study. Inclusion criteria were (1) age of patient ranging from 18 years to 70 years, (2) involvement of single level, (3) diagnosis of degenerative spine disease, and (4) minimum follow-up of 1 year. Radiographic parameters such as slippage of vertebrae, anterior and posterior disc heights, local disc lordosis, T12–S1 angle were measured, and fusion were assessed; comparison between preoperative and postoperative parameters was also done. Clinical outcome score was obtained using visual analog scale (VAS) and Oswestry disability index (ODI). Statistical analysis was done using SPSS software.
Results:
No significant difference was found in ODI and VAS between TLIF and PLF. Restoration of disc height and improvement of local disc lordosis was better in the TLIF group than in the PLF group. The fusion rate was 87.5% in the TLIF group and 81% in the instrumented PLF group. Amount of blood loss was slightly higher in the TLIF group (319.69 ± 53.8 mL) than in the instrumented PLF group (261.19 ± 34.9 mL). Operating time was also slightly higher in TLIF (133 ± 6.02 min) than in instrumented PLF (90.71 ± 6.3 min).
Conclusion:
TLIF is superior to instrumented PLF in terms of restoration of anterior and posterior disc heights and improvement in local disc lordosis and higher fusion rate, however it requires greater surgical expertise and more experience. Because of anterior cage support, early weight-bearing mobilization can be allowed in the TLIF group compared to the PLF group. Surgical time and blood loss were slightly higher in cases of TLIF than instrumented PLF.
Introduction
Methods of spinal fusion continue to evolve in efforts to treat chronic low back pain. Degenerative spine disease may cause severe and chronic low back pain.
According to Matsunaga et al., 30% of patients with degenerative spine disease develop progressive slippage of vertebrae. 1 There are still controversies regarding the role of surgical intervention in these disorders. Lumbar fusion may be required in patients with degenerative spine disease that were refractory to conservative management. Goal of operative treatment is to relieve pain, improve neurological deficit, and show improvement in quality of life. Surgical decompression with fusion with instrumentation provides better outcome as compared to decompression and fusion without instrumentation in terms of additional stability and deformity correction. Various approaches to lumbar interbody fusion have been described like posterior, transforaminal, direct lateral, and anterior.
Two most common surgical procedures are posterolateral fusion (PLF) with instrumentation and transforaminal lumbar interbody fusion (TLIF) with instrumentation. 2 On theoretical grounds, interbody fusion has improved outcomes because of increased surface area for fusion to occur and more suitable vascular environment provided by highly vascular cancellous nature of vertebral body in comparison to PLF. In addition to this, interbody fusion has increased lordosis in short fusions, direct or indirect foraminal decompression and because interbody graft material is placed in load-bearing axis of spine, fusion occurs under compressive force rather than tensile forces. 3,4 The aim of this study was to compare the TLIF and the instrumented PLF with respect to clinical and radiological outcomes in terms of pain, anterior and posterior disc heights, local lumbar lordosis, fusion, blood loss, and operating time.
Materials and methods
This was a type of retro-prospective study with simple randomization/allocation. The allocation was done by picking a folded slip with each group giving a 50% selection probability to each treatment group. Appropriate Institute Ethics Committee clearance was obtained. There were a total of 37 patients, of which 16 were operated with TLIF and 21 were operated with instrumented PLF with bone grafting, having a minimum follow-up of 1 year. Duration of the study was from June 2017 to June 2019. Patients with (i) age ranging from 18 years to 70 years, (ii) involvement of single level, (iii) diagnosis of degenerative spine disease, and (iv) minimum follow-up of 1 year were included in the analysis. Exclusion criteria were (1) age <18 years or >70 years, (2) involvement of multiple levels, and (3) patients with other comorbidities. Investigations like plain radiograph, magnetic resonance imaging, and computed tomography scans were used.
At each follow-up, radiographic parameters such as slippage of vertebrae, anterior and posterior disc heights, local disc lordosis, T12–S1 angle (Figure 1), and fusion were assessed. Comparison was made between preoperative and postoperative parameters. Visual analog scale (VAS) and Oswestry disability index (ODI) were used to assess the clinical outcome preoperatively, postoperatively, at 3 months, 6 months, and 1 year of follow-up.
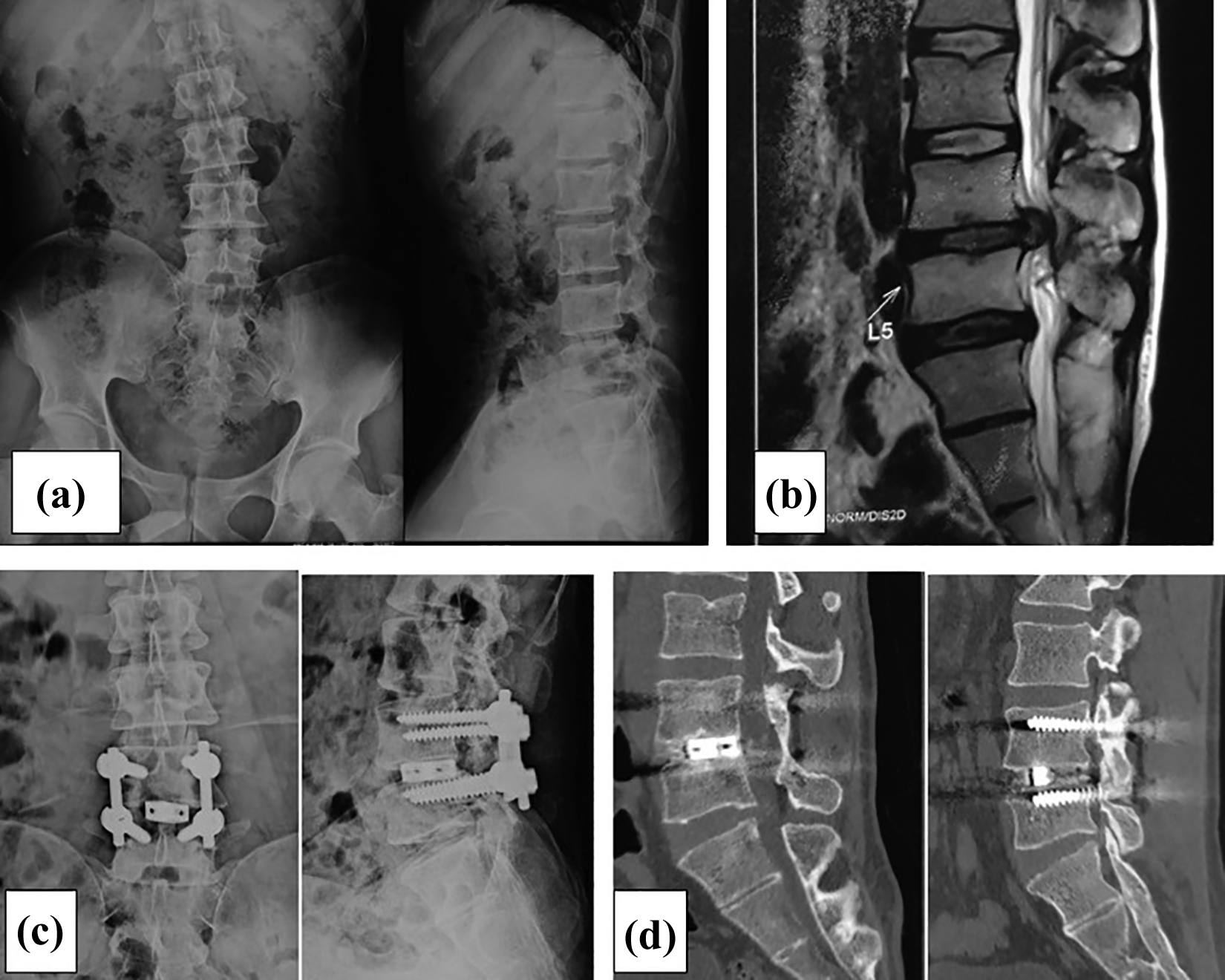
(a) Preoperative radiograph AP and lateral view of a 40-year-old male with back pain and radiculopathy for 2 years. (b) Preoperative MRI showing disc degeneration at L4–L5 level with prolapse. (c) Postoperative radiograph at 1 year showing pedicle screw and cage between intervertebral space. (d) Follow-up CT scan at 1 year showing anterior bony bridge between end plates. AP: anteroposterior; MRI: magnetic resonance imaging; CT: computed tomography.
Radiographic fusion was graded according to Lenke and classified into fusion A, B, C, or D. 5 The fusion in the TLIF group was defined as Lenke A or B (posterolateral) or calcification of the anterior longitudinal ligament (sentinel sign) or central bony bridging between vertebrae in the absence of resorption around implants. Fusion in the PLF group in the present study was defined as Lenke A or B, presence of large solid fusion mass at least unilaterally with smaller fusion mass on contralateral side without loosening of pedicle screw.
Operative procedure
After giving general anesthesia, the patient was shifted to operation table in prone position. Image intensifier was used to confirm the level. An appropriate longitudinal incision was given in midline over involved level. Fascia and muscle were dissected from midline, and retractors were used to expose the posterior vertebral structures. Pedicle screw fixation was done on contralateral side. Unilateral laminectomy was done through lamina and pars of cranial vertebrae of involved disc level, thus exposing the superior articular process of caudal vertebrae and exposing the foramen on the more symptomatic side from which TLIF was planned, and distraction was obtained across the pedicle screws.
Discectomy was done from far lateral entrance point, endplates were prepared, and cage filled with autologous bone graft was inserted. Finally, cage and pedicle screw position were confirmed under image.
Similarly, in PLF after positioning and exposure pedicle screws were inserted and connected with rods on either side of spinous process. Decompression was done and hypertrophic bone spur with ligamentum flavum was removed. Small amount of distraction was done to restore disc height. Bone grafting over transverse process of vertebrae to be fused was done.
Sitting was allowed on fifth postoperative day and ambulation to manage activities of daily living (ADL) was started at 2 weeks in the TLIF group. In the PLF group, in-bed mobilization was allowed as tolerated. Sitting and ADL were allowed only after 4–6 weeks. A lumbar corset was given to provide additional lumbar support. Patient was called up for follow-up at 2 weeks, 6 weeks, 3 months, 6 months, and then 1 year. ODI and VAS scoring was calculated at each follow-up visit and plain radiographs were obtained to assess the union and to look for the position of instruments.
For statistical analysis, t-test was used to compare the radiographical and clinical outcome parameters in two operated groups. For categorical data, comparison χ 2 test was used. Statistical analysis was performed using SPSS software from IBM Corporation.
Results
Demographic and operative date is recorded in Table 1. Radiological and clinical outcomes are compared in Table 2. Case examples are shown in Figures 1 and 2.
Demographic and operative data between the study groups.
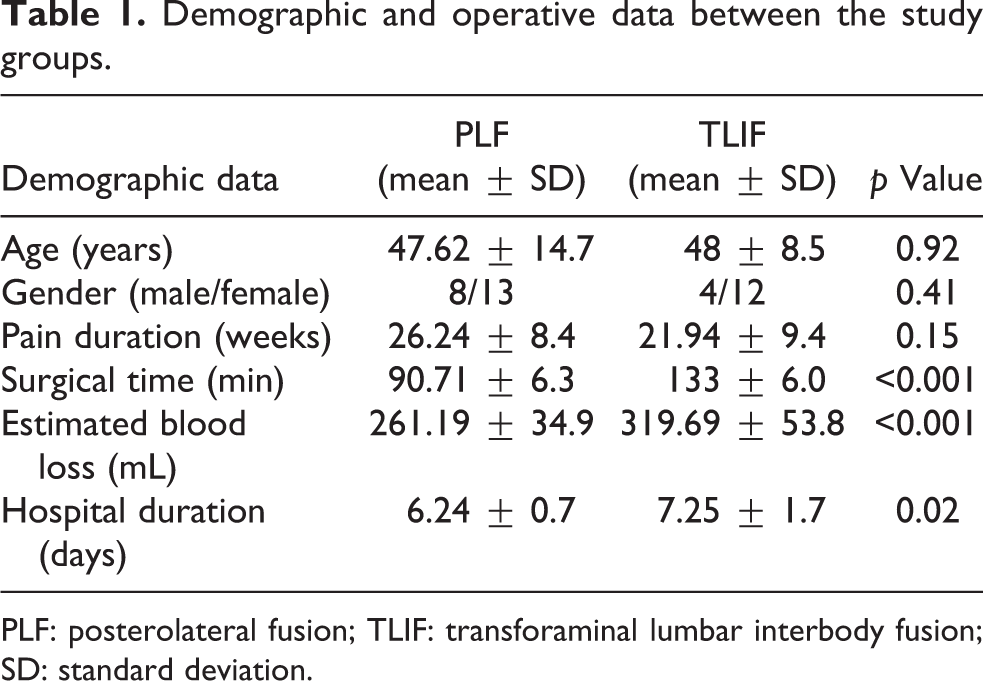
PLF: posterolateral fusion; TLIF: transforaminal lumbar interbody fusion; SD: standard deviation.
Comparison of radiological and clinical outcomes in two study groups.
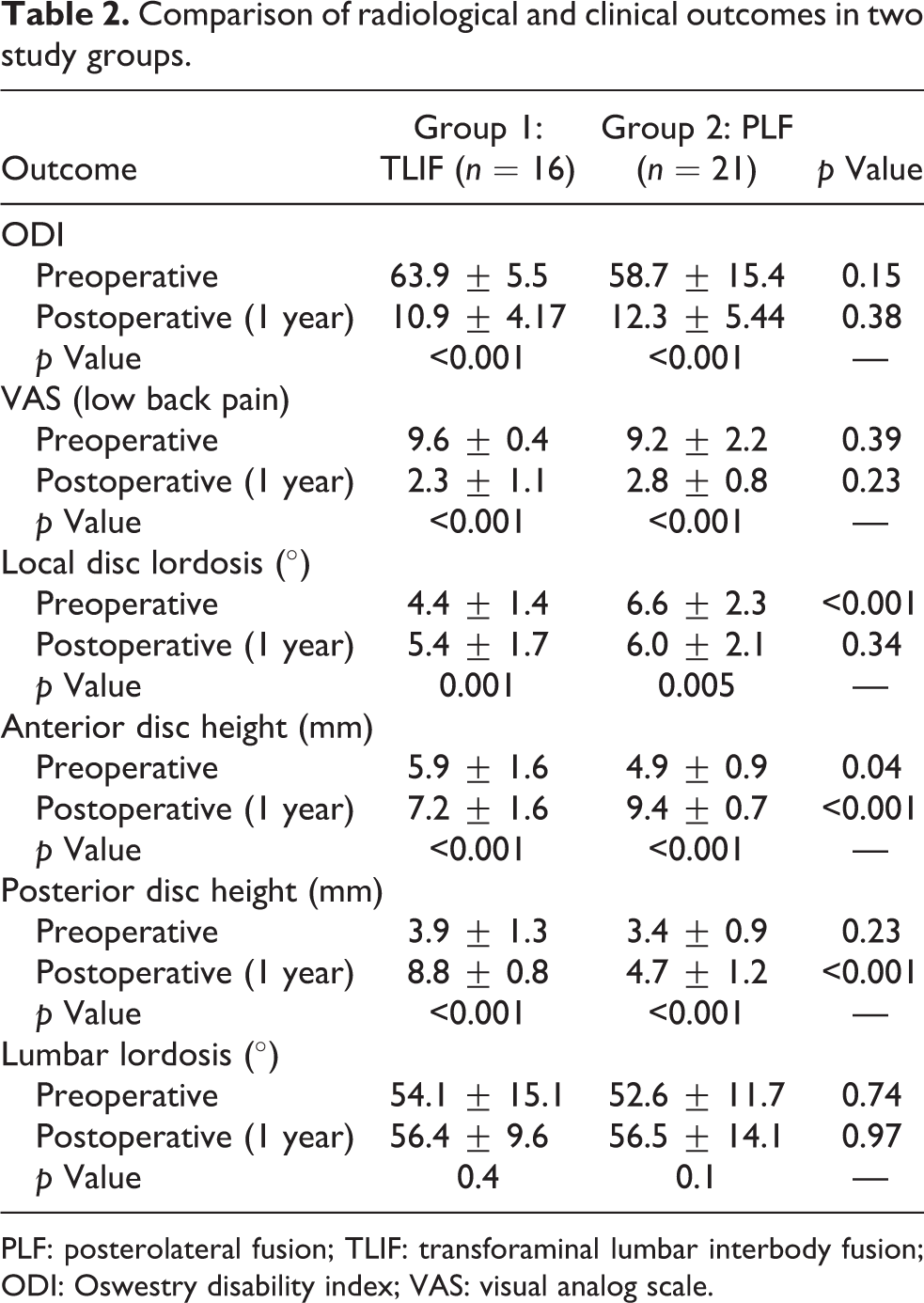
PLF: posterolateral fusion; TLIF: transforaminal lumbar interbody fusion; ODI: Oswestry disability index; VAS: visual analog scale.
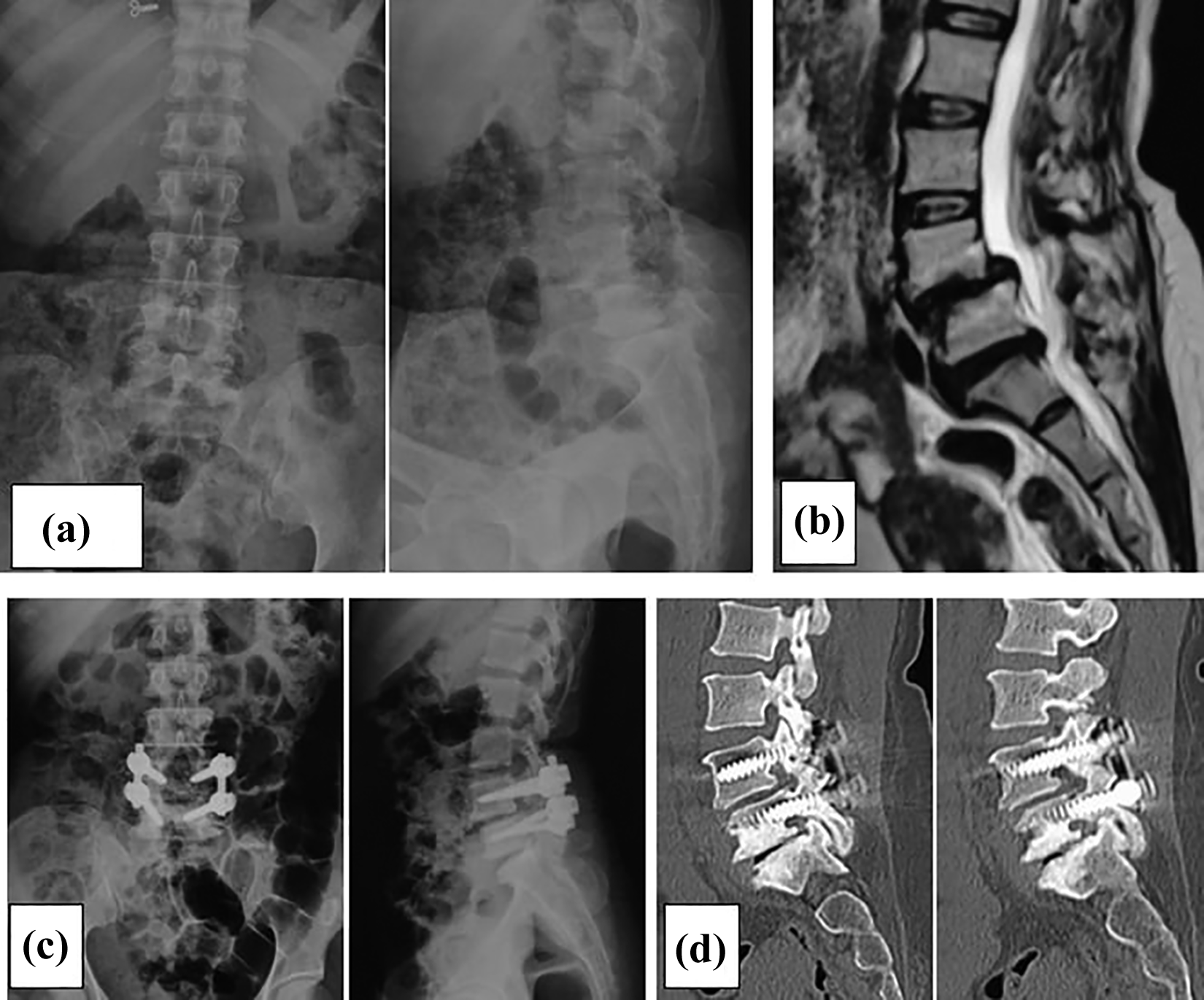
Instrumented posterolateral fusion. (a) Preoperative radiograph showing degenerative changes. (b) Preoperative MRI showing disc degeneration at L4–L5–S1 level. (c) Postoperative radiograph. (d) Follow-up CT scan at 1 year showing bony bridge along the rods. MRI: magnetic resonance imaging; CT: computed tomography.
Discussion
Among all the spinal fusion methods, anterior and posterior combined approach is considered superior because it offers higher stability and maximum chance of fusion. However, nowadays anterior approach is less preferred because it may result in dreadful complications due to close proximity of surgical field to major anatomical vessels. 6,7
TLIF is a widely used procedure because it reduces the risk of cord manipulation as compared to posterolateral interbody fusion (PLIF) and reduces surgical time and morbidity as compared to other fusion techniques like anterior lumbar interbody fusion. The aim of the spinal fusion is to eliminate motion between the two vertebrae, thus eliminating the nociceptive afferents and decreasing the pain.
Harms and Jeszenszky 8 first described TLIF in 1998 as modification of PLIF procedure. They conducted their study on 191 patients and reported excellent results in degenerative spondylolisthesis and moderate result in post-discectomy syndrome and degenerative scoliosis. Furthermore, Videbaek et al. 9 concluded that 360° fused patients had better outcome measured using ODI, SF-36, leg and back pain scores as compared to patients treated with PLF. Fusion rate was 96% in the TLIF group and 84% in the PLF group, with one pseudoarthrosis in the TLIF group and five in the PLF group. Blood loss was nearly equivalent in both groups.
Our study is a single-center study, which increases the possible chances of homogeneous selection of patients and similar surgical techniques. Possible drawback was relatively limited number of patients. It is retro-prospective study of 37 patients with minimum follow-up of 1 year. At the end of the study, it was found that the TLIF group had better outcome in terms of early mobilization, and surgeon was also more confident in allowing early weight-bearing in the TLIF group as compared to the instrumented PLF group. Both groups have significant improvement in clinical outcome compared to their preoperative status in terms of ODI score and VAS.
Hoy et al. 10 showed similar clinical outcome in TLIF and instrumented PLF groups. They conducted study on 96 patients with 48 patients in each group. After 2-year follow-up, fusion rate was 94% in the TLIF group and 88% in the PLF group (p = 0.31). Blood loss and operation time were significantly higher in the TLIF group. There was no significant difference in average hospital days in both groups. Complication rates were significantly higher in case of the TLIF group, that is, 14% as compared to 6% in the PLF group (p = 0.21). In our study, clinical outcomes in terms of ODI and VAS score were similar to Hoy et al.’s investigation. Fusion rate was 87% in the TLIF group and 81% in the instrumented PLF group at 1-year follow-up.
Another study conducted by Shanmugasundaram Pooswamy et al. 11 reported PLF as simpler and safer procedure as compared to TLIF in grade I/II spondylolisthesis. They evaluated 40 cases with comparable age range and sex and reported no significant difference in clinical outcome between the two groups in terms of low back pain rating scale and ODI score. Blood loss was not significant between these two groups. Operative time was on an average 50 min more in the TLIF group than the PLF group (p = 0.02). There was one case of dural tear and one case of injury to nerve root in the TLIF group. One case of pseudoarthrosis was seen in the PLF group due to implant failure. There was no case of deep infection in any of the groups but two cases of superficial infection in the PLF group, which was treated with appropriate antibiotic and resolved completely. The result of our study is also similar to the above study in terms of operative time. Average operative time was 43 min more in the TLIF group than the instrumented PLF group. There was one case of dural tear in the TLIF group and three cases of dural tear in the instrumented PLF group. One case of pseudoarthrosis was seen in the TLIF group.
Another study conducted by Fujimori et al. 12 reported greater improvement in VAS score for leg pain in the TLIF group as compared to the PLF group (3.4 vs. 1.0; p = 0.02), VAS score for low back pain was also significantly better in the TLIF group. There was no significant difference in ODI and preoperative physical component summary improvement in both groups for back pain. There was no significant difference in change of local disc lordosis between the groups: TLIF: 0.1 ± 3.3° versus PLF: 0.3 ± 2.9°; p = 0.9, and the change in disc heights was significant in the TLIF group as compared to the PLF group: TLIF (anterior: 1.4 ± 1.8 mm; posterior: 1.2 ± 1.5 mm) and PLF (anterior: 0 ± 1.7 mm; posterior: 0 ± 1.5 mm), p < 0.01. They also reported no significant change in lumbar lordosis (p = 0.9).
In the current study, slippage reduction and restoration of anterior and posterior disc height were significantly higher in the TLIF group than the PLF group. Change in anterior and posterior disc heights was 4.5 mm and 4.9 mm, respectively, in the TLIF group and 1.34 mm and 1.28 mm, respectively, in the instrumented PLF group. However, many studies have reported that slippage reduction and disc height do not affect the clinical outcome in degenerative spine disease.
Biomechanically anterior placement of interbody cage away from instant axis of rotation maximizes local disc lordosis. Faundez et al. 13 reported anterior placement of cage alone could not improve the local disc lordosis. Compression at posterior element is required which can cause reduction in posterior disc height and foraminal stenosis. In our study, we used banana-shaped cages filled with graft material without any built-in lordosis in cage. Thus, anterior and posterior disc heights are increased with little change in local lordosis and lumbar lordosis. Till now no study had demonstrated the simultaneous increase in posterior disc height and local disc lordosis.
Wu et al. 14 in their study described the fusion rate of 91% and complication rate of 12.6% for open TLIF. In our study, fusion rate was similar in the TLIF group (87%). We found the most common complication to be radicular pain in both the study groups (12–14%). In terms of blood loss and operating time, these were slightly higher in case of TLIF. Mean blood loss was 319.69 ± 53.8 mL in the TLIF group and 261.19 ± 34.9 mL in the PLF group. There was no infection in any group.
Thus, from our study, in operative treatment of degenerative disc disease it can be concluded that both procedures are very effective when performed in well-equipped centers with low complication rates. Instrumented PLF is a simpler procedure but because of lack of anterior support between vertebral end plates, early weight-bearing is a concern specially while using implants, which are locally made.
Conclusion
In conclusion, TLIF is superior to instrumented PLF in terms of restoration of anterior and posterior disc heights, improvement in local disc lordosis, and higher fusion rate; however, it requires greater surgical expertise and more experience. Because of anterior cage support early weight-bearing mobilization is possible in the TLIF group as compared to the PLF group. Surgical time and blood loss were slightly higher in cases of TLIF than instrumented PLF.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.