
Abstract
Study Design:
This is a retrospective cohort study.
Introduction:
Spine procedures are the most expensive surgical interventions on a per-case basis. Previously, orthopedic procedures occurring later in the week have been associated with an increased length of stay (LOS) and consequent increase in costs. However, no such analysis has been performed on common spinal procedures such as minimally invasive lumbar decompression (MIS LD). The purpose of this study is to determine if there is an association between day of surgery and LOS or direct hospital costs after MIS LD.
Materials and Methods:
A prospectively maintained surgical database of patients who underwent primary, single, or multilevel MIS LD for degenerative spinal pathology between 2008 and 2017 was reviewed. Patients undergoing MIS LD were grouped as early in the week (Monday/Tuesday) or late in the week (Thursday/Friday). Differences in patient demographics and preoperative characteristics were compared using χ 2 analysis or Student’s t-test. Associations between date of surgery, LOS, and costs were assessed using multivariate linear regression.
Results:
A total of 717 patients were included. Of these, 420 (58.6%) were in the early surgery cohort and 297 (41.4%) were in the late surgery cohort. There were no differences in demographic characteristics, operative levels, operative time, blood loss, or hospital LOS between cohorts (p > 0.05). Furthermore, there was no difference in total direct costs or specific cost categories between cohorts (p > 0.05).
Discussion:
The timing of surgery within the week is not associated with differences in inpatient LOS or hospital costs following MIS LD. As such, hospitals should not alter surgical scheduling patterns to restrict these procedures to certain days within the week.
Introduction
With the introduction of the Affordable Care Act, health-care providers transitioned from volume-based to value-based care and reimbursement. 1,2 In response, the health-care industry has become focused on minimizing the steadily increasing medical expenditures. However, in order to reform the delivery of health care in a cost-effective manner, the factors that contribute to increased costs must be identified and reduced without sacrificing quality. Although unnecessary tests and procedures are the obvious culprits of increased expenditures, hospital length of stay (LOS) was recently identified as one of the contributing factors leading to the cost burden. 3,4
Spine procedures have been deemed the most expensive surgical intervention on a per-case basis, with a potential for inefficiencies in resource allocation for most relatively healthy patients undergoing surgery. 5,6 The introduction of minimally invasive approaches as an alternative to open procedures has drastically minimized the LOS and costs to the patient and hospital. 7,8 However, surgical scheduling, such as the day of surgery and surgical start time, may also contribute to increased lengths of stay and subsequent costs as demonstrated by studies evaluating hip fractures and total joint arthroplasties. Those surgeries performed earlier in the week were associated with reduced lengths of stay and resulting costs. 9 –12 However, the effect of surgical scheduling on LOS and cost has not been performed on common spinal procedures such as minimally invasive lumbar decompression (MIS LD). Thus, the aim of this investigation is to determine if there is an association between surgery day and LOS or hospital costs after primary MIS LD.
Methods
Patient population
A prospectively maintained surgical database of patients who underwent primary, 1- to 3-level MIS LD for degenerative spinal pathology between 2008 and 2017 was retrospectively reviewed. Lumbar decompressions included any combination of laminectomies, facetectomies, foraminotomies, and/or partial discectomies. The primary indications for patients who underwent MIS LD included progressive motor weakness and extremity pain that was refractory to nonsurgical measures. Patients were excluded if they had preexisting spinal metastases, infectious spinal etiologies, traumatic spine injuries, or if their direct hospital cost data were unavailable. Additionally, patients who experienced any perioperative surgical or medical complications were excluded to ensure that observed variations in LOS and costs were not affected by these occurrences. All surgeries were performed by a single surgeon at a single academic medical center.
Data collection
Patients undergoing MIS LD were grouped according to the timing of their procedures: early in the week (Monday/Tuesday) or late in the week (Thursday/Friday). Demographic and baseline characteristics included age, gender, body mass index, smoking status, insurance status (e.g. Medicare/Medicaid, worker’s compensation, and private insurance), preoperative duration of symptoms (e.g. years) and comorbidity burden measured as Charlson Comorbidity Index. Perioperative variables included operative levels, operation time, estimated blood loss, and length of hospital stay. Patients were discharged once the following criteria were fulfilled and confirmed by the primary health-care team: patient readiness, stable vitals were observed and within objectively normal limits, adequate pain control, voluntary bladder control was established, nausea and vomiting were absent, and when patients were cleared by occupational and physical therapy.
Direct hospital costs were obtained from our institutions’ billing department. Direct hospital costs were expressed as total costs. A subanalysis of the total costs included blood, cardiology, emergency room, radiology, laboratory, nursing unit, intensive care unit, pharmacy, rehabilitation (physical, occupational, or speech therapy), surgical services, and other miscellaneous expenditures.
Statistical analysis
Statistical analysis was performed using Stata/MP® 13.1 for Mac (StataCorp LP, College Station, Texas, USA). Differences in patient demographics and preoperative characteristics were compared using χ 2 analysis or Student’s t-test for categorical and continuous variables, respectively. Associations between date of surgery, LOS, and costs were assessed using multivariate linear regression controlled for age, gender, body mass index, smoking status, and comorbidity burden. Statistical significance was established at p < 0.05.
Surgical technique
All lumbar decompressions were performed identically whether in the hospital or in the ambulatory surgery center. Endotracheal general anesthesia was utilized for all patients. Intraoperative fluoroscopic imaging assisted in identifying the pathologic spinal level(s). A unilateral approach was utilized through a 2- to 3-cm skin incision. Dissection was accomplished to the deep fascia level. This facilitated placement of tubular dilators on the appropriate interspace(s). A 16- or 21-mm non-expandable tube was inserted as the final working portal. Laminectomy with a bilateral partial facetectomy and foraminotomy was accomplished with a high-speed drill. A 3-mm Kerrison rongeur was used to resect the ligamentum flavum. Once decompression was accomplished, the nerve roots were visualized and confirmed to have an excursion distance of at least 1 cm. If patients required discectomy, the nerve root was carefully mobilized medially while the underlying disk fragment was resected with a straight pituitary rongeur and sharp knife.
Results
A total of 717 patients were included in the analysis. Of these, 420 (58.6%) patients were in the early surgery cohort and 297 (41.4%) were in the late surgery cohort. Table 1 demonstrates demographic and baseline characteristics. There were no differences in age, gender, body mass index, smoking status, insurance status, preoperative duration of symptoms, or comorbidity burden between cohorts (p > 0.05 for each).
Demographics and baseline characteristics.
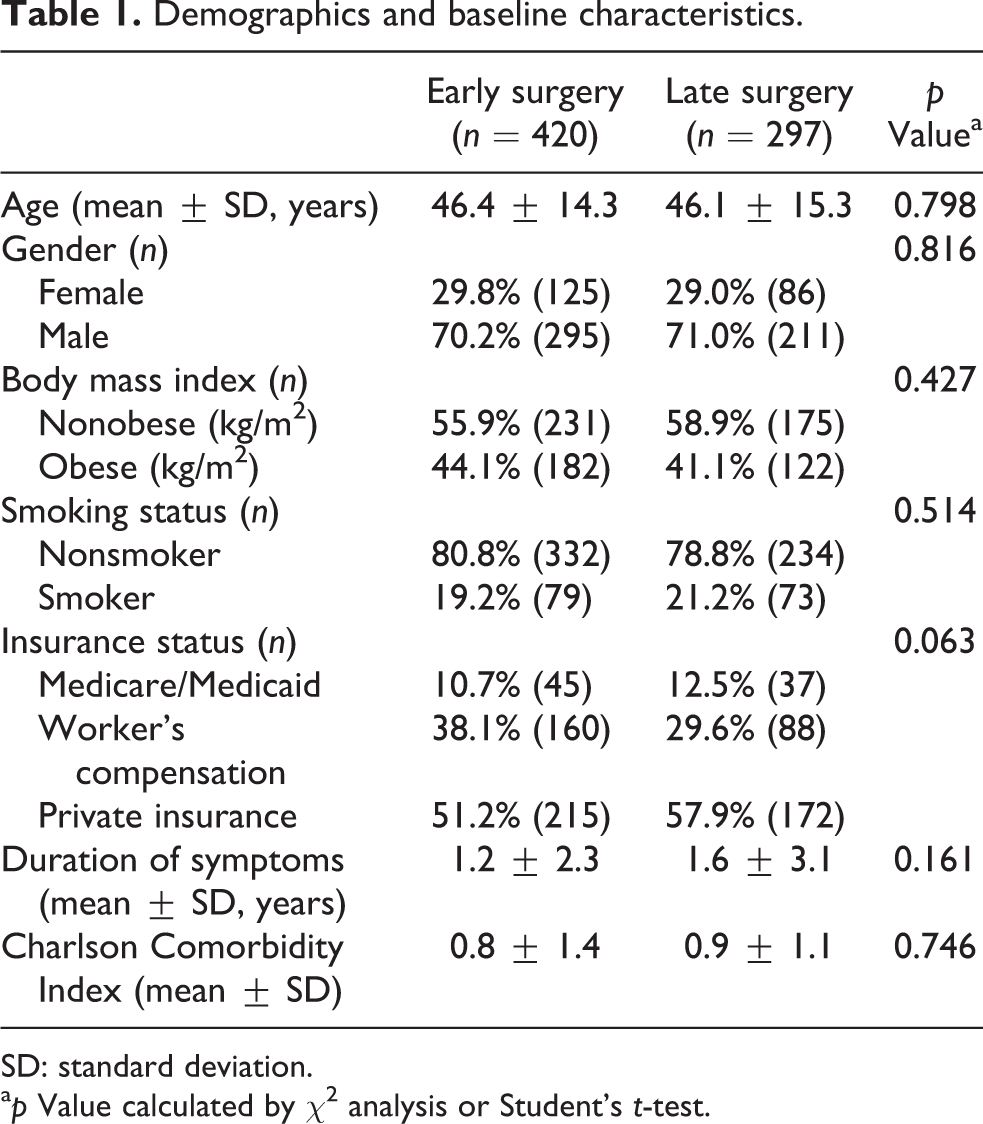
SD: standard deviation.
a p Value calculated by χ 2 analysis or Student’s t-test.
Table 2 compares perioperative characteristics between the two cohorts. There was no difference in the number of operative levels (early surgery: 1-level = 74.6%, 2-level = 21.4%, 3-level = 4.0%; late surgery: 1-level = 71.5%, 2-level = 20.9%, 3-level = 7.6%; p = 0.161), operative time (early surgery: 44.7 min; late surgery: 47.5 min; p = 0.205), or estimated blood loss (early surgery: 41.5 mL; late surgery: 40.6 mL; p = 0.555) between the subgroups. Additionally, there was no difference in hospital LOS between cohorts (early surgery: 11.1 h; late surgery: 12.0 h; p = 0.589).
Perioperative characteristics.
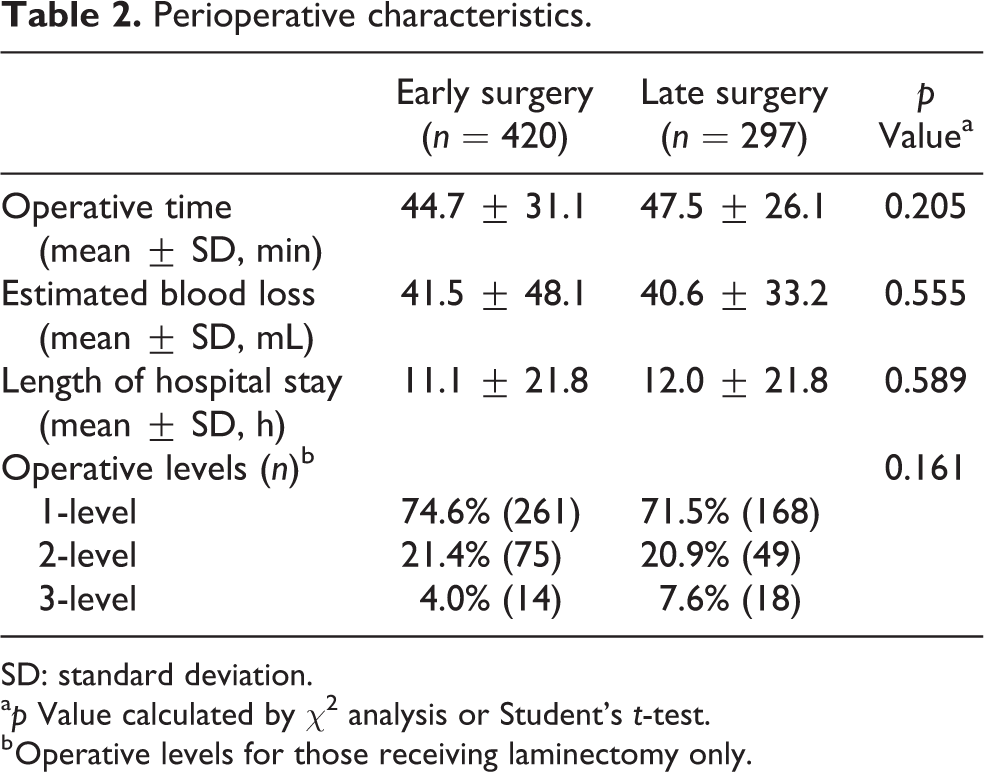
SD: standard deviation.
a p Value calculated by χ 2 analysis or Student’s t-test.
b Operative levels for those receiving laminectomy only.
Table 3 compares the direct hospital costs between cohorts. There was no difference in total direct hospital costs (early surgery: $3496; late surgery: $3324; p = 0.711). After further analysis, there were no differences in subcosts between early and late surgery cohorts (p > 0.05). The highest cost incurred was directly related to surgical services (early surgery: $2725; late surgery: $2546; p = 0.304). No patient incurred costs related to cardiology.
Direct hospital costs.
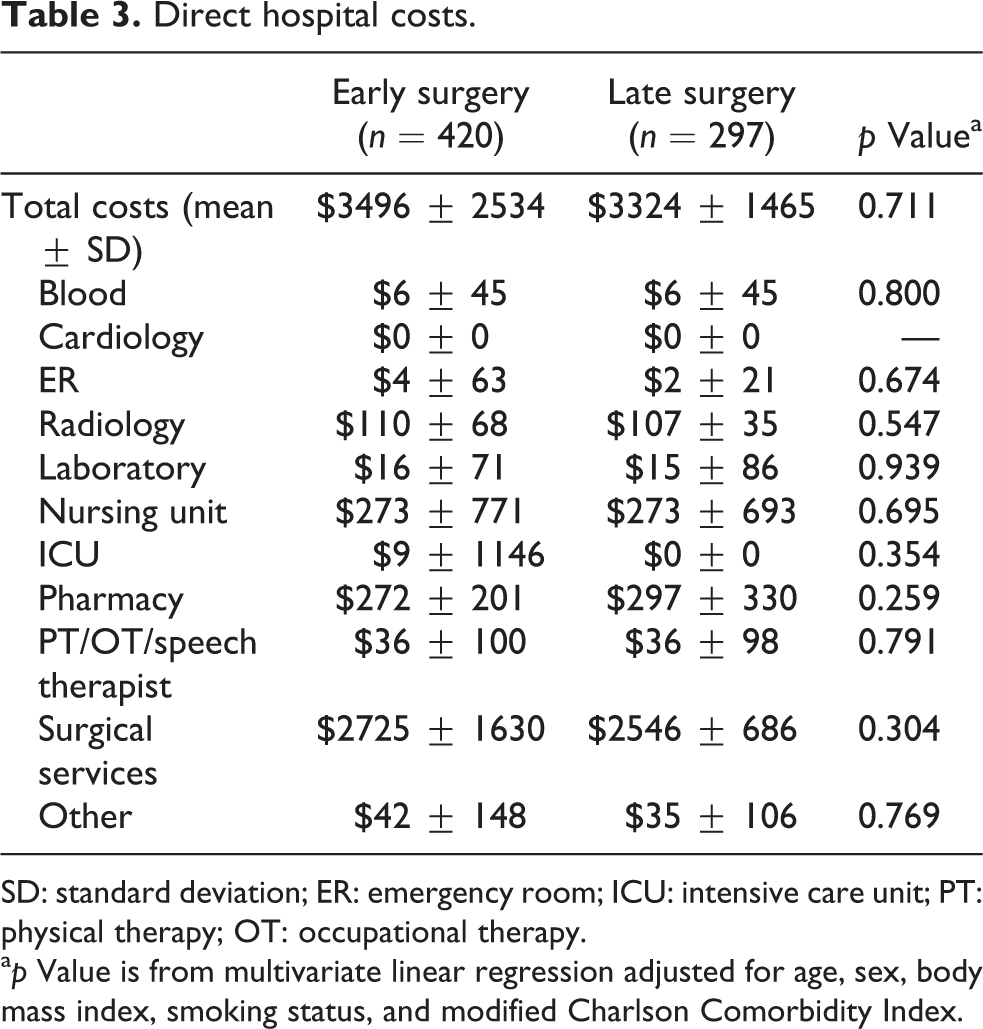
SD: standard deviation; ER: emergency room; ICU: intensive care unit; PT: physical therapy; OT: occupational therapy.
a p Value is from multivariate linear regression adjusted for age, sex, body mass index, smoking status, and modified Charlson Comorbidity Index.
Discussion
The US health-care sector has rebranded itself in the last few decades as its focus has shifted from volume-based to value-based medicine. 13 Hospitals and physicians are constantly searching for methods to increase the quality of care at reduced costs. Within the realm of spine surgery, understanding the itemized costs behind each procedure can assist surgeons and health-care administrators in determining which unnecessary expenses can be avoided. In recent investigations, the timing of surgery during the workweek was established as a potential source of unnecessary costs as LOS and total hospital charges were determined to be greater for procedures scheduled toward the end of the week. 3,4 Thus, we sought to determine if there is an association between the day of surgery during the week and LOS or hospital costs after a primary, single, and multilevel MIS LD.
The results of this study demonstrated that patients undergoing an MIS LD early in the week have similar lengths of hospital stay compared to those undergoing surgery toward the end of the week. Additionally, the direct hospital costs were similar among patients regardless of when they had their surgery. Furthermore, our subcost analysis demonstrated no difference between cohorts with respect to surgical service fees as well as laboratory, nursing, radiology, therapy, and medical subspecialties fees. Although this study exhibits no statistical significance in costs with respect to the timing of MIS LD, it is an important topic to investigate, as other orthopedic specialties have found increases in LOS and subsequent costs when surgery is later in the week.
This was one of the first studies that assessed the impact that day of surgery had on costs and LOS for patients undergoing an MIS LD. Other areas of orthopedics have investigated this topic and, in some cases, have found substantial cost difference. For instance, Lilly et al. examined 2184 patients undergoing either a total hip arthroplasty (THA) or a total knee arthroplasty (TKA) on each day of the week and determined the associated LOS. The authors concluded that patients undergoing procedures on Thursday had a longer inpatient LOS compared to earlier in the week. 3,4 In relation, Newman et al. investigated the effect of day of week of surgery on LOS and direct costs after a primary TKA and THA, demonstrating that procedures performed later in the week exhibited increased total charges. 4
There are a variety of factors that can contribute to the longer LOS in procedures performed later in the week. Patients undergoing surgery later in the workweek, such as a Thursday, are likely to be ready for discharge by the weekend. However, there are typically fewer physical therapists and nurses available on demand during the weekend, which purportedly leads to delayed patient mobilization and recovery. This ultimately results in increasing the LOS and prolonged discharge. 9 Moreover, the roles of discharge planners are assumed by physicians on the weekends, likely lengthening the discharge process. Additionally, certain disposition facilities such as nursing and rehabilitation centers do not accept patients on the weekend. 14
There may be multiple explanations as to why the timing of MIS LD surgery during the week has minimal effect on LOS and direct hospital costs. In relation to traditional open spine procedures, minimally invasive techniques are associated with shorter operative time, less blood loss, and quicker recovery. 15 Compared to the previous studies evaluating THAs and TKAs, patients undergoing MIS LD have much less invasive procedures and on average suffer significantly less pain and are less restricted in mobility in the early postoperative period, allowing for same-day ambulation in most cases. For these reasons, the necessity of physical and occupational therapists may not be as demanding in the immediate postoperative course. In regard to direct hospital charges, the main cost-driving factor in MIS LD is directly related to surgical service, which has little procedural variation.
Since MIS LD is mostly a same-day procedure, cohorts had similar lengths of stay with little fluctuation in postoperative hospital course. The majority of patients included in each cohort were single-level decompressions, 74.6% (261) early surgery and 71.5% (168) late surgery. Many surgeons perform single-level decompressions as a same-day procedure and the patient gets discharged home from the post-anesthesia care unit. Thus, there was no significant difference in costs associated with nursing, physical therapy, and other typical postoperative measures. At this time, there are no recommended changes to the scheduling of patients for MIS LD with respect to the day of the week when considering cost. A population of patients who may require more careful scheduling are those who are at higher risk of experiencing medical or surgical complications. Although not all surgical complications can be predicted, patients with increased medical comorbidity burden are more likely to have complications postoperatively. 16,17
While it may be beneficial to schedule high-risk patients earlier in the week within the traditional hospital setting in order to ensure the full array of support staff are available, our study supports the growing movement to shift appropriately selected patients for many MIS LD to the outpatient surgical setting. The patients we observed were on average, discharged in approximately 12 h. We also observed that day of the week had little influence on hospital LOS. Both the lack of influence of day of the week and the short discharge time are clinically significant because they demonstrate the feasibility of shifting MIS LD to ambulatory day surgery centers. Furthermore, our findings emphasize the need to examine the potential impact of day of surgery on hospital LOS, and to assess overall hospital lengths of stay while estimating the feasibility of day surgery for a given procedure.
This study is not without limitations. While the patients underwent surgeries performed by a single surgeon at a single academic medical center, which allowed for consistency of care, the generalizability and repeatability to other surgeons or surgical centers is unknown. However, the retrospective nature of this study may have introduced an element of selection bias. Additionally, our institution has a standard discharge protocol where social work is contacted and discharge documents are completed in a scheduled manner before the weekend, therefore, our discharge protocols may not be generalizable to other institutions. Additionally, due to limitations of sample size, a subanalysis of costs by the number of operative levels could not be performed. Finally, case selection is of great importance while assessing a patient prior to undergoing outpatient same-day surgery. Ambulatory same-day surgery offers a number of potential benefits, including cost, lessened morbidity, and shorter lengths of stay. However, all of these are only possible through a rigorously tested patient selection criteria. This study was limited in that we did not evaluate a selection criteria for possible ambulatory same-day surgery patients. Future investigations are needed in order to prospectively determine and evaluate the performance of selection criteria for ambulatory same-day surgery patient candidates.
Conclusion
Regarding MIS LD, the timing of surgery within the week is not associated with differences in inpatient LOS or hospital costs. This is probably due to the minimally invasive nature of the procedures, which are mostly same-day surgeries with limited variability of postoperative care. As such, spine surgeons should not restrict the scheduling of MIS LD procedures to certain days of the workweek. Moving forward, other potential sources of cost-inefficiencies should be identified to relieve the cost burden related to MIS LD and other common spinal surgeries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.