
Abstract
Subtalar dislocations are rare and account for about 1% of all dislocations. Standard management is by prompt reduction by closed means, which if unsuccessful, should be followed by open reduction. We present a case report of a closed medial subtalar dislocation in which the talus is internally rotated by 90° and the talar dome formed a pseudoarticulation with the medial malleolus following unsuccessful attempts at closed manipulation and reduction. The patient underwent successful open reduction and fixation and subsequently recovered completely with an American Orthopaedic Foot and Ankle Society hindfoot score of 100 at 5 years after injury. To the best of our knowledge, this is the first case report of a closed talus rotation.
Keywords
Introduction
Subtalar dislocation is a simultaneous dislocation of the talonavicular and talocalcaneal joints, first described by Dufaurest and Judey in 1811. 1,2 Subtalar dislocations are rare and account for about 1% of all dislocations. 3,4 These are usually caused by a high-energy trauma such as motor vehicle accidents and fall from height or by activities such as jumping, running, or twisting. 5 –8 These injuries are more common in males than females. 8,9
We present a unique case report of a closed medial subtalar dislocation that, after three attempts at closed manipulation and reduction, saw the talus internally rotated by 90° such that the talar dome formed a pseudoarticulation with the medial malleolus. To the best of our knowledge, there have been no previous reports of a similar case in which the talus internally rotated 90° in a closed injury.
Case report
A 35-year-old man presented to the emergency department after he slipped and fell from three steps of stairs at work and twisted his right ankle in inversion. X-Rays revealed a medial subtalar dislocation. Talonavicular dislocation was also evident (Figure 1). On physical examination, the ankle was swollen, but the skin was otherwise intact. Neurovascular status was also noted to be normal.
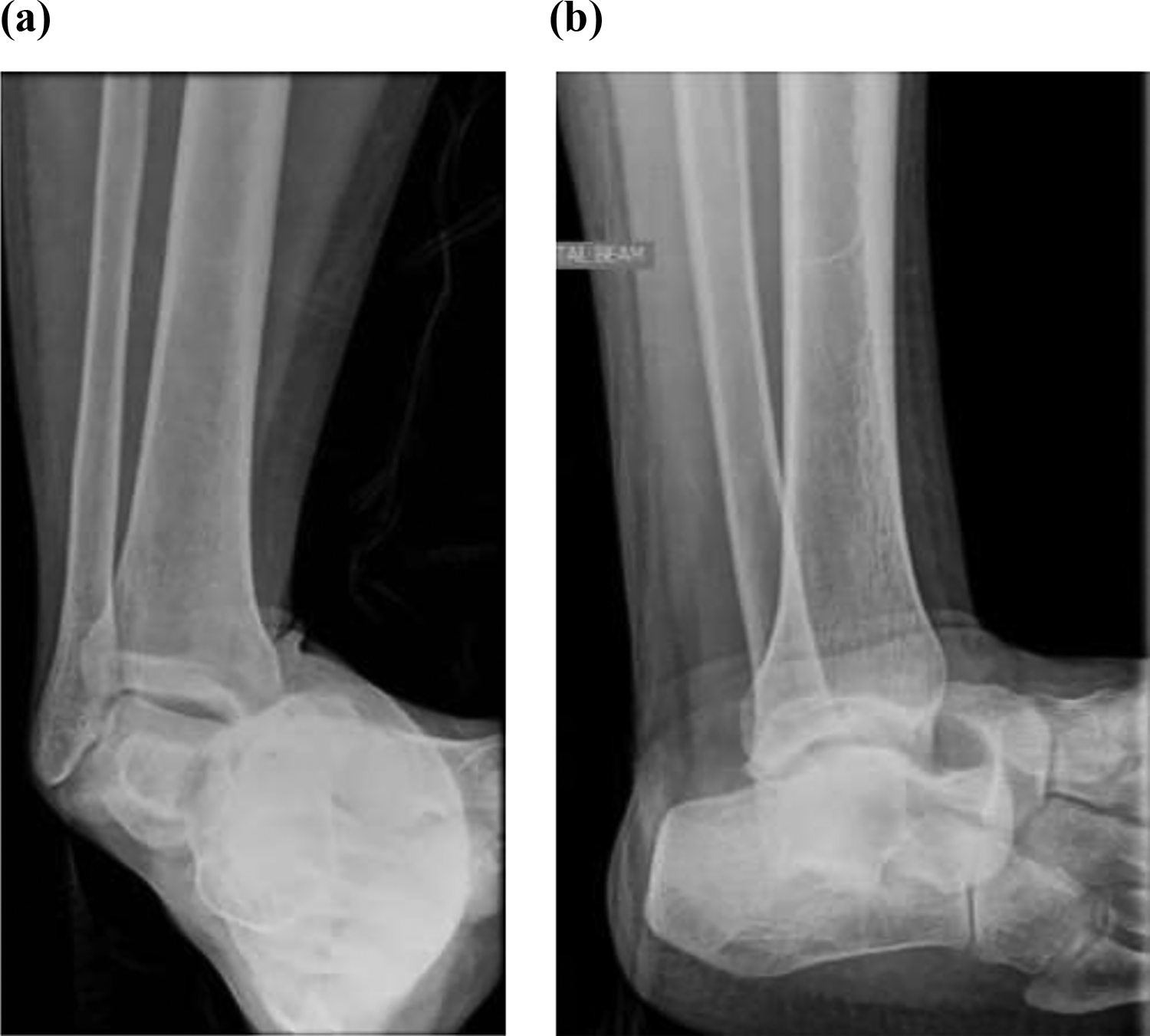
Right ankle (a) anteroposterior and (b) lateral views on presentation.
A first attempt at closed manipulation and reduction was done within 45 min of admission, after which X-rays showed that the talus was internally rotated 45° in the coronal plane, with no reduction of the subtalar dislocation (Figure 2).

Right ankle (a) anteroposterior and (b) lateral X-rays after first attempt at closed reduction.
The second attempt at closed manipulation and reduction also failed, and the talus was noted to be further internally rotated at 80° in the coronal plane, with no reduction of the subtalar dislocation (Figure 3).

Right ankle (a) anteroposterior and (b) lateral X-rays after second attempt at closed reduction.
A third and final attempt at closed manipulation and reduction was attempted, and X-rays showed that the talus was now internally rotated 90° in the coronal plane, and the subtalar dislocation failed to be reduced (Figure 4). The three attempts at closed reduction were performed within a total of 2 h.

Right ankle (a) anteroposterior and (b) lateral X-rays after third attempt at closed reduction.
The details of the method of closed reduction employed during all three attempts were not documented in the available case records but is postulated to be a traction and eversion maneuver under sedation.
A computed tomography (CT) scan of the ankle was only able to be obtained the next morning, 10 h after the third attempt at closed reduction. It revealed that the body of the talus was flipped medially by 90° in the coronal plane such that the talar dome now formed a pseudoarticulation with the medial malleolus. There were associated dislocations of the talocalcaneal, tibiotalar, talofibular, and talonavicular joints and a comminuted fracture of the posterior tubercle of the talus (Figure 5).
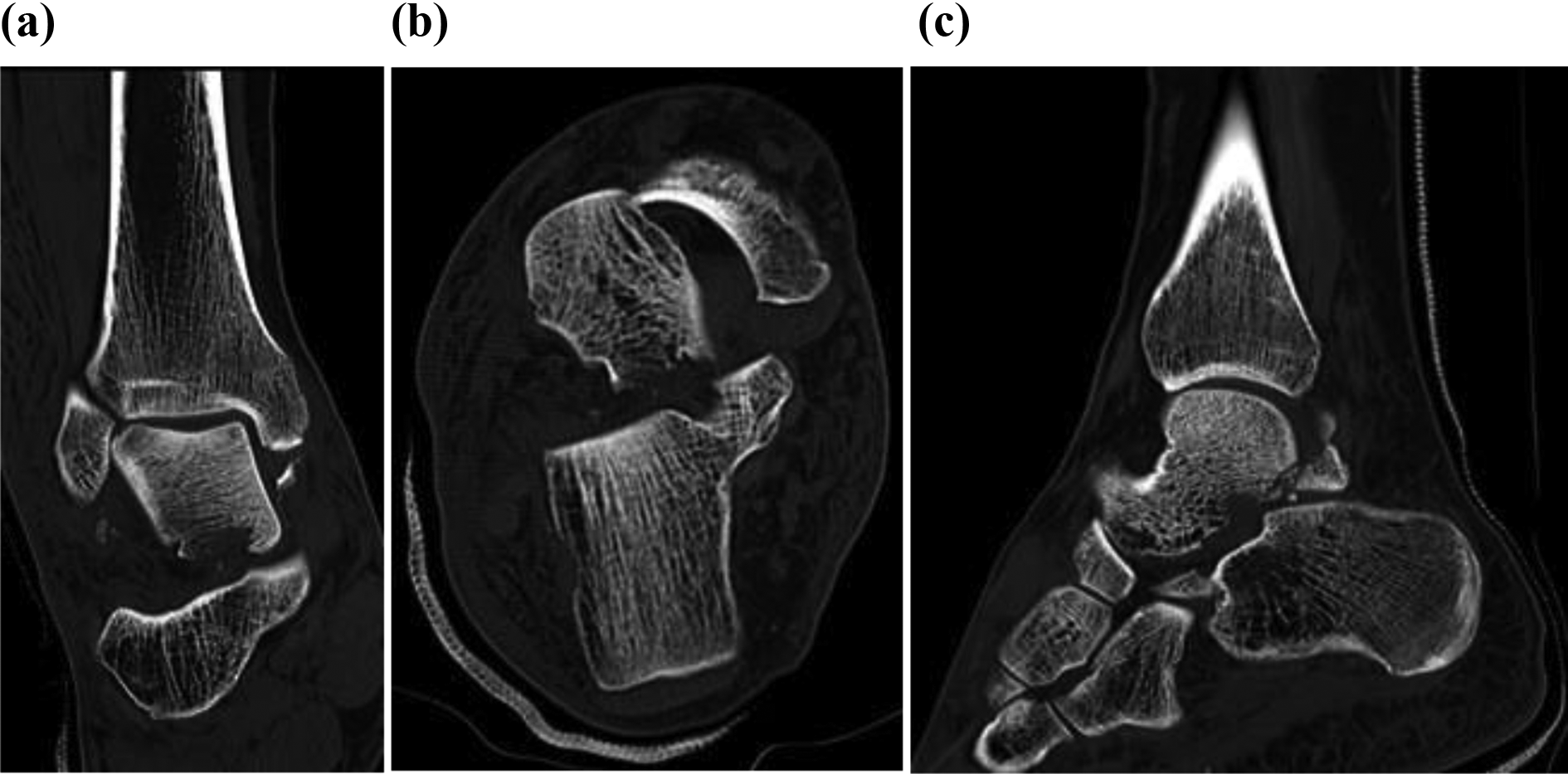
(a to c) CT scan of right ankle after third attempt at closed reduction. CT: computed tomography.
The patient underwent successful open reduction and K-wiring of the dislocated tibiotalar, talonavicular, and talocalcaneal joints (Figure 6). Standard anteromedial and anterolateral incisions to the talus were used, and a total of 4 K-wires were inserted. Intraoperatively, it was discovered that the talus was “free-floating” due to the associated dislocations of the talocalcaneal, tibiotalar, talofibular, and talonavicular joints and a comminuted fracture of the posterior tubercle of the talus as described. The K-wires were removed 5 weeks after index surgery.
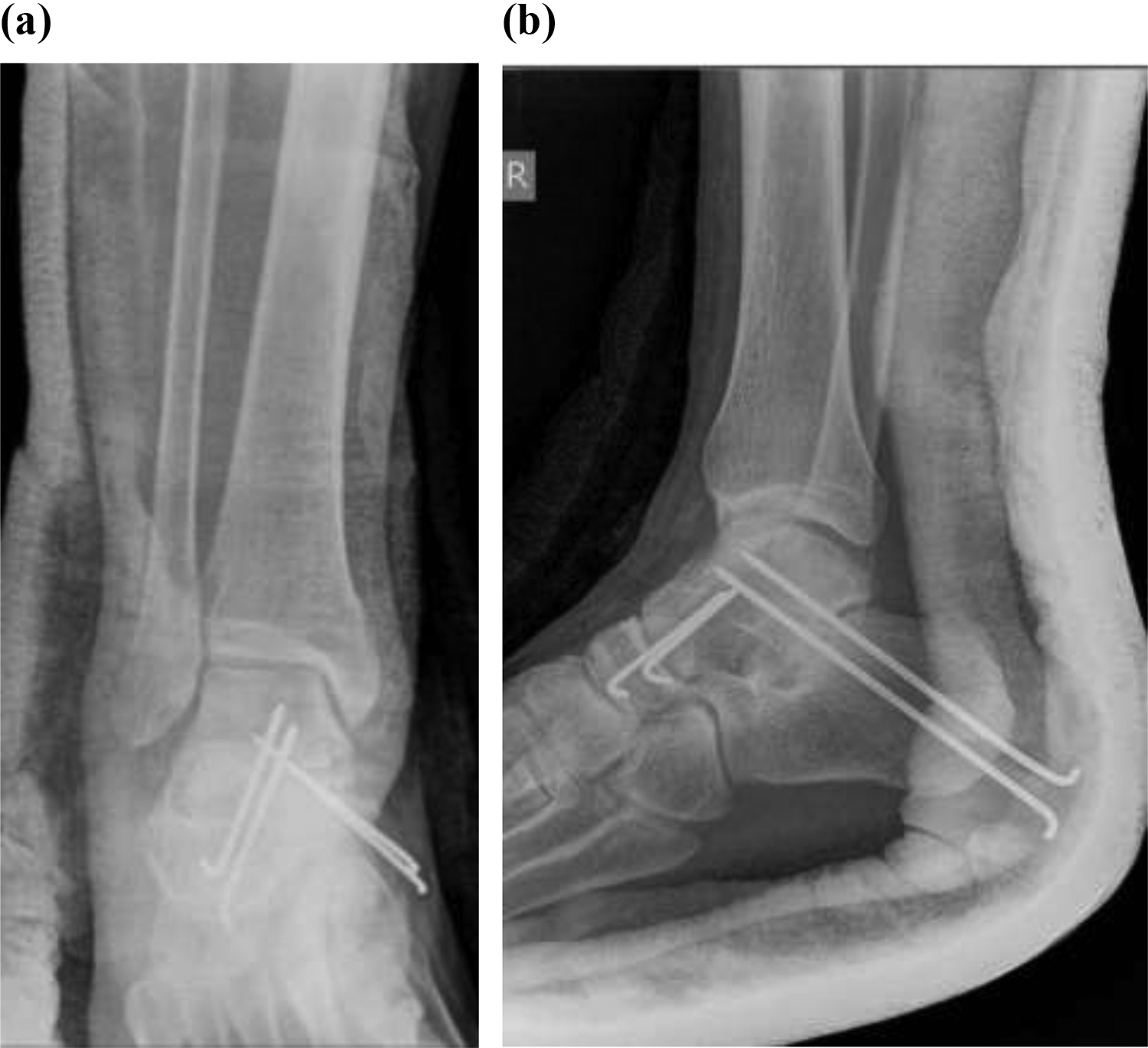
Postoperative right ankle (a) anteroposterior and (b) lateral X-rays following open reduction and K-wire fixation.
The patient returned to full weight-bearing within 3 months after the initial injury. X-Rays at 10 months did not reveal any radiographic evidence of avascular necrosis (Figure 7). At 5-year review, the patient recovered with no disability, could achieve full range of motion in his ankle, subtalar, and midtarsal joints, and his American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot score was 100.
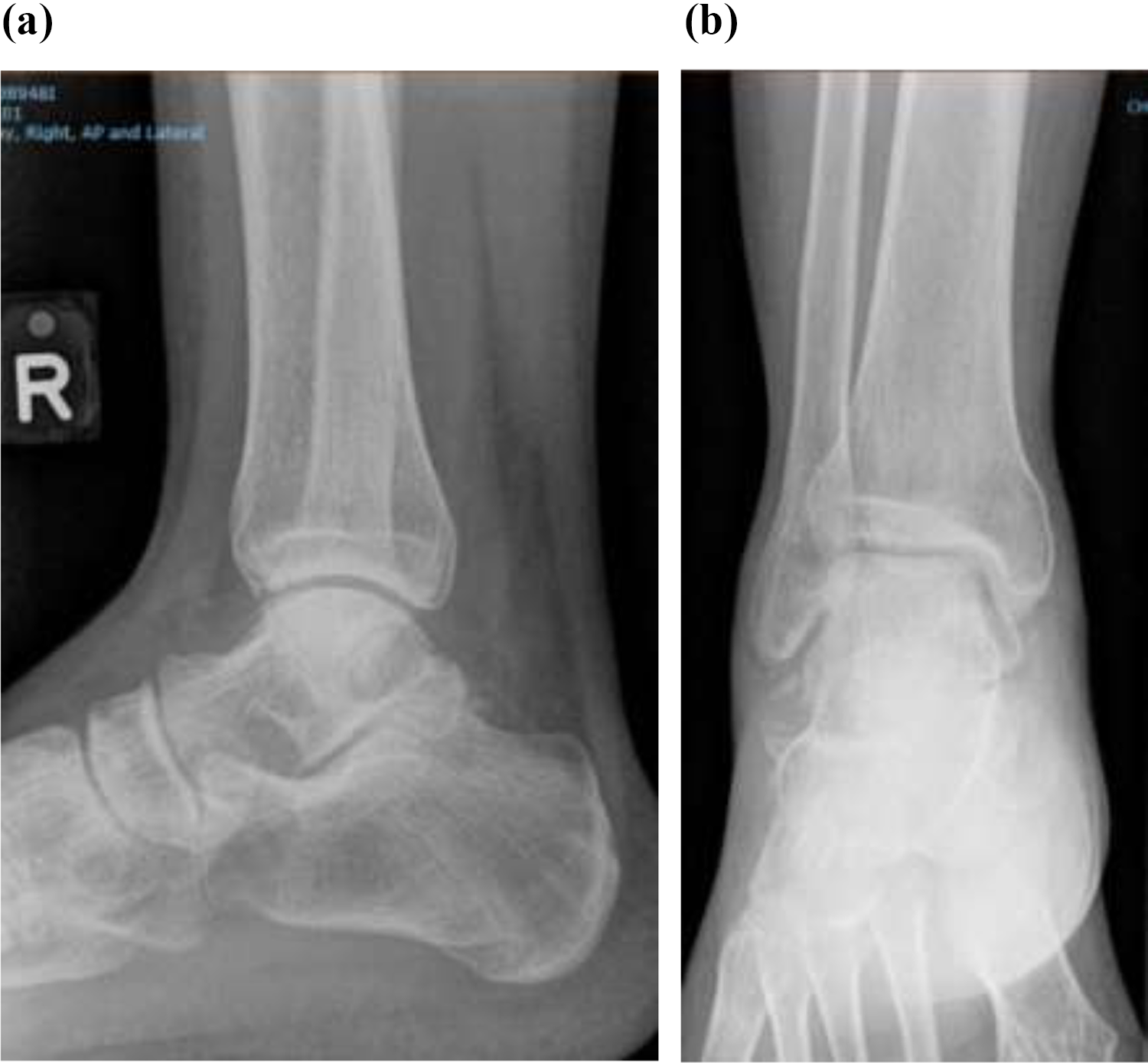
Right ankle (a) anteroposterior and (b) lateral X-rays at 10 months.
Discussion
Subtalar dislocations were first classified in 1853 by Broca, 10 and modified by Malgaigne et al. in 1856. 11 There are four types of subtalar dislocations, classified according to the relative position of the foot to the talus. Medial dislocations are the most common and account for about 70–80% of the cases. This is followed by lateral (about 20%), posterior (about 2%), and anterior (<1%) dislocations. 9,12 –14
In medial subtalar dislocations, inversion forces cause the foot and calcaneus to be displaced medially, with the sustentaculum tali acting as the fulcrum point to lever the calcaneum from the talus. 15 The talar head is prominent dorsolaterally, and the navicular is sited medially and sometimes dorsal to the talar head. 4,14,16
Lateral subtalar dislocations are typically caused by forceful eversion of the foot, with the anterolateral talus pivoting over the anterior calcaneal process. 17 The talar head is commonly displaced through the talonavicular capsule.
Posterior subtalar dislocations are rare and usually occur as the foot is excessively plantarflexed. 18 Anterior subtalar dislocations are the least common and result from forces being transmitted through an excessively dorsiflexed foot. 19
In our unique case, the patient initially presented with a medial subtalar dislocation. However, it would be difficult to classify the dislocation after the multiple failed attempts at closed reduction, as it involved rotation of the talus, which is not described in classification systems.
Associated fractures in subtalar dislocations have been reported in the literature to occur between 50% and 100% of the time, with the talus most commonly affected and are more common in lateral dislocations. 4,8,17,20 Injuries to the deep deltoid ligament in lateral subtalar dislocations and to the calcaneofibular ligaments in medial subtalar dislocations have also been described, with sparing of the spring ligament. 21
Prompt reduction of the subtalar dislocation should be performed after diagnosis has been confirmed. Closed reduction can typically be attempted under sedation in the emergency department.
Failure of closed reduction occurs in about 10–30% of cases of subtalar dislocations. 4,8,22 Irreducible subtalar dislocations are more commonly lateral than medial. 8 Inability to obtain closed reduction is often due to soft tissue interposition (e.g. extensor digitorum brevis, peroneal tendons, and joint capsule) or interference by osteochondral or chondral elements of the talonavicular and talocalcaneal joints. 8 , 23 A cadaver study supported the entrapment of the talar head in the extensor retinaculum, talonavicular impaction, and impingement of the deep peroneal nerve and associated dorsalis pedis arterial branches between the talus and the navicular as causes of irreducible subtalar dislocations. 24
In the case of our patient, we postulate that closed reduction attempts of the subtalar dislocation proved futile due to possible soft tissue interposition. Forceful closed reduction eversion maneuvers only served to eventually cause an iatrogenic dislocation of the tibiotalar joint.
Open reduction is required if closed reduction is unsuccessful. 4,25,26 Reduction should be followed by repeat radiographic assessment and CT scans to evaluate associated osteochondral fractures. 27
It is important to recognize the anatomy of the talus and its relation within the ankle mortise. In the case of our patient, repeated attempts at closed reduction should not have been carried out as soon as it became evident that successful closed reduction would prove difficult, due to the low likelihood of success as well as the possibility of iatrogenic complications. The internal rotation of the talus by 90° was caused by multiple attempts with misdirected excessive force. It is important for the clinician to recognize that the direction of force is inappropriate and to resist further attempts at closed reduction.
Most studies found that restriction in range of subtalar motion is a common complication in treated subtalar dislocation, which is seen in up to 80% of patients. 4,17,28 Despite this, most patients with treated subtalar dislocations recover without significant disability. 4,17,29 Bibbo et al. found that at the mean follow-up of 5 years, there were radiographic changes of the subtalar joint in 89% of patients, and 75% of these patients suffered an associated peri-subtalar joint fracture at the time of injury, while the midfoot showed radiographic changes in 72% of patients.8
At 5-year follow-up, our patient is doing well and has successfully taken up recreational long-distance running with no symptoms. His AOFAS hindfoot score was 100.
Conclusion
Closed subtalar dislocations can usually be managed by prompt closed reduction following diagnosis. In attempting closed reduction, it is important to have intimate knowledge of the anatomy of the talus and its relation within the mortise and to recognize the direction of forces. If reduction by closed means proves difficult, open reduction should be performed. Soft tissue and osteochondral interposition are obstacles to reduction. Repeat radiographic assessment and CT scans should be performed to evaluate for associated fractures. Outcomes in treated closed subtalar dislocations are mostly favorable. Our patient healed without any sequelae at 5 years after injury with an AOFAS hindfoot score of 100.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.