
Abstract
Purpose:
The purpose of this study was to assess the outcomes of a cohort of local Chinese patients who underwent oblique lumbar interbody fusion (OLIF) surgery for lumbar degenerative diseases.
Methods:
We adopted a minimally invasive anterior approach to the lumbar spine through retroperitoneal access. In the first part of the surgery, a 3- to 5-cm left lateral incision over the abdomen was made guided by imaging. L2–L5 disc space was approached via the corridor between the left psoas muscle and the great vessels. A specially designed interbody cage filled with bone substitute was utilized for interbody fusion. In the second part of the surgery, posterior instrumentation with or without decompression, was performed in a prone position. Efficacy and safety of the surgery were studied.
Results:
A total of 60 patients with the mean age of 68 years underwent OLIF at 83 surgical levels. Their mean operative time was 79 min, and the average blood loss was 84 ml for the OLIF part. The mean length of hospital stay was 5.5 days. Based on plain computed tomography scan obtained at post-operative 6 months, successful fusion was achieved in 82 of the 83 surgical levels. The Oswestry Disability Index for low back pain had a mean reduction of 22.3% after 6 months. Specific complications observed include transient thigh pain or numbness, retroperitoneal hematoma, post-operative ileus and Bone Morphogenetic Protein (BMP) osteolysis. None of the patients experienced infection, symptomatic pseudo-arthrosis, hardware failure, vascular injury, nerve injury, ureteral injury, bowel injury, incisional hernia or death.
Conclusion:
OLIF is an effective procedure to treat lumbar spinal stenosis and spondylolisthesis with excellent fusion rate and good functional outcome. Complications specific to this procedure are not uncommon, but majority are minor and self-recovery. Proper training is required to minimize potential surgical risks.
Introduction
The first anterior lumbar fusion for treating lumbar spinal disease was described at the 1930s by Burns and Capener. 1,2 Posterior lumbar interbody fusion (PLIF) was described at the 1940s, 3 followed by the introduction of trans-foraminal lumbar interbody fusion (TLIF) at the 1980s. After the introduction of pedicle screws as well as interbody cages at the 1990s, 4 instrumented open TLIF using open pedicle screws and cage became one of the most commonly performed spinal operations in the past two decades.
Minimal invasive techniques for spinal fusion surgery have gained much popularity in the 21st century, with advantages of smaller wounds, less blood loss and faster post-operative recovery. Percutaneous TLIF using tubular retractor and percutaneous screws has proved to be safe and effective in many studies. 5 Recently, many surgeons started to think about a larger cage for potential better fusion and alignment correction. The extreme lateral interbody fusion (XLIF) was first introduced by Pimenta in 2001, 6 which can access the lumbar spine via a lateral approach, passing through the psoas major muscle. However, nerve injury is a known potential devastating complication of XLIF, as majority of the lumbosacral plexus travels within the posterior part of the psoas major muscle. Therefore, real-time electromyography (EMG) monitoring is required during the procedure. 7
Mayer first described a minimally invasive anterolateral approach to the lumbar spine through retroperitoneal access for L2–L5 discs via a corridor between the aorta and the psoas muscle at 1997. 8 Later, OLIF has been applied with cages developed by Medtronic as reported in 2012. 9 Followed by subsequent developments, the improved OLIF system (OLIF25) has been proved to be a safe and effective method to achieve good surgical outcomes in overseas studies.
However, results and complications of this OLIF surgery have not been reported in our local population. Recruiting patients with OLIF25 was performed in our centre from 2016 to 2018, and this study is conducted to examine the efficacy and safety of OLIF surgery in treating degenerative lumbar spinal stenosis, in terms of operation time, blood loss, hospital stay, fusion rate, functional scorings and complications.
Methodology
A retrospective review was performed on 60 patients who underwent OLIF surgery between January 2016 and December 2018 in the same centre. The inclusion criteria were single or multilevel OLIF from L2–L5 for the treatment of degenerative lumbar spinal stenosis. Patients with infection, malignancy and traumatic fractures of the thoracic and lumbar spine were excluded. Patients who underwent OLIF51 surgery to L5/S1 were excluded (Table 1).
Demographic characteristics.
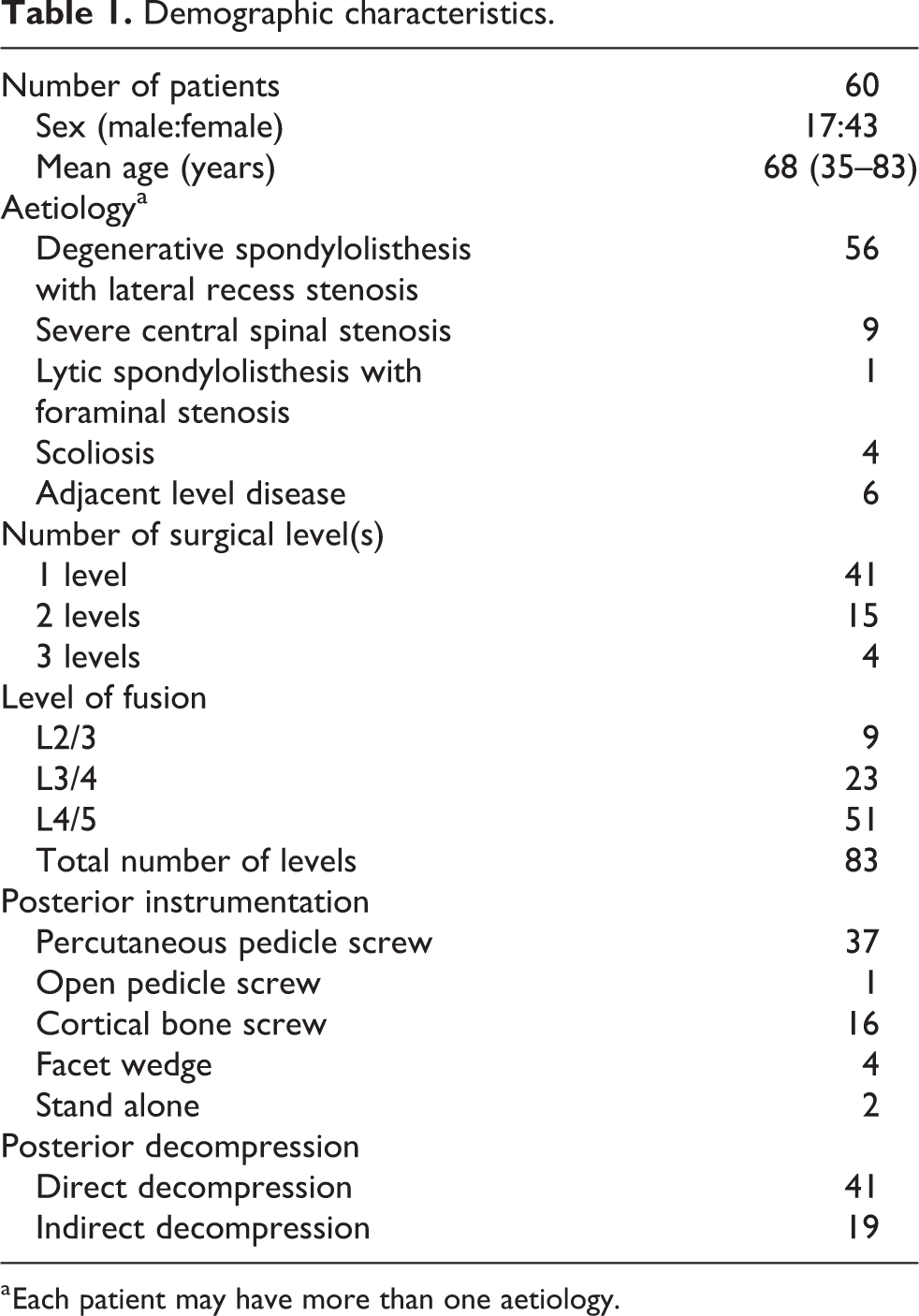
a Each patient may have more than one aetiology.
During the surgery, the patient was positioned laterally. A 3- to 5-cm (depending on the number of surgical levels) left lateral incision is made under image guidance. The abdominal muscles including external oblique, internal oblique and transverse abdominal muscles are then split. Upon entering the retroperitoneum space, peritoneum and ureter were swept anteriorly, while the psoas muscle was retracted posteriorly with the help of special retractors. With direct visualization of the disc, dilators and retractors were inserted. Disc space was then entered, followed by annulotomy, discectomy and end plate preparation. Trial of interbody cages was performed with correction of sagittal alignment attempted. Finally, a specially designed interbody cage filled with bone substitute was placed at the disc space (Table 2). The skin wound was then closed, and the patient was turned to prone position for the second part of the surgery – posterior instrumentation with direct or indirect decompression. Open pedicle screws, percutaneous pedicle screws, cortical bone screws or facet wedge were used in posterior instrumentation. Direct posterior decompression was performed either by open laminectomy or through a 16-mm tube as a minimally invasive procedure.
Cages and bone substitutes used in OLIF.

OLIF: oblique lumbar interbody fusion; PEEK: polyetheretherketone; DBM: demineralized bone matrix.
X-Rays and plain computer tomography (CT) were used for evaluation of alignment and complications after surgery. CT was performed 6 months (± 2 weeks) after surgery to evaluate fusion and subsidence. Fusion was considered successful if there was bridging trabecular bone between the vertebral bodies of interest, irrespective of the status of facet fusion. 10 Cage subsidence was defined as breaching of an end plate immediately adjacent to an intervertebral device, causing greater than or equal to 2 mm loss of height. 11
To assess the functional outcome, physiotherapist recorded the Oswestry Disability Index (ODI) for low back pain before the surgery, 6 months and 2 years after surgery. 12 Pain visual analogue scale (VAS) for back pain and leg pain and results of 6-minute walk test (6MWT) were recorded as well.
Results
A total of 60 patients underwent OLIF25 at 83 surgical levels. L4/5 level was the most commonly operated (61%). There were 17 men and 43 women, with ages ranging from 35 years to 83 years (mean age 68.4 years). The operative time for OLIF part range from 30 min to 195 min (mean time 79 min), and the average blood loss was 84 ml. Forty-one patients (68%) underwent direct posterior decompression during posterior surgery. Nineteen patients (32%) did not require direct posterior decompression, and indirect decompression was achieved by anterior interbody fusion. For the posterior part of the surgery, the average operative time was 133 min and the average blood loss was 229 ml. Length of hospital stay ranged from 2 days to 18 days (mean 5.5 days).
Based on plain CT scan obtained at 6 months after surgery, successful fusion was achieved in 82 of the 83 surgical levels. Cage subsidence was noted in 10 levels, ranging from 2 mm to 7 mm, with 4.4 mm subsidence on average. Fusion at 6 months was failed at L4/5 level in a patient undergoing OLIF surgery on two levels. It was associated with loss of reduction of retrolisthesis, yet neurological symptoms of this particular patient still improved as direct posterior decompression was performed. Follow-up CT scans of this patient at post-operative 8 months showed successful fusion with no further loss of reduction.
Concerning the correction of deformity, segmental lordosis had an increase of 4.7° per level in average (Figure 1). Among the 68 operated levels with spondylolisthesis, complete reduction of slip was achieved in 38 levels, while partial reduction was achieved in 26 levels, including two levels with grade 2 slips reduced to grade 1 slips (Figure 2). For the four patients with mark lumbar scoliosis (Cobbs’ angle over or equal to 15), their average Cobb’s angle improved from 20 to 14.
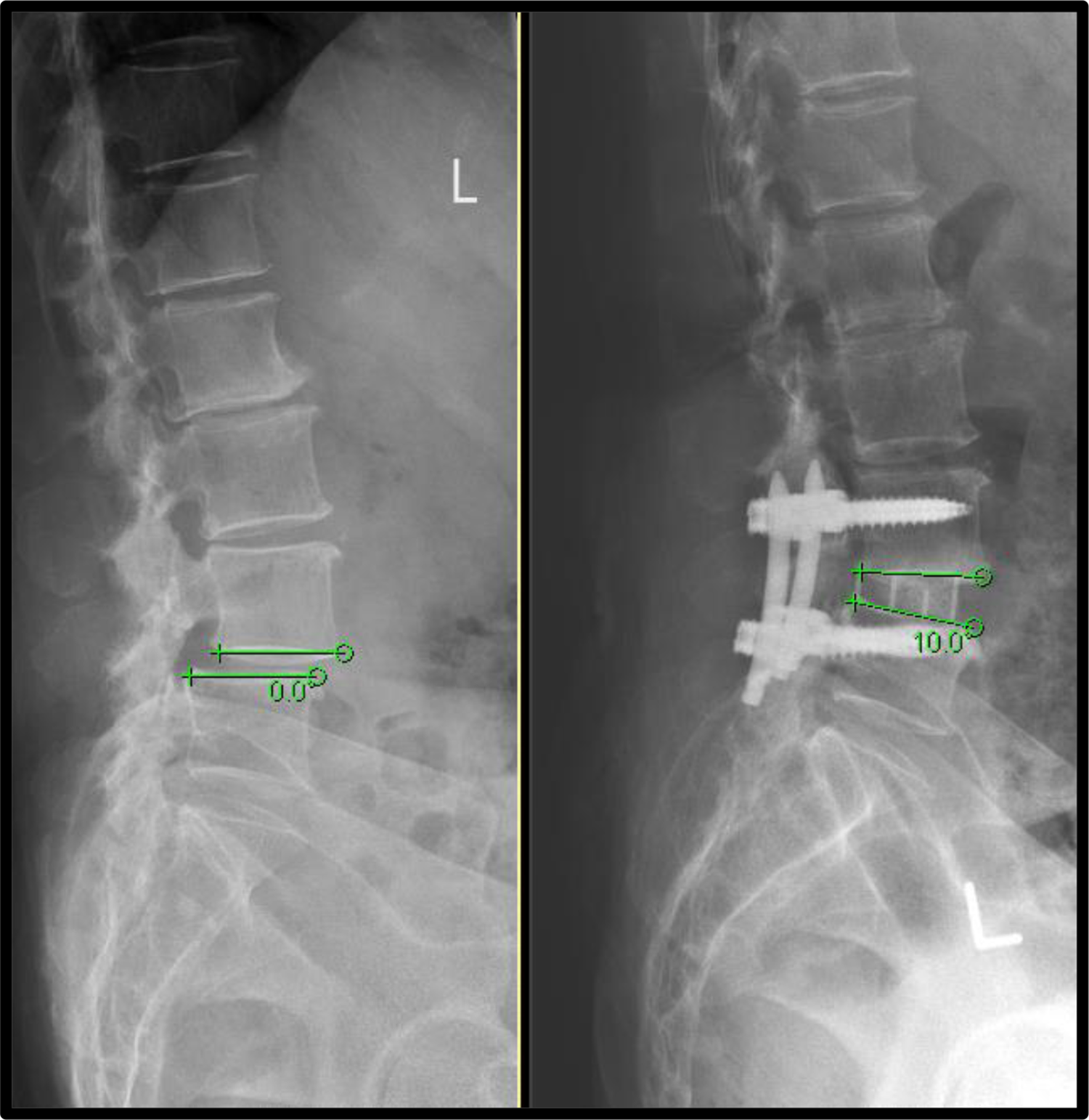
Improvement in segmental lordosis after L4/5 OLIF. OLIF: oblique lumbar interbody fusion.
Complete reduction of L3/4 grade 1 slip. Partial reduction of L4/5 grade 1 unstable slip.
Among 49 patients who completed the whole course of physiotherapy and assessments, ODI was improved in 42 of them (86%) at post-operative 6 months, with an average reduction of 22.3%. The mean VAS for back pain improved from 5.8 to 3.2, while VAS for leg pain improved from 5 to 2.
Results of operative outcomes are listed in Table 3.
Operative outcomes.
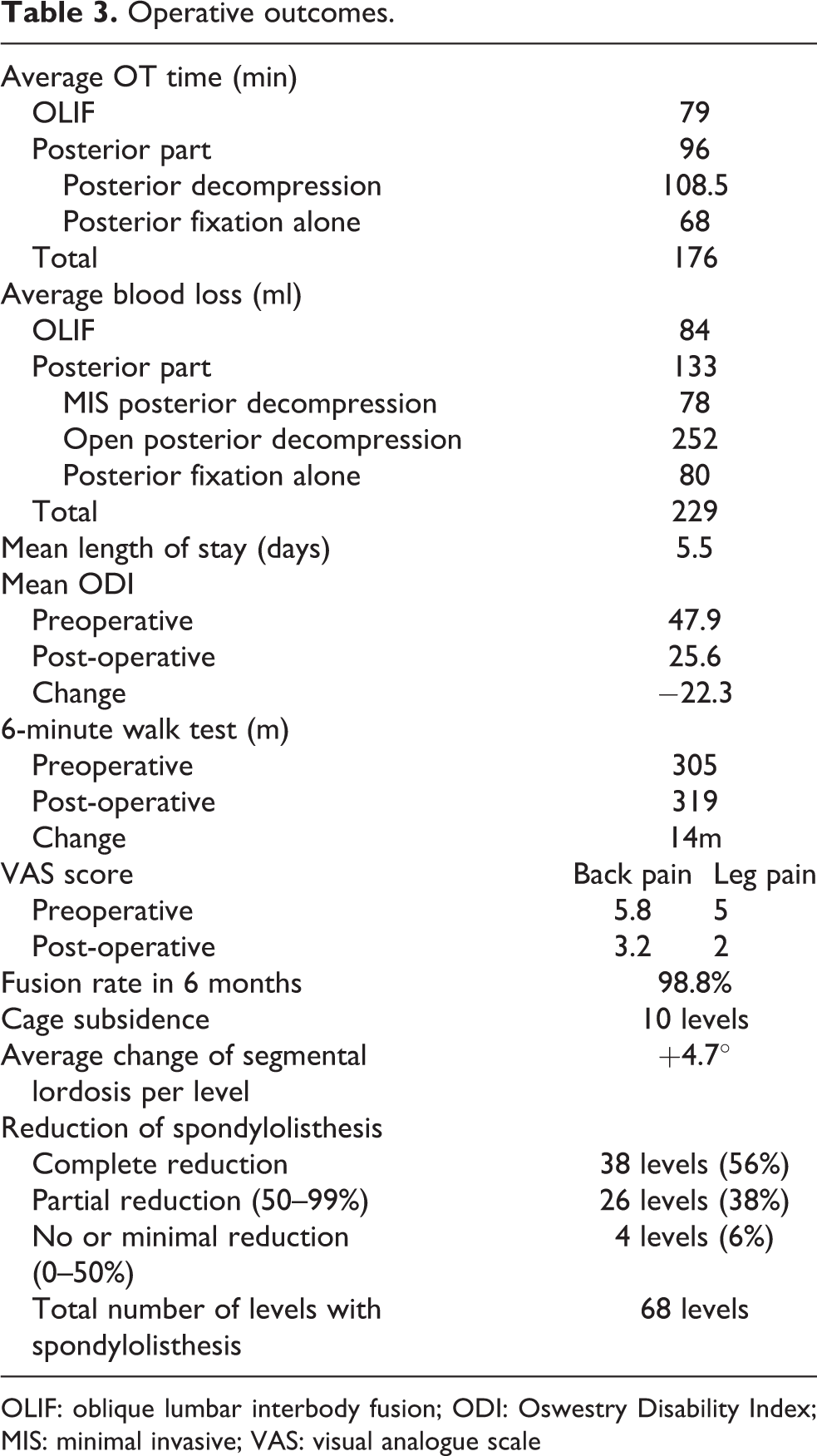
OLIF: oblique lumbar interbody fusion; ODI: Oswestry Disability Index; MIS: minimal invasive; VAS: visual analogue scale
Discussion
In the current study, we examined the efficacy and safety of OLIF surgery in treating degenerative lumbar spinal stenosis. Primary operative outcomes were satisfactory. High fusion rate of 98.8% was achieved. By fusing diseased level with specially designed interbody cages, alignment was improved with the increase of segmental lordosis, reduction of spondylolisthesis and correction of scoliosis. With alleviation of back pain and claudication symptoms as reflected by a reduction of average VAS score, mean ODI of our patients significantly improved from 47.9% to 25.6%.
Operative time, blood loss and hospital stay
Reduced blood loss and hospital stay were observed in our patients who underwent OLIF surgery. Their average blood loss for OLIF part was 84 ml, and their average blood loss for posterior fixation surgery was 133 ml. Over 90% of patients had less than 10 days of hospital stay, with a mean post-operative hospital stay of 5.5 days. Presence of early post-operative complications was one of the main confounding factors affecting the length of hospital stay. One case with 18 days of hospital stay was complicated with post-operative ileus and urinary tract infection. One case with psoas hematoma had 13 days of hospital stay.
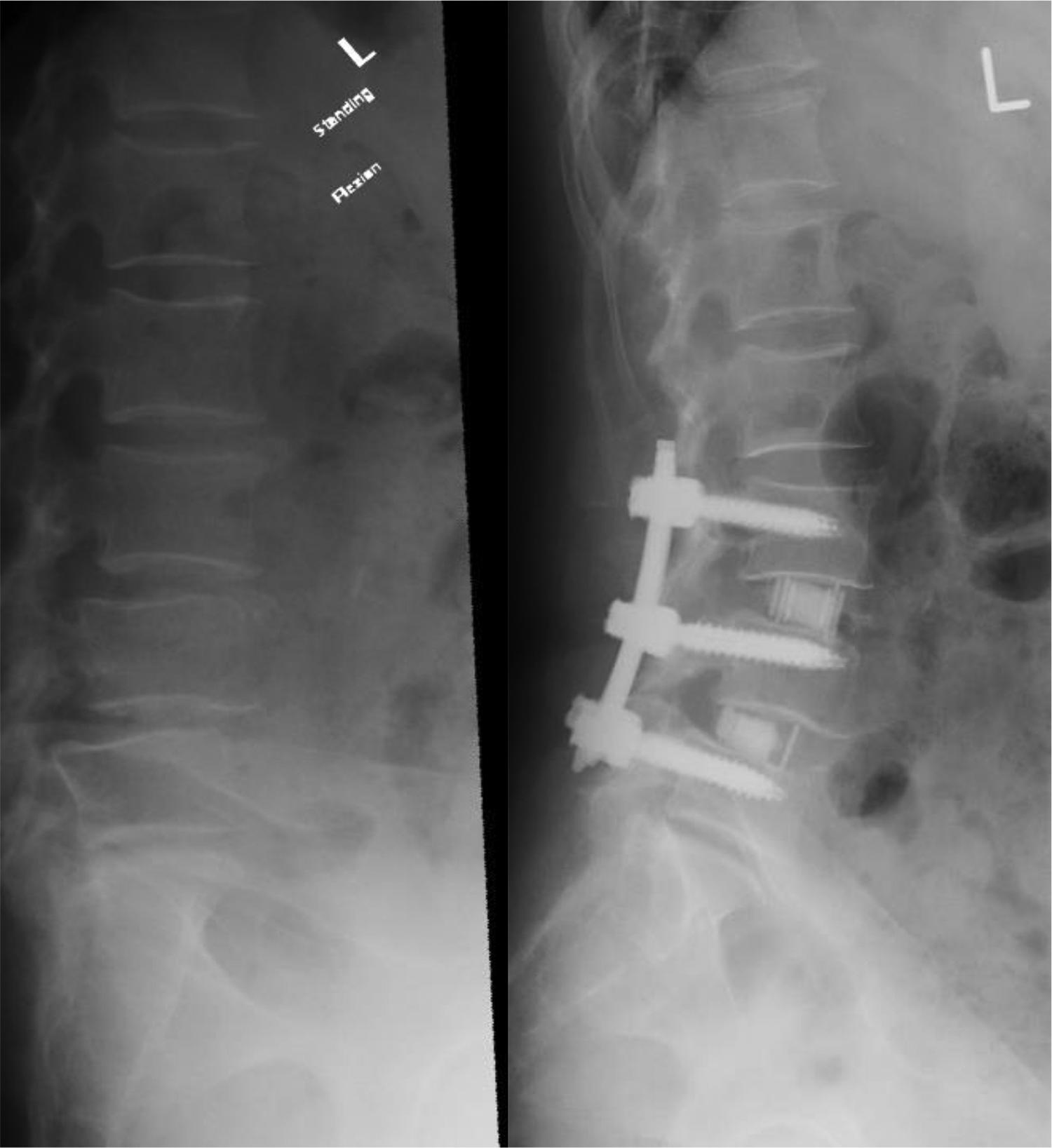
Further reduction of blood loss could be achieved with minimally invasive approach during posterior surgery, as surgical wounds were much smaller than the conventional approach (Figure 3). For patients receiving minimal invasive posterior decompression and percutaneous screw fixation, the average blood loss in the posterior part of the operation was 78 ml. For patients receiving open decompression and posterior fixation, their average blood loss was 252 ml. Both groups of patients had similar average operative time.
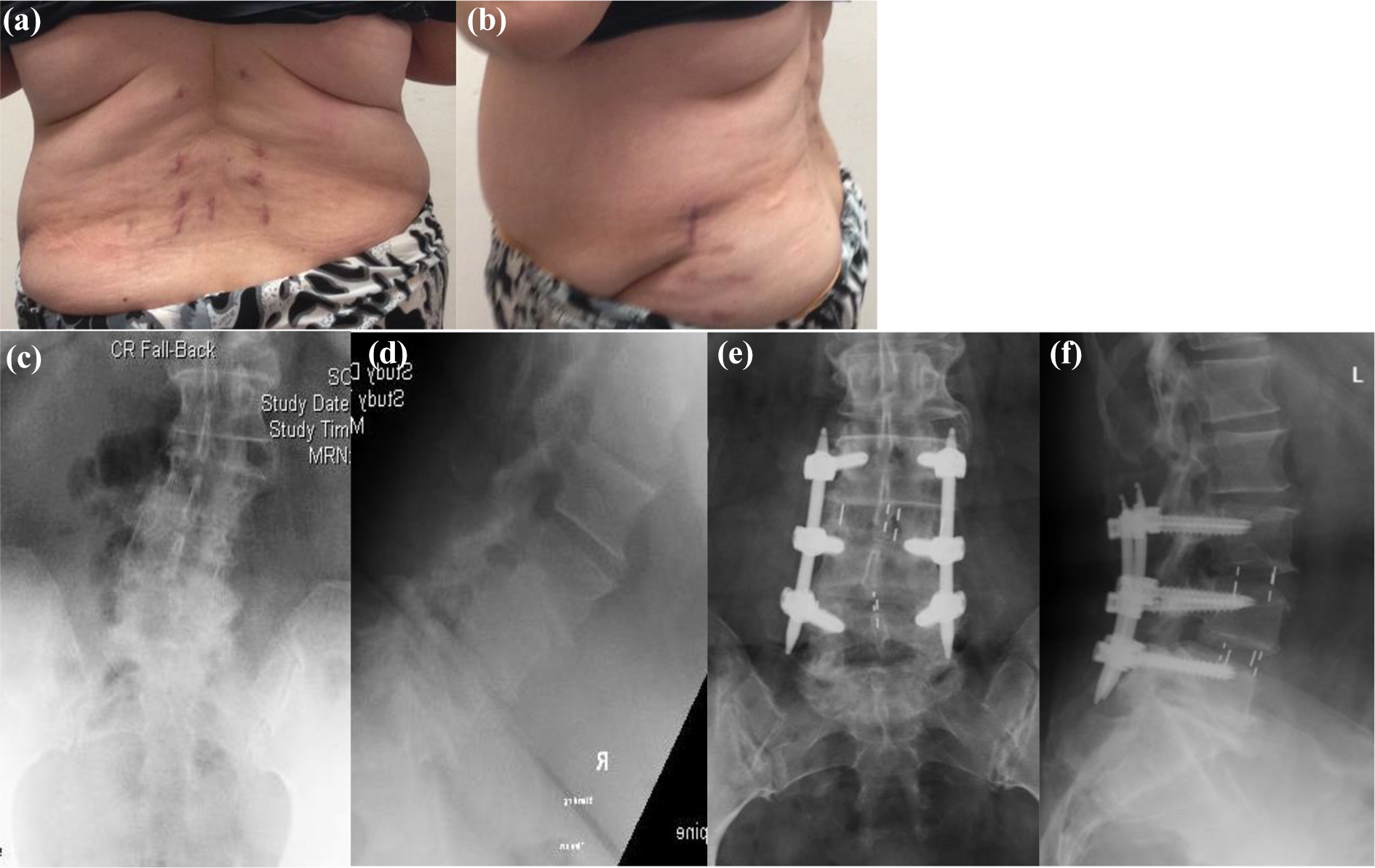
(a to f) OLIF L3–L5 with percutaneous screw achieving good correction of deformity with small wounds. OLIF: oblique lumbar interbody fusion.
The reported results of operative time, blood loss and hospital stay are variable in the literature. Li et al. 13 examined 16 studies in a meta-analysis: The mean blood loss of OLIF part was 109.9 ml, average operating time was 95.2 min, and mean post-operative hospital stay was 6.3 days. In our study, mean blood loss was 84 ml and average operating time was 79 min, while mean hospital stay was 5.5 days. Our results are comparable.
Cage subsidence
Delayed cage subsidence of 2 to 7 mm (mean 4.4 mm) was noted in 10 of the 83 levels of fusion performed, with incidence of 12% (Figure 4). Cage subsidence is indeed a common phenomenon found in all interbody fusion techniques utilizing cages. Currently, a few aetiologies are proposed to relate to the occurrence of subsidence. Patient factors increasing the risk of subsidence include high body mass index and low bone mineral density. 14 Studies have shown that oral bisphosphonate given post-operatively could decrease the incidence of cage subsidence. 15 Oxland et al. found that the removal of vertebral endplate reduces local strength and stiffness magnitudes in L3–L5 vertebral bodies, leading to an increased risk of implant subsidence. 16 Removing only the cartilaginous end plates and preserve bony end plate carefully could help to ensure a mechanically stable recipient site and reduce the potential for cage subsidence. 11

L3/4 solid fusion without subsidence. L4/5 solid fusion with subsidence.
Although cage subsidence caused loss of disc height and potentially reduced corrective power of deformity, most of these patients had improved ODI and VAS score at 6 months. Average ODI improved from 41.5% to 29.4%, while average VAS score for leg pain improved from 4.5 to 1.4. (Due to the small number of subjects, these results were not statistically significant.) We postulate the underlying reasons which include the majority of our patients received direct decompression and the subsidence we noticed are usually mild. However, we have to be very careful in indirect decompression group because subsidence might lead to loss of reduction and rebound of the stenosis. Choi and Sung 17 suggest that subsidence is the incorporation process of the cage to both end plates. As end plate tends to be curved or concave, often only the periphery of the cage is initially in contact with the end plates. When loaded, a cage subsides to achieve better contact with the bone, leading to the reduction of disc space height in spite of solid fusion, which does not preclude a good clinical outcome.
Adverse events and Complications
Adverse events were seen in 10 patients. The complications observed include transient thigh pain or numbness (seven cases), retroperitoneal hematoma (two cases) and post-operative ileus (one case). One case needed reoperation (one case). None of the patients experienced infection, symptomatic pseudoarthrosis, hardware failure, vascular injury, nerve injury, ureteral injury, bowel injury, incisional hernia or death.
The most common minor complication observed in our study is transient thigh pain or numbness, which is found in 11.7% of our patients. All the cases have symptoms resolved spontaneously within 6 weeks upon conservative management. Transient thigh pain or numbness is believed to result from retraction of psoas, which contains the nerves of lumbosacral plexus posteriorly and genito-femoral nerve anteriorly. 18 To compare with XLIF, which is a trans-psoas approach potentially causing plexopathy up to 13.3%, 19 OLIF is safer and less likely to cause neurological morbidity.
There were two cases with retroperitoneal hematoma. One of the two patients was taking warfarin for aortic valve regurgitation. Warfarin was withheld 7 days before the operation and resumed at post-operative day 2 with bridging low-molecular-weight heparin. She presented with sudden deterioration of left L2 and L3 power at 2 weeks post-operatively. Urgent MRI reviewed a large left psoas hematoma. Surgical drainage was performed with resolution of hematoma and gradual improvement of plexopathy. In another case, left psoas hematoma found at post-operative day 5 was confirmed with CT scan. Reassessment CT scan showed hematoma completely subsided after 1 month upon outpatient conservative management. There was no deterioration of neurology all along (Figure 5).
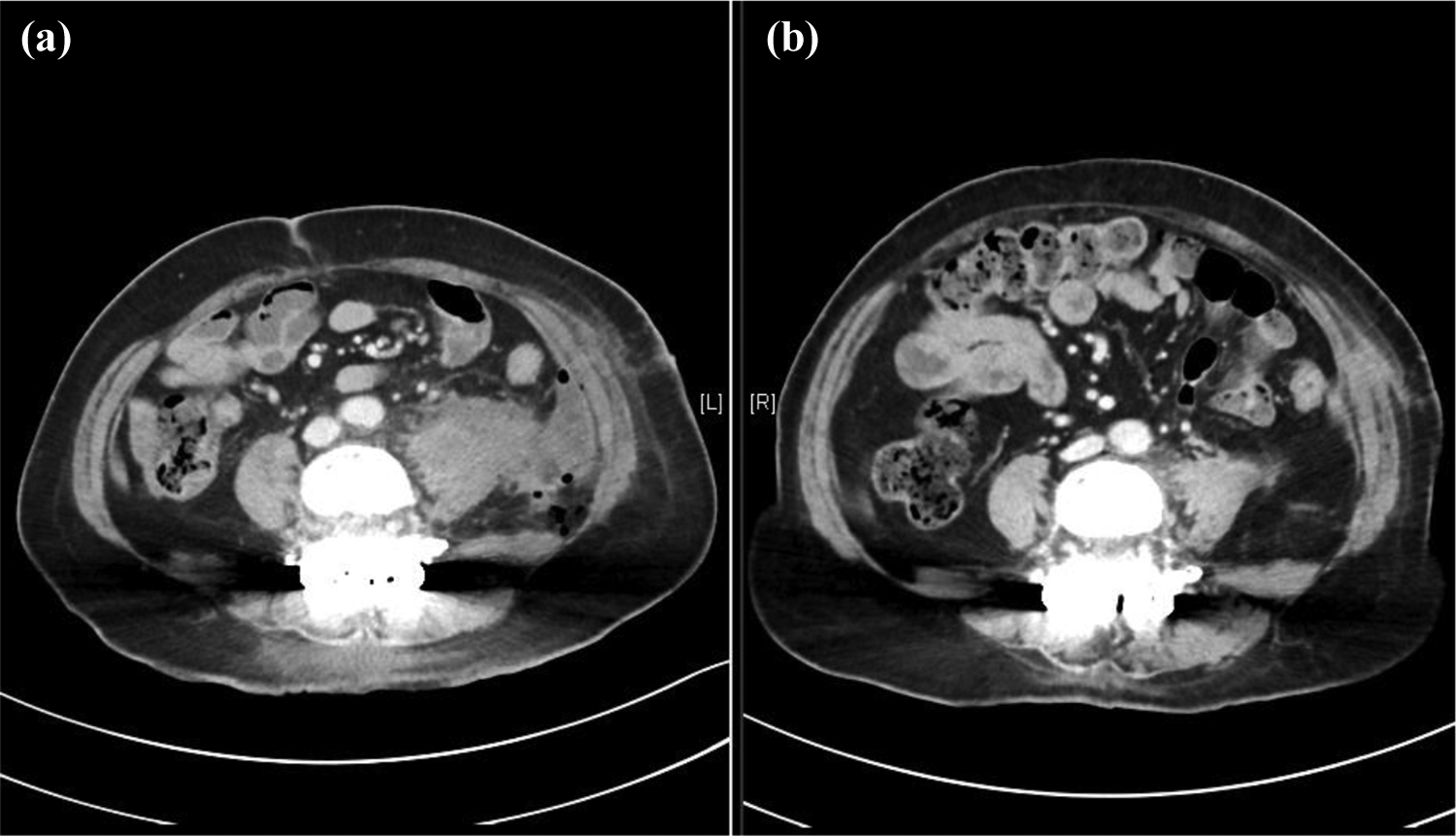
Retroperitoneal hematoma treated with conservative management. (a) Contrast CT at post-op day 5. (b) Contrast CT at post-operative 1 month. CT: computed tomography.
There was one case of BMP osteolysis (Figure 6) OLIF was performed at L4/5 level using 12° polyetheretherketone (PEEK) cage inserted with BMP (1.4 cm3) and demineralized bone matrix. X-Ray taken at post-operative 6 weeks revealed cut out of upper L4 screw with L4/5 slip and osteolysis of L4 lower endplate. The patient was relatively asymptomatic and conservative management was given. Plain CT scan at post-operative 2 months showed fusion with 4 mm subsidence. Follow-up CT scan at 8 months showed no further displacement. It is proposed that damage of end plate during end plate preparation with blunt shaver, as well as a relatively high dose of BMP (1.4 cm3) given were the cause of this rare complication. In subsequent surgeries, Cobbs was used to peel off cartilaginous end plates carefully. Half of the recommended dosage of BMP (0.7 cm3) was used. No more BMP osteolysis was reported.
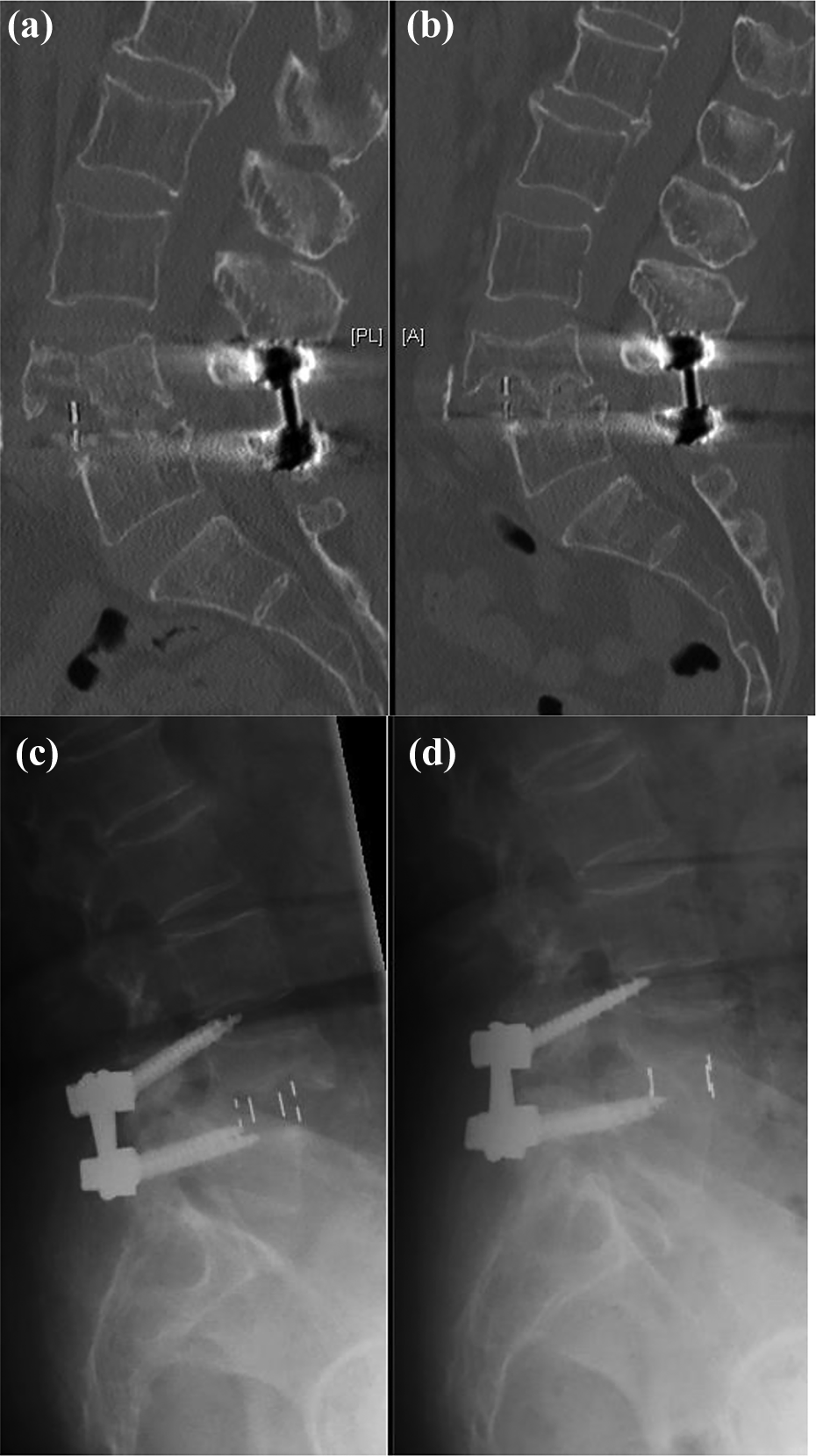
This patient had L4/5 OLIF performed. (a) X-Ray and (c) CT on the left showed BMP osteolysis at post-operative 6 weeks causing cut out of L4 screws. Treated conservatively. Repeated (b) X-ray and (d) CT showed solid fusion after 8 months. CT: computed tomography.
There was one case of post-operative ileus, resulting in prolonged hospitalization. It is believed that ileus was caused by excessive anterior retraction on the peritoneum, and the complication rate was up to 2–4% in the literature. 20 There were no cases with peritoneum laceration in our cohort of patients.
In the literature, OLIF is reported to associate with vascular, ureter and nerve injury. 20 The most commonly injured vessel is lumbar segmental arteries, followed by iliac vein laceration. In our cohort of patients, there were no cases with major vessel, ureter or nerve injury reported. Despite the seemingly proximity of the OLIF approach with these structures, injury can be well prevented with correct surgical technique and careful dissection. Also, the anatomical parameters of the OLIF operative window can be measured in preoperative magnetic resonance imaging (MRI). The oblique corridor is defined as the smallest distance between the left psoas major muscle and aorta at the left side, and between the right psoas major muscle and inferior vena cava or common iliac artery at the right side. Liu et al. recommended opting for a different lumbar fusion technique when this distance is less than 1 cm. 21 Li et al. suggested a left-side approach is more viable as the oblique corridor is larger in both sexes. 22
Indirect decompression achieved by OLIF procedure
OLIF allows placement of larger interbody cages as compared to posterior approaches, which leads to greater restoration of disc height and thus indirectly decompresses the spinal canal. Various studies have shown indirect decompression have satisfactory clinical and radiological outcomes. 23 In our study, indirect decompression is only adopted in selected patients, as we believe that there are a few prerequisites before considering indirect decompression sufficient. These include patients with symptoms that are variable with position and activity, signifying a dynamic component affecting symptoms presentation. We also preferred patients with magnetic resonance imaging showing spondylolisthesis causing predominant lateral canal stenosis, with relatively less central canal stenosis, minimal facet hypertrophy or prolapsed intervertebral disc. Also, selected patients need to have good bone quality. Osteoporotic bone is a relative contraindication as there is a higher risk of loss of reduction. Last but not the least, we are able to achieve good reduction of slip and relief of lateral recess stenosis from OLIF.
Comparison with other approaches
In the literature, some trials have compared OLIF with other interbody fusion approaches. No one single approach has been proved to be superior to the others significantly in terms of outcome. 24 However, we believe that OLIF has its specific advantages compared with other approaches. Compared with PLIF or TLIF, OLIF has less back muscle injury and allows the use of a larger cage. Compared with XLIF, OLIF has less psoas muscle and spinal nerve injury. It does not require the use of real-time EMG monitoring. Compared with traditional anterior approaches, minimally invasive OLIF carries about the same type and rate of complications, with less post-operative pain and wound-related co-morbidity such as abdominal wall herniation. 25 More cases should be examined with longer follow-up to further evaluate the long-term outcome of OLIF in our population.
Conclusion
In summary, OLIF surgery with specially designed cages enables placement of a larger interbody graft into the disc space for anterior column support and segmental sagittal alignment, while minimizing the nerve, muscle and bone obstacles associated with traditional direct lateral approaches.
It is an effective procedure to treat lumbar spinal stenosis and spondylolisthesis with excellent fusion rate and good functional outcome. Complications specific to this procedure are not uncommon, but the majority are minor and self-recovery. Proper training is required to minimize potential surgical risks.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.