
Abstract
Background/purpose:
The combination of ipsilateral floating shoulder and flail chest is a unique injury pattern that has not been previously described in the literature. We termed the injury pattern floating flail chest (FFC). The purpose of this study was to evaluate the effect of operative treatment of the shoulder girdle component to overall hospital length of stay (LOS).
Methods:
Forty-one patients were enrolled between two level I trauma centers identifying with a combination ipsilateral floating shoulder and flail chest injury, 23 treated with operative stabilization and 18 treated non-operatively. This retrospective cohort study evaluated the overall LOS and intensive care unit (ICU) days.
Results:
The operative group had decreased overall LOS (10.1 vs. 19.8 days, p = 0.02) and decreased ICU days (3.4 vs. 10.3, p = 0.04).
Conclusion:
This study describes a unique injury pattern that combines the floating shoulder and flail chest, FFC. Our study suggests that operative treatment of the shoulder girdle may decrease both overall LOS and ICU days in patients with FFC.
Introduction
The “floating shoulder,” is a rare injury consisting of ipsilateral fractures of the clavicle and glenoid neck; first described by Ganz and Noesberger in 1975. 1 Traditionally defined as a bony injury, 2 Goss expanded the understanding of this injury to include the ligamentous injuries that disrupt the superior shoulder suspensory complex. 3 Floating shoulder typically requires a high-energy mechanism such as motor vehicle accident 4 or fall from height. 5 A variety of treatment protocols have been described in the literature with good results following conservative management, 6,7 operative management of the clavicle alone, 5,8,9 or operative management of both the clavicle and the scapula. 10 While the shoulder girdle is the primary pathology, the zone of injury frequently involves the chest wall, with rib fractures occurring in up to 73% of cases of floating shoulder 11 (Figure 1).

Floating shoulder: (a) injury radiograph demonstrating a bony injury involving midshaft clavicle fracture and complex scapula fracture involving neck, body, and glenoid. Note the medialization of the humeral head on the injury radiograph and (b) postoperative radiograph with restoration of anatomic alignment after open reduction and internal fixation of clavicle and scapula.
The most severe type of chest wall injury has been described as a flail chest. The definition of flail chest has been inconsistent in the literature. However, it was recently defined as fractures of three or more consecutive ribs, with each rib fractured in two or more places. 2,9 This leads to a free segment of the chest wall recognized clinically by the resulting paradoxical motion with respiration. The incidence of flail chest has been reported to be as high as 6% in patients suffering from blunt chest trauma. 12,13 The paradoxical motion leads to respiratory inefficiency and difficulty in clearing secretions. 14 In-hospital mortality of this injury has been reported to approach 33%. 15,16 Treatment protocols continue to favor non-operative management in the vast majority of institutions 14 as well as by the current Eastern Association for the Surgery of Trauma (EAST) guidelines. 17,18 However, two randomized studies 18,19 and a matched cohort study 20 have shown improved outcomes with surgical intervention in carefully selected patient populations.
The combination of floating shoulder and flail chest injuries have not been previously described in the literature. We define floating flail chest (FFC) as an injury resulting in segmental fractures of three consecutive ribs in conjunction with an ipsilateral clavicle and scapula fracture. The management of both floating shoulder and flail chest individually remains controversial, with significant mortality and morbidity associated with each injury pattern. The risk of mortality in the management of flail chest has been linked to the acute phase of the injury, particularly limiting the duration of mechanical ventilation and intensive care unit (ICU) length of stay (LOS). 17,21,22 The literature does not currently provide any guidance for the management of this combined injury pattern. No recommendations exist on the strategy for stabilization of the floating shoulder or the effect this may have on the hospital course for these patients. Our study describes a combined injury pattern, which we define as FFC, and presents our initial series of patients evaluating the results of surgical stabilization of the shoulder girdle compared to non-operative treatment. We hypothesized that rigid surgical stabilization of the shoulder girdle would improve the hospital course in the operative cohort compared to the non-operative group. The purpose of this study was to evaluate the effect of operative treatment of the shoulder girdle component of the FFC injury pattern on overall hospital LOS. Our primary outcome was total LOS, with the specific ICU LOS acting as a secondary variable. Finally, we performed a preliminary cost-analysis to explore the cost-of-care measures within either treatment arm.
Materials and methods
Following Institutional Review Board approval of our study design involving human participants, patient records from two level I trauma centers were retrospectively reviewed. Inclusion criteria were defined as skeletal maturity, osseous floating shoulder defined as an ipsilateral displaced scapula (14-A3 and 14-C3) and clavicle fractures (15-B), ipsilateral flail chest defined as three consecutive segmental rib fractures, and survival to discharge. Exclusion criteria were moderate or severe traumatic brain injury (Glasgow Coma Scale <13), spinal cord injury with motor deficits, and low-energy mechanism in a geriatric patient population (age > 80). Between August 2007 and November 2015, a total of 88 consecutive patients were identified with displaced scapula and clavicle fractures based on radiographs. Flail chest was then confirmed by reviewing chest computed tomography studies, which the literature has reported as the most sensitive imaging modality to identify flail chest. 23 The decision to intubate patients upon arrival to the trauma bay was made by the attending trauma surgeon as well as the ventilation management in the surgical ICU. Our protocol for the management of flail chest follows the EAST.
In total, 41 patients met the inclusion criteria with 23 patients managed with operative stabilization of the shoulder girdle and 18 patients treated non-operatively. The decision to preform operative stabilization was left to the discretion of four fellowship-trained orthopedic trauma surgeons. Patients of both treatment cohorts were seen by physical therapy and provided the same motion protocol, unrestricted active and passive motion with weight bearing restricted to 5 lbs. Cohorts were evaluated regarding age, sex, and Injury Severity Score (ISS).
Cost analysis was preformed to compare the cost of care for these two cohorts. Cost estimates utilized a previously published method for evaluating clavicle fracture fixation cost-effectiveness. 24 The total cost per patient was extrapolated from each patient’s number of ventilator days, ICU days, total hospital LOS, operative status, tracheostomy, and home oxygen. All patients were assessed with a hospital diagnosis-related group (DRG) 443, while operative patients were charged an additional cost for anesthesia care and a cost of operative fixation of the fracture as previously reported. 24 Operative charges were allocated by current procedural terminology (CPT) codes 23515 and 23585. DRG codes identify patient charges for those that utilized federal health-care mediums, specifically either Medicare or Medicaid. CPT codes are utilized to derive costs for operative procedures, and specific CPT codes correlate with a specific amount of relative value units (RVUs). These RVUs are then translated into fiscal sums based on the supervising systems’ costing formula. 24
Non-operative patients were charged the same DRG, presuming that it was an admission trigger. Cost of ICU was estimated at US$10794.00 if ventilated and US$6667 if not ventilated for the first day, US$4796 if ventilated and US$3968 if not ventilated for the second day, and the remaining days it was estimated at US$3968 if ventilated and US$3184 if not ventilated, as previously reported. 25 Each additional day in hospital (floor) was estimated to be US$1488. 26 Non-operative patients were assessed an estimated US$4558.71 DRG fee based on hospital admission and US$185.32 for management of fracture of the shoulder girdle (CPT 23500 and 23570), as previously reported. 24 Operative patients were assessed the US$4558.71 DRG fee, plus US$203.70 for anesthesia, US$1012.63 for scapula fixation, or US$816.17 for clavicle fixation. Costs of tracheostomy and home oxygen supplies were estimated based on Medicare reimbursement for CPT 31600 (US$605.40) and standard initial supplies, respectively. For the sake of the cost analysis, fixation of the clavicle and scapula were assumed to be concurrent, discounting the cost of clavicle fixation by 50%. However, it should be noted that cost data is only relevant to the patients’ initial inpatient stay, not the full episode of care.
Primary outcome was LOS, defined as the total time in hospital with secondary analysis examining the number of ICU days, ventilator days, tracheostomy, and home oxygen requirements. All patients were followed to hospital discharge. Statistical analysis was done utilizing nonparametric Mann–Whitney U test for continuous variables and Fischer’s exact test for descriptive variables. All statistical analysis was conducted in SAS 9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Our study consisted of 41 patients, with 23 patients undergoing surgical stabilization and 18 patients treated non-operatively (Table 1). The mean age was 48.8 (range 33–74), with mean ages being 47.5 and 50.4 years in the operative and non-operative groups, respectively. The predominant mechanism of injury was motorcycle injury in 25 patients followed by fall from height in 8 patients, motor vehicle collision in 3 patients, and 5 other unique high-energy mechanisms in the remaining patients. Of the operative cohort, nine (39.1%) patients received some level of open reduction and internal fixation of at least one of the resulting rib fractures. The mean ISS of the operative group was 23.8, compared to 28.4 in the non-operative group (p = 0.08).
Study population characteristics from August 2007 to November 2015, stratified by the treatment strategy (N=41).a
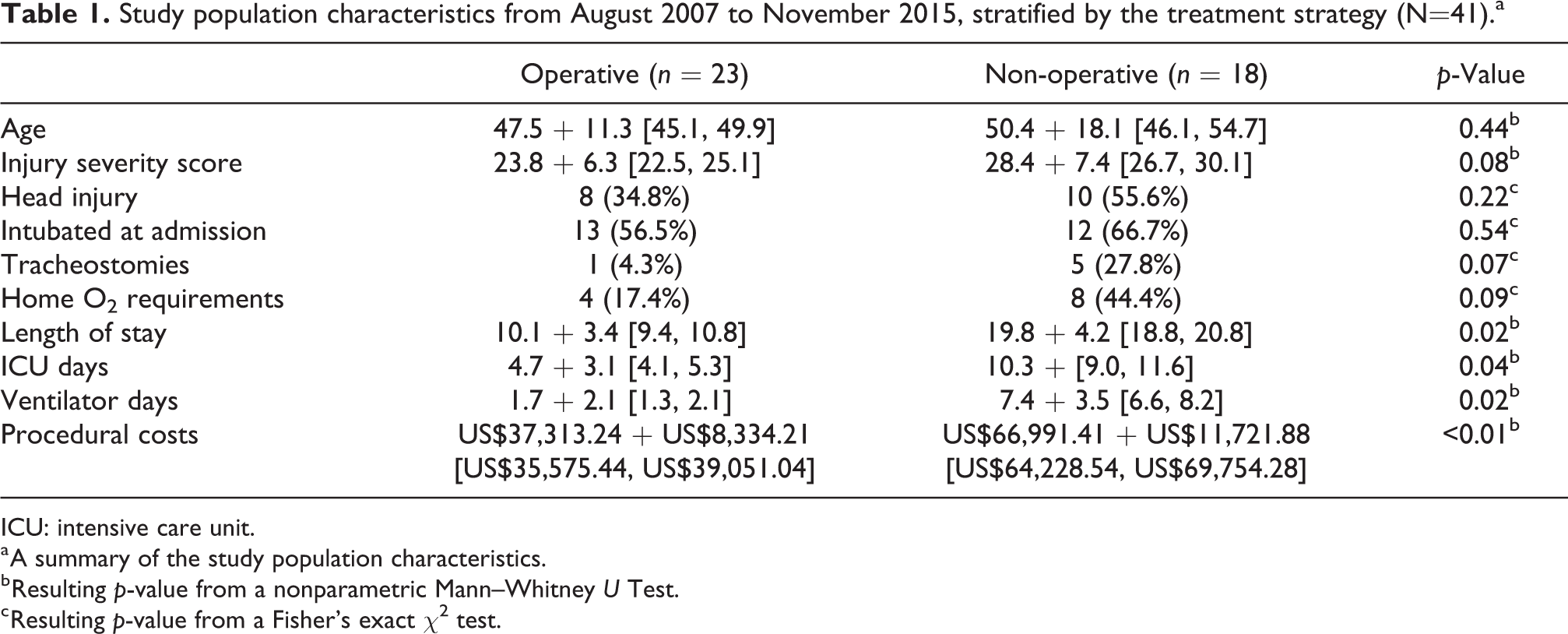
ICU: intensive care unit.
a A summary of the study population characteristics.
b Resulting p-value from a nonparametric Mann–Whitney U Test.
c Resulting p-value from a Fisher’s exact χ2 test.
Concurrent open reduction and internal fixation of both the scapula and the clavicle were done for 10 patients, with independent fixation of the scapula or clavicle in 7 and 6 patients, respectively. Classifiers of head injuries (34.8% vs. 55.6%; p = 0.22), intubation at admission (56.5% vs. 66.7%; p = 0.54), tracheostomies (4.3% vs. 27.8%; p = 0.07), and home oxygen requirement (17.4% vs. 44.4%; p = 0.09) were all comparable between the operative and non-operative groups.
The operative group had shorter average LOS (10.1 vs. 19.8 days; p = 0.02), LOS within the ICU (10.3 days vs. 4.7 days; p = 0.04), and days remaining on a ventilator (1.7 days vs. 7.4 day; p = 0.02). There were no cases of acute operative wound infection. Provided with these details, the operative cohort consisted of a mean cost of US$37,313.24 with non-operative treatment averaging US$66,991.41 (p < 0.01). Due to the limited sample sizes, the above statistics should be interpreted with caution.
Discussion
Our study is the first to describe a complex injury pattern including ipsilateral floating shoulder and flail chest defined as an FFC. The cohort was predominately middle-aged men with high-energy injury mechanisms, most often motorcycle collisions. The demographic and mechanism characteristics of this cohort are consistent with a recent review of the National Trauma Bank for patients with flail chest 14 ; however, a slightly older population than previously reported for cohorts of patients with floating shoulder. 5,9 In our study of 88 consecutive patients with floating shoulder, the incidence of flail chest was 46.6%. Our results show a significant decrease in the overall length of hospital stay in favor of the cohort that received operative stabilization of the floating shoulder component. Secondary analyses presented with positive results in favor of operative stabilization of the shoulder girdle, demonstrating decreased time in the ICU and decreased time in the ventilator in the postoperative period. We speculate that the benefit from operative management is from the restoration of the scapula-clavicular arch that improves the biomechanics of the articulation of the shoulder girdle with the thoracic cage, unloading the injured chest wall, reducing pain, and facilitating earlier participation in physical therapy. Additionally, while operative management has an associated upfront cost, the surgical management cohort identified with a lower mean inpatient cost-of-care than their non-operative counterparts (Figures 2 and 3).
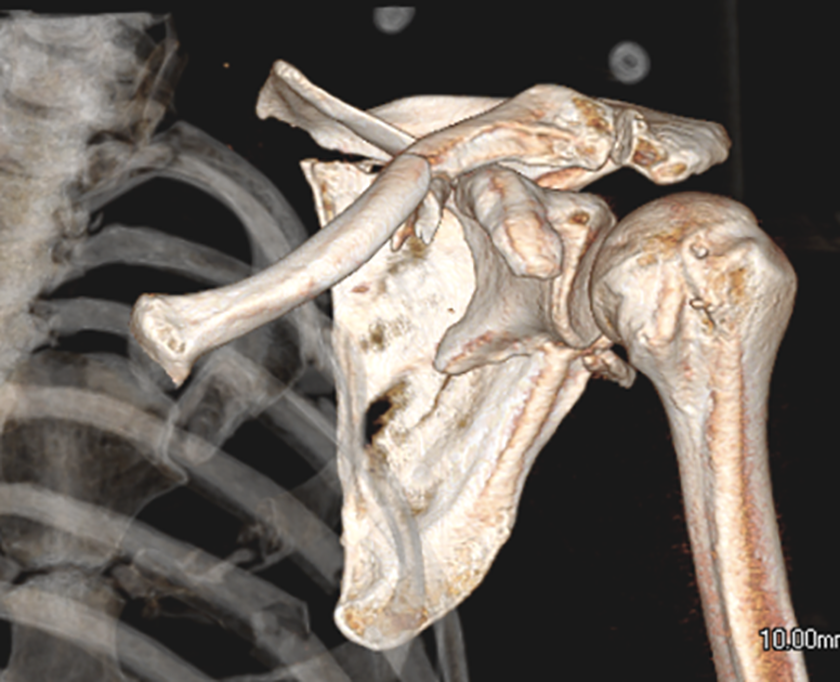
Floating shoulder. 3D-CT reconstruction demonstrating the floating shoulder portion of the injury. Note the loss of the normal humeral head offset relative to the thoracic cage, which was noted routinely in this patient population. The loss of the scapula-clavicular arch was a consistent finding in this injury pattern. 3D: three dimensional; CT: computed tomography.
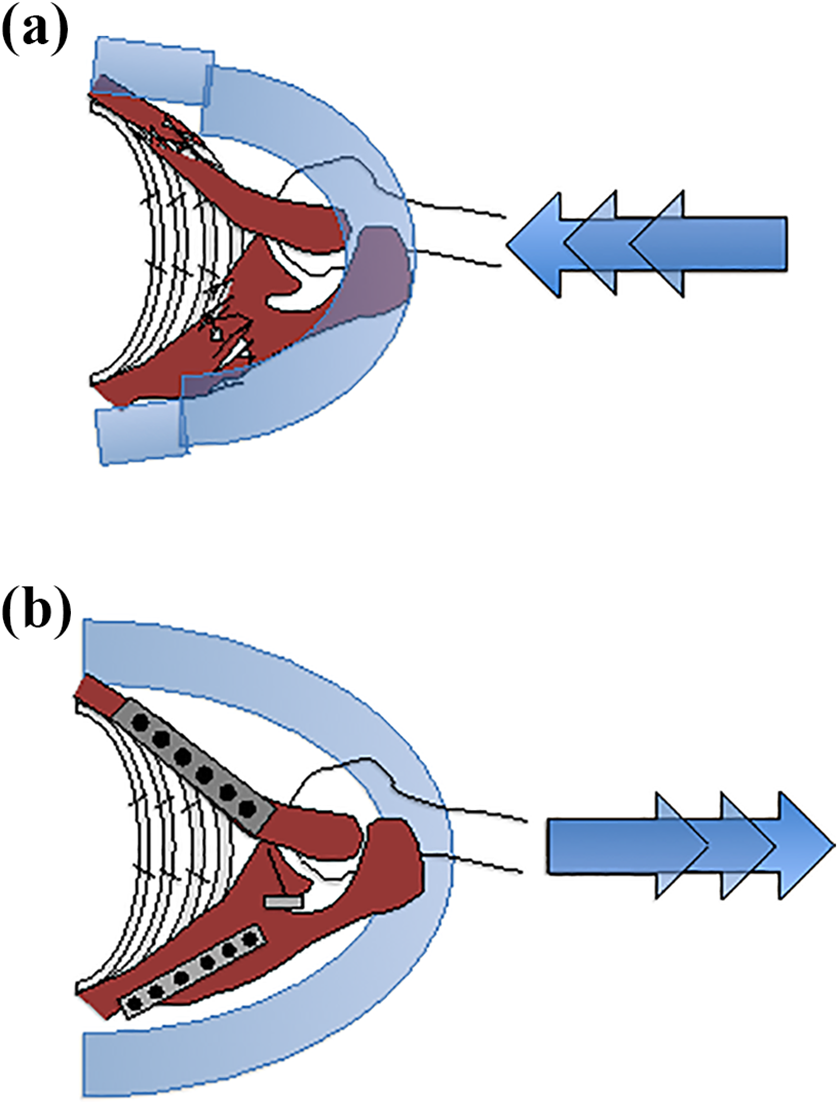
(a) Restoration of the scapula-clavicular arch collapse results in compression of the flail chest segment. (b) Restoration of the scapula-clavicular arch unloads of the flail chest segment and may lead to improved respiratory function and pain control.
Previous treatment protocols have historically been controversial for both flail chest 14,17 –20 and floating shoulder. 2,6 –10 Concerns regarding operative stabilization have been related to perioperative infection, cost, and questionable benefits. Flail chest places patients at a significant risk of respiratory complications in the acute phase of the injury by compromising respiratory function via altered chest wall biomechanics and decreased ability to clear secretions because of pain control. Patients with flail chest often require mechanical ventilation. 14 Pneumonia and sepsis are the two leading causes of death in patients with flail chest injuries. 27 Our surgical cohort averaged 4.7 ICU days versus 10.3 ICU days in the conservatively managed group. The National Trauma Bank data reflects similar results for patients with isolated flail chest, who were managed conservatively, averaging 11.7 ICU days. 14 Decreased time in the intensive care has been shown in multiple studies to improve outcomes, decrease infection risk, and correlate with decreased mortality. 14,28 –31
In addition to other clinical benefits, operative fixation was found to lead to decreased overall hospital costs. The average cost of an ICU day is estimated at US$10,794.00 for the first day and then plateaus at US$3,968/day by the third day, depending on the need for mechanical ventilation, 25 and surgical floor costs are estimated at US$1,488/day. 26 Therefore, the decreased length of inpatient hospital stay, decreased ICU days, and decreased number of ventilator days from operative treatment may potentially offset the additional costs incurred during surgery for the operative group (US$37,313.24 vs. US$66,991.41). The mean inpatient cost of care estimates differed by US$29,678.17, in favor of the operative cohort. However, it should be noted that this does not reflect the large costs associated with rare complication events, such as: deep vein thrombosis (DVT), pulmonary embolism, or pneumonia; which our study does not have an adequate sample size to evaluate. A large database study recently reported that ventilator-associated pneumonia developed in 9.3% of ventilated patients at a mean of 3.3 days from intubation with an overall cost of more than US$40,000/patient. 29 Furthermore, this preliminary cost-analysis only evaluates costs attributed to the patients’ primary inpatient care episode. Further cost data regarding the full patient episode-of-care would have to be rigorously analyzed before further conclusions can be drawn.
Our study has a number of strengths and weaknesses that warrant discussion. The strengths of our study include the description of a complex and previously unreported injury pattern. Additionally, our study reports a robust experience with a rare injury pattern including both operative and non-operative management. We used a retrospective cohort study design providing an increased level of evidence and more rigorous scientific evaluation of our hypotheses compared to a traditional case series. Weaknesses of our study include a small sample size, which may have contributed to multiple parameters lacking statistical significance. Despite the rigorous use of inclusion and exclusion criteria, our sample represents a heterogeneous patient population, in-part because the extent of pulmonary and other associated injuries was not quantified. We did not examine clinical outcomes following hospital discharge to assess the long-term benefits of operative treatment; however, this was outside of the scope of the current study. Previous authors have shown the benefits of operative fixation of the floating shoulder in isolation, 5,9,10,14,28 including a recent randomized, prospective trial. 8 Another weakness of our study was that the treating surgeon was allowed the discretion to choose operative or non-operative intervention as well as the independence to select which components of the floating shoulder to stabilize. The average ISS was not statistically significant between groups; however, there was a trend suggesting the potential for selection bias of the treating surgeon.
Conclusion
In conclusion, our study reports a rare combination of floating shoulder and flail chest, which we describe as FFC. Operative treatment of this injury pattern suggests stabilization of the floating shoulder may improve outcomes in this patient population through decreased hospital LOS, decreased ICU, and decreased ventilator days. We hypothesize that the operative stabilization of the floating shoulder may unload the flail chest injury through the restoration of the scapula-clavicular arch. Therefore, we recommend that the presence of flail chest be an indication to operatively manage floating shoulder. However, considerations must be made for the small study sample and its limitations to the interpretability of these study results. We do plan to continue studying this injury by examining the long-term clinical outcomes of operative stabilization as well as evaluating the biomechanical interaction of the scapula-clavicular arch and the thoracic cage. Lastly, we plan to expand on the cost-analysis introduced in this study, to evaluate costs attributed within the full patient episode of care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.