
Abstract
A case of post-traumatic proximal peroneal artery pseudoaneurysm following a proximal tibial shaft fracture, complicated by acute compartment syndrome, fixed using an external fixator, in a 22-year-old female is presented. She was investigated for sudden-onset bleeding from the external fixator pin site, 6 weeks after the initial injury, was anaemic and diagnosed with a pseudoaneurysm at lower limb angiography. Contrast leak from the site of pseudoaneurysm was noted and open surgery with ligation of the pseudoaneurysm was performed. This rare complication of a proximal tibial shaft fracture has to be considered in patients presenting with acute bleeding from the surgical site or from pin sites after a significant lag period and requires a high index of suspicion.
Introduction
Post-traumatic pseudoaneurysms are localized haematoma with persistent communication with the native artery via a narrow neck 1 formed following direct arterial injury resulting in disruption of arterial wall continuity. Symptoms include leg swelling, bruising, pain, neurological signs due to nerve compression (commoner in femoral and popliteal aneurysms) and bleeding due to rupture, and their onset depends on the size, rate of expansion and its proximity to a nerve. Peripheral traumatic pseudoaneurysms rarely present around the foot and ankle. A few case reports on peroneal artery traumatic pseudoaneurysms are reported but a majority are associated with ankle ligament injury. No case reports of traumatic proximal peroneal pseudoaneurysms as a complication arising due to external fixator screw fixation or from proximal tibial fractures were found in the literature. 1 Treatment options described include both surgical (open repair and ligation) and interventional radiological interventions (ultrasound-guided thrombin injection and percutaneous endovascular repair with stents).
Case description
A 22-year-old previously healthy female patient, a passenger of a motor bicycle, was admitted to a tertiary care hospital, following a road traffic accident. She sustained an isolated compound comminuted proximal tibial fracture of the right lower extremity with skin loss over the medial aspect of the proximal tibia, followed by acute compartment syndrome of the right leg. The dorsalis paedis and posterior tibial pulses were palpable and the foot was sensate. The knee joint was stable with clinically intact cruciate ligaments. A lateral single incision fasciotomy with the release of all four compartments along with the application of an external fixator was performed (Figure 1). There was no evidence of bleeding or other hard signs suggestive of a vascular injury at surgery.
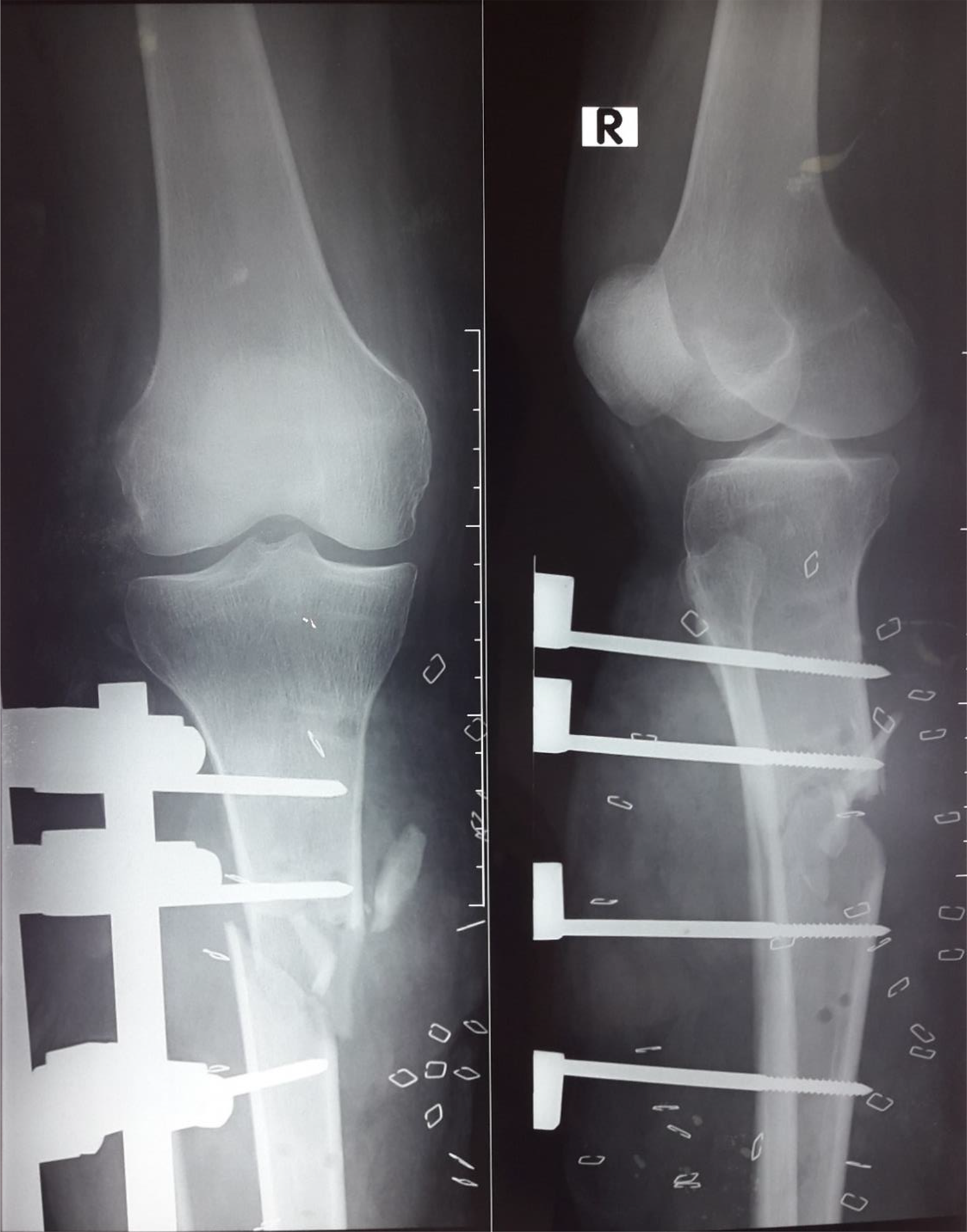
Antero-posterior and lateral radiographs of the knee joint and proximal tibia.
A medial gastrocnemius flap cover was performed to cover the fracture site, and a vacuum-assisted closure device applied, followed by superficial partial thickness skin grafting of the site later. She was discharged from the hospital 30 days after admission, with evidence of satisfactory skin graft acceptance and radiographic evidence of callus formation.
She re-presented, 45 days after the initial injury, with complaints of sudden onset of bleeding from the external fixator distal pin site for 3 days and had a haemoglobin level of 7.2 g/dL (haemoglobin level prior to hospital discharge was 10.5 g/dL). Subsequent ultrasound scan was normal; however, angiography revealed a pseudoaneurysm of the peroneal artery, adjacent to the tibioperoneal trunk with contrast leak suggestive of rupture of the pseudoaneurysm (Figure 2). Endovascular intervention was deemed not suitable, and surgical exploration with proximal ligation of the pseudoaneursym was undertaken. Post-operative recovery was uneventful with palpable dorsalis paedis and posterior tibial pulses, and a sensate foot.
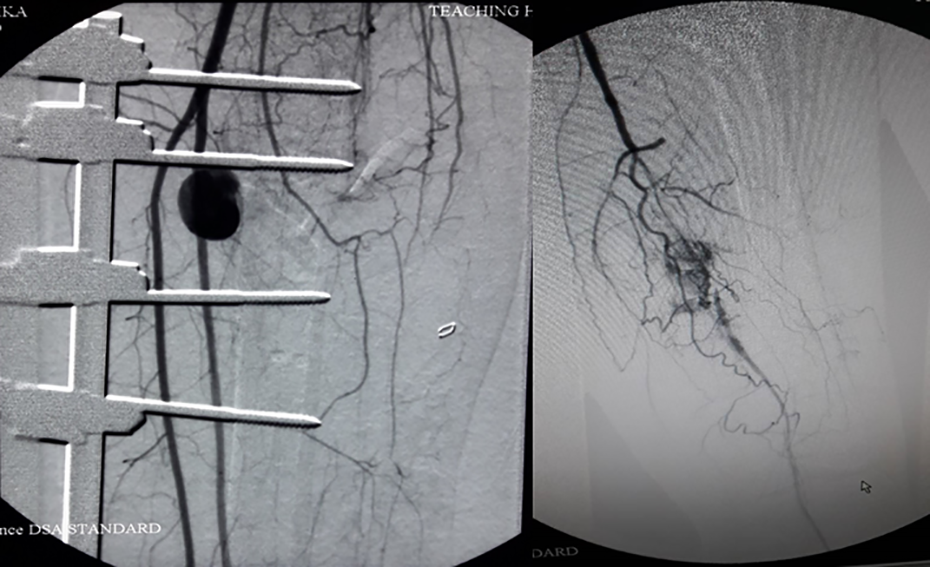
Lower limb angiography with the pseudoaneurysm of the peroneal artery, adjacent to the tibioperoneal trunk (left) with contrast leak apparent (right).
Discussion
Case reports on pseudoaneurysms of the peroneal artery, which are rare in the literature, are described in subjects between 17 years and 71 years, with a majority being less than 30 years 1 with ligament sprains, bimalleolar fractures and distal tibia/fibular fractures being the commonest associated injury.
Arteriography was the most commonly performed investigation (52%), followed by computed tomography angiography (CTA; 22%) and Doppler ultrasonography (11%). 2 The anatomical origin is confirmed by angiography as well as to delineate the lesion size and margins. CTA is not used on a routine basis due to the presence of metal hardware.
Management options for traumatic pseudoaneurysm of the peroneal artery are varied and controversial. 2 Open surgery involves achieving proximal and distal vascular control, followed by evacuating the haematoma, and the resultant arterial wall defect repaired by primary closure or secondarily using a venous patch graft. Endovascular coil embolization would have been the treatment of choice in this patient before rupture, as the posterior tibial artery is the dominant arterial supply to the foot and, therefore, justify the sacrifice of the peroneal artery. Other options include ultrasound-guided occlusion with thrombin injection with post-therapeutic courses being often uneventful (93%) with resultant low morbidity (5%) and mortality (2%) rates. 2
This patient presented 45 days after the initial trauma in an anaemic state, having bled from an external fixator pin site. We propose several possible mechanisms to explain the aetiology of the traumatic pseudoaneurysm of the peroneal artery in our case. The initial traumatic impact, compounded by the onset of compartment syndrome, may have disrupted the integrity of the deep-seated proximal peroneal artery. Another likely mechanism is iatrogenic arterial injury during external fixator pin drilling despite placing the pins in the safe zones. 3
Sala et al. 4 described a case of traumatic pseudoaneurysm of the peroneal artery in the mid-leg region following Taylor frame application and open docking site procedure with bone transport and have postulated arterial damage to have occurred during the osteotomies for the segmental excision of the fibula and tibial cuts. Kurian et al. 5 described a case of traumatic pseudoaneurysm of the peroneal artery proximal to the ankle joint following bimalleolar fracture fixation and postulated either trauma due to drilling or injury by the fracture fragments during the initial trauma. In our case, the site of pseudoaneurysm is more proximal, and we postulate that initial vascular damage could have been due to the sharp fracture fragments, tissue dissection and manipulation of the fractured ends of the bone during reduction or during the process of drilling for fixation of the external fixator. However, the absence of fracture fragment in relation to the site of the pseudoaneurysm and correct placement of the Schanz screws (Figure 1) are noted. We postulated that iatrogenic injury to the peroneal artery has been caused during the process of drilling of the Schanz screws.
No case reports were found in the literature of traumatic pseudoaneurysms of the lower limb as a complication arising from compartment syndrome or due to external fixator screw fixation and of proximal peroneal artery pseudoaneurysms. 1
Traumatic pseudoaneurysms may present either in the acute setting (in a majority, within a few weeks after the surgical intervention or trauma) or as a late sequalae (less common, presenting after many weeks to years). A high index of suspicion is needed by the clinicians when evaluating a patient presenting with bleeding from an external fixator pin site and a traumatic pseudoaneurysm should be excluded using angiography or colour Doppler ultrasound, as the presence of distal pulses does not preclude a pseudoaneurysm or other vascular complications.
In conclusion, iatrogenic injury to the peroneal artery during drilling for Schanz screw insertion seems to be the most likely cause of the traumatic pseudoaneurym in this case. A high degree of suspicion and vigilance needs to be maintained to detect pseudoaneurysms following proximal tibial fractures and early intervention by endovascular or surgical methods is recommended in such cases.
Footnotes
Author contributions
MRI contributed to collection of data, performing a literature search, formulating the case report and its discussion. BH (the supervising author) included reviewing the case report and adding inputs to the discussion.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.