
Abstract
Circumferential constriction in limb will lead to distal limb ischaemia. This is a potentially reversible condition but it has a drastic consequence if undiagnosed. We described a patient with underlying diabetes mellitus presented with persistent lower limb linear circumferential ulcer and developing subacute limb ischaemia distal to the ulcer. During further wound dressing, a rubber band was detected in the wound. Surgical exploration removed the rubber band and its circumferential constriction effect. As a result, the ulcer healed uneventfully and the distal limb perfusion improved clinically. A scoring index consisted of contributing risk factors was proposed to facilitate the diagnosis. A flow chart was proposed to serve as a treatment protocol to ensure logical and comprehensive management. We hope the proposal of the new term and flow chart can help improve the threshold of recognition and for salvage of potentially devastating limb ischaemia.
Keywords
Introduction
Rubber band is an elastic loop of rubber that commonly used for holding multiple objects together. Although there is a warning that rubber band should not be used in the extremity, it is still always being neglected. For neuropathic elderly with limited self-care ability and social or familial support, the use of rubber band in the lower extremity poses their lower limb at high risk of ischaemic change. We would like to present an uncommonly encountered case study for better awareness of this condition and prevention of further cases.
Case report
A 75-year-old man with diabetes mellitus, hypertension and hyperlipidaemia presented with non-healing left ankle ulcer and left leg cellulitis for 2 weeks. He was admitted as an inpatient. He and his family member could not recall any trauma before ulceration. X-ray of left ankle and leg showed no underlying osteomyelitis and commented unremarkable. There was persistent discharge over left lower leg wound despite intravenous Tazocin and wound swab revealed heavy Staphylococcus aureus, moderate Diphtheroid bacilli and scanty Pseudomonas aeruginosa. Left leg cellulitis subsequently subsided after antibiotics. However, wound healing progress was poor despite antibiotic cover, good diabetic control (HbA1c fewer than 6%) and intense wound care for 4 weeks.
Lower limb assessment showed dorsalis pedis and posterior tibialis arteries pulses were not palpable over the left leg. Also, there was generalized purplish discoloration (distal to the wound) from toe to mild calf with delayed capillary refill time of left leg. Neurological assessment showed deceased protective sensation of left foot. Wound assessment revealed that it was a linear circumferential constriction wound at the left lower leg above the ankle. Medial part of the circumferential wound had already healed with linear scar. There was thick yellowish discharge from the lateral wound, and wound base presented with sloughy yellowish tissue. Owing to the circumferential nature of wound, underlying foreign body constriction was suspected. Sterile equipment was used to probe into the wound. Rubber-band-like material was found in wound bed (Figure 1).

Clinical photos showing rubber band beneath the wound.
Exploration of the left leg wound was performed in view of the purulent wound discharge and suspected retained rubber band. Intraoperatively, an intact rubber band was found embedded into the subcutaneous layer in the linear circumferential wound, which was about 6 cm proximal to ankle level. The width of the wound was 5 mm. There was partial scar formation over the rubber band without exposure of underlying muscles or tendons. There was no abscess collection and no neurovascular structures involved with a viable wound edge. The rubber band was cut into two segments and removed easily, followed by thorough debridement and curettage of the wound. Intraoperative imaging confirmed no residual radioopaque foreign body. The wound was loosely sutured with interrupted stitches to allow for pus drainage. After the foreign body removal and intense wound care, left leg linear (Figure 2). Left leg circulation improved gradually with no more purplish discoloration and capillary refill time within 2 s resumed with palpable dorsalis pedis and posterior tibial pulses, comparable to the other side.

Clinical photo showing the healed wound after treatment.
Discussion
Ulcers in the lower limb were common in diabetic patients. Causes included angiopathy and peripheral neuropathy. 1 Whenever there was persistent ulcer with adequate wound dressing, underlying causes should be sought. Local causes included underlying osteomyelitis, untreated infection or foreign body beneath the wound. Patient factors, including poor nutrition and poor glycaemic control, should also be optimized.
Previous literature had described rubber band tied circumferentially in the wrist, 2,3 arm 4 and thigh. 5 The presence of rubber band causing a non-healing ulcer in neuropathic elderly’s leg had not been described in the current literature. A linear circumferential constriction scar, a non-healing ulcer with discharging sinus and the presence of ischaemic changes distal to ulcer gave rise to the typical pattern of wound as reported in the rubber band syndrome. 2,6 The rubber band would cut into the tissues. As the gap produced by the pressure necrosis by rubber band was only a few millimetres, the wound might be partially healed after passing through stages of infection, granulation, fibrosis, wound contraction and skin epithelialization over the band, leaving a circumferential scar mark on the surface. 5
A linear circumferential persistent ulcer with signs of ishcaemia distal to the ulcer should raise the possibility of rubber band syndrome. The constriction by the rubber band was similar to the eschar in burn injury. The eschar would cause a local constriction with a distal ischaemic pattern, which was also true for rubber band. Operative removal was indicated for both eschar and rubber band, aiming to remove the constriction and restore the distal circulation. However, in contrast to eschar, rubber band might cut into the tissues as the band had tension, which in turn caused more oedema distally. A more swollen limb would be constricted by the band more and this started a vicious cycle. Moreover, after the rubber band buried into the tissue, skin would epithelialize over the band and the wound could heal. This made the rubber band undetectable from the outside. Patient might just present with distal limb ishcaemia without any superficial wound.
Rubber bands were put on the limbs for different purposes. In some countries, the band might put on the upper limbs for decorative purposes. Previous literature described rubber band embedded in the wrist in Indian, known as the Dhaga syndrome (the Moli Dhaga in the Hindi language, which meant a sacred thread). 7 In the elderly, rubber band was sometimes put on the lower limb to tighten the loosen socks. However, this was not a recommended practice. The presence of rubber band in the leg in this patient could be due to patient’s education problem or a carer problem.
Our patient could not recall the reason of putting rubber band around the leg, but it was believed that he might put it there with the intention to tighten the loosen socks, which is a cultural habit quite commonly seen in Hong Kong elderly. He also had no insight on the consequence of rubber band being tighten around the lower extremity. In addition, he was not involved in podiatric care in the earlier part of his management. Podiatrist is a professional who specialized in lower limb pathology and could provide a comprehensive care with a special role for the neuropathic elderly, in terms of patient’s education, progress follow-up and wound management. Interventional procedures could also be provided by podiatrists. The presence of ischaemic sign in the limb with a constriction linear scar and ulcer with discharging sinus in a neuropathic elderly should alert the possibility of retained foreign body inside. If the patient had ever received podiatry care before this incident, he would have better concept and insight of the danger of rubber band around the extremity and importance of foot care. However, the role of podiatrist in geriatric care is still limited since elderly patients have very limited access to podiatric service and education.
As time went by, in the presence of peripheral neuropathy and oedema of leg, the rubber band constricted and embedded into the subcutaneous layer of the leg, causing the non-healing infective wound with discharging sinus and surrounding cellulitis. If the rubber band could not be discovered, it might have further impaired the vascular system causing non-irreversible gangrenous change of the foot and ankle region, which was distal to the constriction. Similar to other regions, the gradual penetration of rubber band in the leg was painless and without neurovascular symptoms. 7 In our patient, the dorsalis pedis and posterior tibial pulses were palpable after removal of the rubber band. This made it an arterial constriction more likely than a venous stasis by the rubber band. In the later stage, the X-ray of the affected region might show a ‘constriction sign’ with normal underlying bone. Preoperative magnetic resonance imaging (MRI) would be useful if the rubber band had already burrowed into the deep structures. 2 However, MRI is often difficult to be arranged in the acute setting. In contrast, ultrasonography is getting more easily available nowadays. Radiolucent foreign bodies are visualized as hyper-echoic foci with accompanying acoustic shadows. 8 In ultrasonography, acoustic shadowing can differentiate foreign body from scar tissue, gas bubble and normal intermuscular fascia, because they are void of acoustic shadowing. Accuracy, sensitivity and positive predictive value for foreign bodies by ultrasonography were determined as 94.16%, 99.08% and 94.13%, respectively. 8 The authors suggested that ultrasonography should be considered in non-healing wound to screen for underlying foreign body.
In Hong Kong, the increase of ageing population poses a bomb to the health care system. There will be 34% elderly in the entire population in 2066 by the estimation of the Hong Kong Population Projections 2017–2066. With ageing population, more medical attention and expenditure were required for the elderly. For elderly who have limited self-care ability and social or familial support, even a small incident can put them at high risk. Therefore, the awareness of external risk factors is of paramount importance and should be addressed in a proper way. However, whether our medical system could meet the emerging urge of this rising population with proper comprehensive care is our concern. In this case, it proved that the role of the podiatrist in geriatric care should not be underemphasized. For circumferential constriction wound cases, the presence of rubber band was difficult to be detected under X-ray until the rubber band has eroded the bone. As a result, the X-ray, in this case, was commented unremarkable.
The current management of chronic wound included regular dressing of the wound and treatment of any underlying infection. In the management of lower limb ulcer, a holistic approach should be used. The diabetic control should be optimized in this group of patient to facilitate wound healing. Peripheral vascular status of the lower limb was another important aspect in the management. Vascular interventions should be considered to optimize wound healing in severe peripheral vascular disease. For patients with a complicated wound, the authors recommended referral to podiatrist should be made.
With the ageing population, together with the cultural habit of using rubber band to tighten the loosen socks, inadequate foot care education, poor elderly self-care ability and limited podiatric elderly service, it is not surprised to see more patients like this in the future. Hence, the authors would like to call for a new term – Acquired Circumferential Ischaemic Constriction Syndrome (ACICS) – to describe this unique phenomenon. We proposed a scoring index to stratify the risk of ACICS (Table 1). In patients with ACICS scoring index ≥6, active searching for peripheral neuropathy, vascular insufficiency and foreign body beneath the wound, including advanced imaging, multidisciplinary approach and advanced wound management including podiatrist referral, should be used (Figure 3). Although one simple case might not be sufficient to generate a scoring index, the authors would like to take this opportunity and use this score to raise the awareness of medical professionals about underlying constriction foreign body in an ulcer, such as a rubber band.
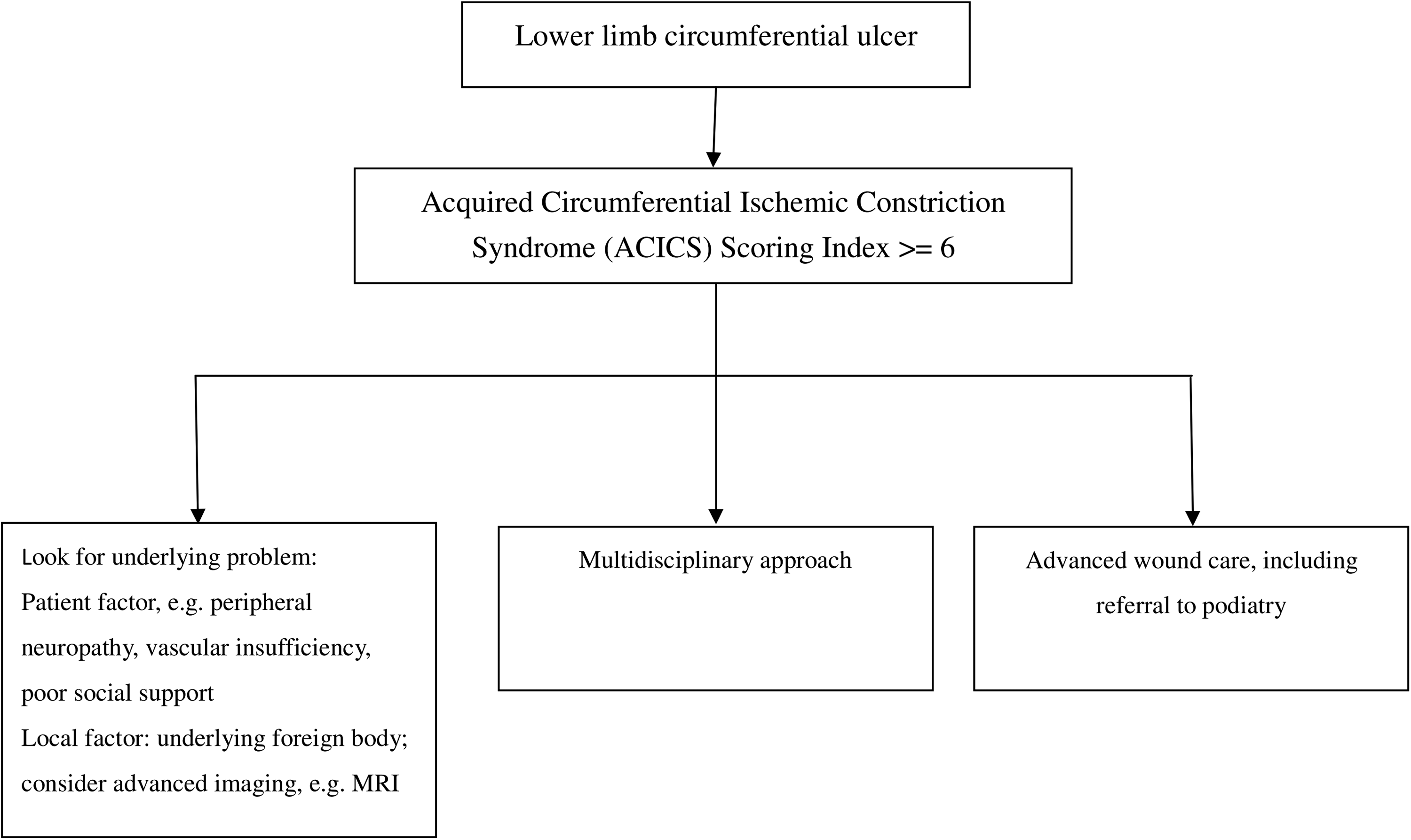
Management algorithm.
ACICS scoring index.
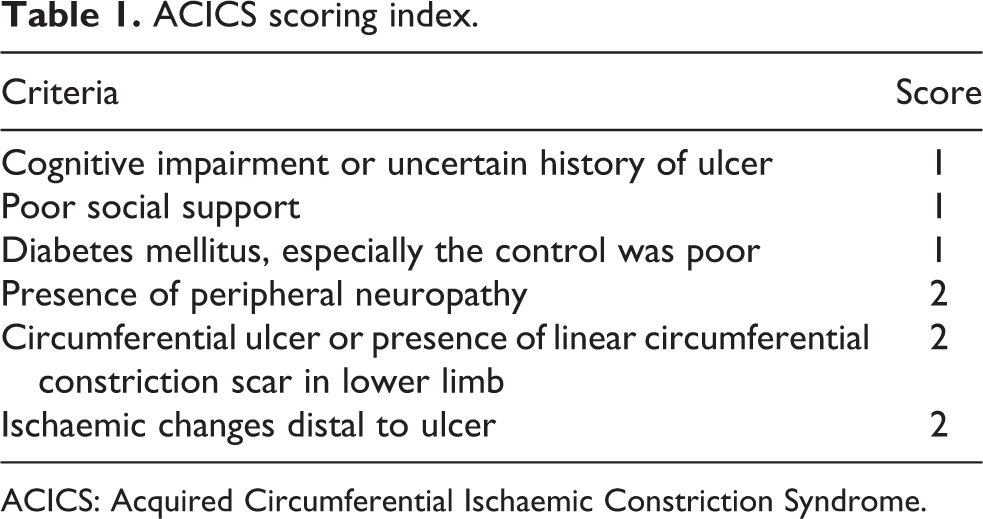
ACICS: Acquired Circumferential Ischaemic Constriction Syndrome.
Conclusion
We reported a patient with rubber band-induced persistent circumferential ulcer in the lower leg to increase the recognition of this uncommon but potentially devastating condition. In a persistent non-healing ulcer, underlying foreign body should be actively looked for. For lower limb ulcers with ACICS scoring index ≥6, a holistic assessment and management of the ulcer should be used. This included a multidisciplinary approach, searching for underlying foreign body and advanced wound management, including referral to podiatrist. Reversible risk factors should be corrected, including optimization of diabetic control, achievement of better social support and screening for peripheral neuropathy and vascular insufficiency to make an earlier diagnosis. Last but not least, proper education of patients and their carer should be reinforced. Avoid putting constriction band such as rubber band around limbs would be the most important prevention for the ACICS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.