
Abstract
Background:
Lack of local data concerning the long-term clinical outcomes of scarf osteotomy in Hong Kong.
Methods:
This is a retrospective review of 75 patients (88 feet) who underwent scarf osteotomy with a mean follow-up of 94.20 months (60–144 months). Clinical ratings were based on visual analog scale (VAS) and American Orthopaedic Foot & Ankle Society (AOFAS) scale. Weight-bearing radiographs were used to perform angular measurements: (i) hallux valgus angle (HVA), (ii) intermetatarsal angle, (iii) distal metatarsal articular angle, and (iv) tibial sesamoid position before operation and at the time of latest follow-up.
Results:
The mean overall AOFAS scales improved from 29.66 (5–49) points preoperatively to 86.83 (39–100) points at the time of final follow-up. The VAS improved from 6.61 (5 to 9) to 0.66 (0 to 4). The average HVA correction was 25.42 (8–46). The 8- to10-year recurrence rate (HVA > 20) was 31.80%. A higher degree of preoperative HVA predicts higher recurrence rate.
Conclusion:
Scarf osteotomy is an effective procedure for symptom control and improvement in radiological parameters for hallux valgus deformity. However, recurrence rate is relatively high.
Hallux valgus is a common orthopedic condition, which presents with progressive lateral deviation and pronation of hallux, increased intermetatarsal angle (IMA), and painful bunion. There are many different types of surgical treatment, and scarf osteotomy is one of the commonly used procedures. It was first described as a sagittal Z shape osteotomy by Meyer in 1926. 1 Burutaran then applied it in 1976. 2 Afterward, it was modified and popularized by Weil and Borelli in the United States 3 as well as by Barouk in France. 4
In fact, “scarf” is a carpentry term. The procedure of scarf osteotomy is operated by making a woodwork like Z-step cut over the first metatarsal (MT1) bone. The cut helps to create a scarf joint that corrects the IMA. This osteotomy has inherent intrinsic stability, which allows early weight-bearing.
However, scarf osteotomy has various limitations. It is contraindicated in patients with severe first tarsometatarsal joint instability, osteoarthritis of the first metatarsophalangeal joint, and severe osteoporosis. Besides, various kinds of complications were also noted after this procedure. Recurrence is one of the common long-term complications. Peter Bock et al. reported that 10-year recurrence rate was 30%. 5
Patients and methods
This was a retrospective review of 88 feet in 75 patients, including 68 females (90.67%) and 7 males (9.33%) (Table 1). All the patients presented with symptomatic hallux valgus deformity underwent scarf osteotomy from January 2006 to December 2009. In 5 (5.70%) of the 88 feet, an Akin osteotomy was also performed. The mean patient age at the time of operation is 54.60 (range 19–78) years; the mean follow-up duration is 94.20 (60–144) months; and the meantime for the latest radiological assessment was 67.84 (50–126) months.
Patient demographics.
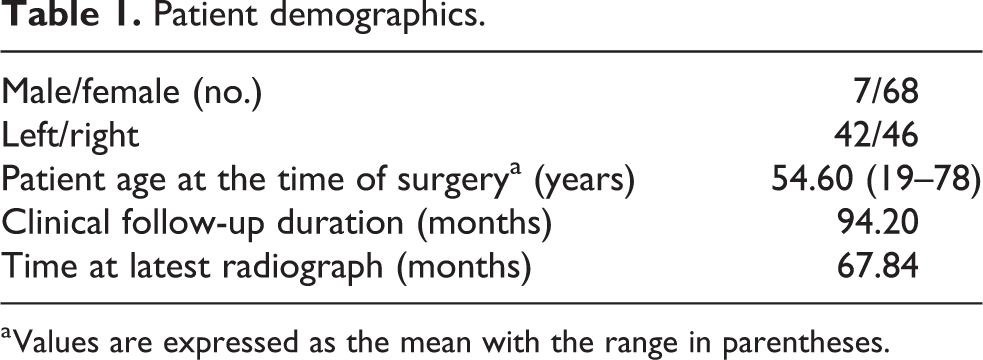
a Values are expressed as the mean with the range in parentheses.
Inclusion criteria for scarf osteotomy in the current study are symptomatic hallux valgus deformity with hallux valgus angle (HVA) more than 20° and failed conservative management. Exclusion criteria include previous forefoot surgery, rheumatoid arthritis, peripheral neuropathy, and complex forefoot malalignment, requiring additional osteotomies at the lesser metatarsals.
In this study, clinical outcomes were assessed and evaluated by using American Orthopedic Foot & Ankle Society (AOFAS) hallux metatarsophalangeal–interphalangeal scales 6 and visual analog scale (VAS) before operation and at the time of latest follow-up.
For radiographic evaluation, weight-bearing dorsoplantar and lateral radiographs were assessed preoperatively, early postoperatively, and then yearly at follow-up. HVA, IMA, and distal metatarsal articular angle (DMAA) were measured following the recommendations from the Ad Hoc Committee of the AOFAS. 7 The position of the tibial sesamoid measurement was based on four gradation systems, as determined by the position of the medial sesamoid in relationship to the bisection of the MT1. 8
Statistical analysis
Data analysis was made by using the Statistical Package for Social Sciences, version 22. The Kolmogorov–Smirnov test was used in the distribution of cases. For normal distribution data, the paired sample t-test was used as the parametric test. For data showing irregular distribution, Wilcoxon test was used. Furthermore, crosswise table statistics (χ2 tests) were used to compare the categorical variables. The data were tested with a logistic regression model to determine the preoperative predictive recurrence factors.
All p values were two-sided, using a significance level of p = 0.05.
Surgical technique
The patient was placed supine. A medial longitudinal incision was made over MT1. The lateral soft tissues were released by a separate incision along with the first webspace. The longitudinal osteotomy along MT1 ended distally at approximately 5 mm proximal to the MT1 head articular cartilage, while proximal part of the osteotomy ended approximately 10 mm distal to the first metatarsocuneiform joint. The Z osteotomy was completed by two short transverse cuts at both ends of the longitudinal osteotomy, which were parallel and at 60° angle to the longitudinal axis. After cautiously releasing both fragments, the plantar metatarsal head fragment was shifted laterally until the hallux deformity was corrected to acceptable alignment. If there was still residual hallux deformity, Akin procedure would be performed too. Internal fixation was achieved with two Barouk screws. Afterward, the prominent medial bony eminence was resected, followed by medial capsulorraphy.
All patients in this study had the same postoperative regimen and had regular follow-up in the standardized protocol. They were allowed to bear weight on a forefoot off-load shoe. Bulky dressing was provided and maintained intact until follow-up. The first follow-up was arranged in approximately 2 weeks after the operation for wound assessment and changing to light dressing. Splintage or taping was not provided. Forefoot off-load shoe (Darco Boot) was kept for 6 weeks. Standard weight-bearing radiograph of foot was checked at 6 weeks, 6 and 12 months postoperatively, and then annually. AOFAS hallux metatarsophalangeal–interphalangeal scales and VAS would be assessed at the same time during follow-up.
Results
The criteria for HVA were accepted and considered as normal when it was less than 15 in the radiographic evaluation; greater than 15 but 20 or less was determined as a mild deformity; 20–39 as moderate deformity; and 40 or greater as severe. 9 It was found that 60 feet were considered as moderate and 28 feet were considered as severe.
Clinical assessment
The AOFAS hallux metatarsophalangeal–interphalangeal scales improved significantly from preoperative mean of 29.66 (range 5–49) to 86.83 (range 39–100) at the latest follow-up. All AOFAS subscores in pain, function, and alignment improved significantly (Table 2).
Comparison of preoperative and postoperative clinical outcomes.
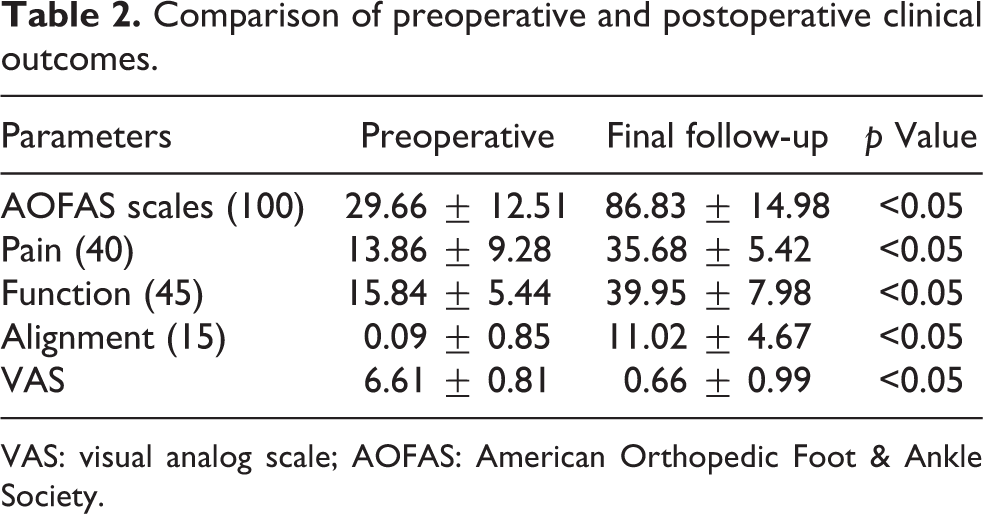
VAS: visual analog scale; AOFAS: American Orthopedic Foot & Ankle Society.
Pain subscores (40 points) increased from a mean value of 13.86 points (0–20) preoperatively to 35.68 points (20–40) postoperatively (p < 0.05). Total functional subscores (45 points) improved from 15.84 (4–29) to 39.95 (9–45) after the operation (p < 0.05). The average VAS was also improved from 6.61 (5–9) preoperatively to 0.66 (0–4) at the final follow-up (p < 0.05). Alignment of the hallux also improved significantly (mean preoperative value 0.09 (0–8) points and 11.02 (0–15) points postoperatively; p < 0.05).
Radiological assessment
In the radiological evaluation, a significant degree of improvement was observed, including the postoperative HVA, IMA, and tibial sesamoid position (p < 0.05) (Table 3).
Comparison of preoperative and postoperative radiographic outcomes.
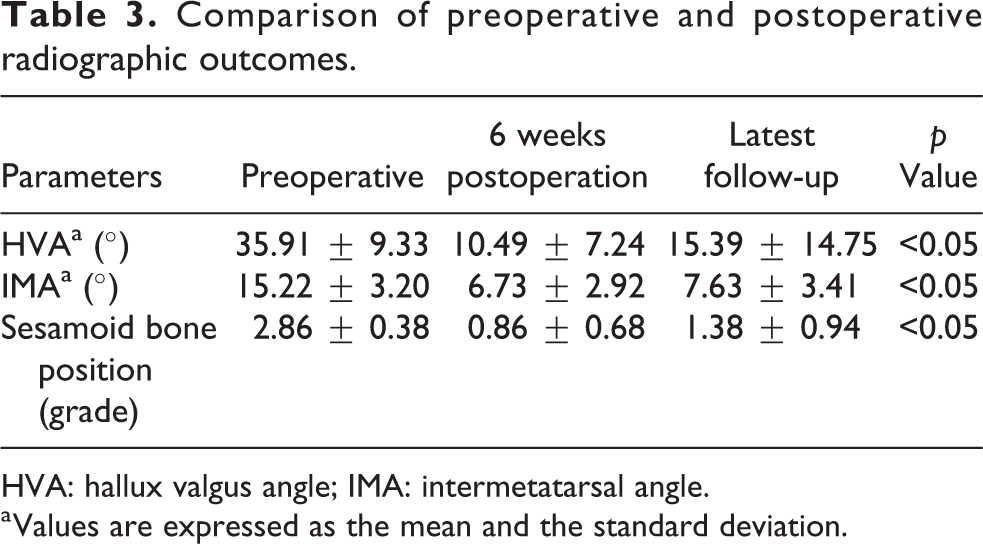
HVA: hallux valgus angle; IMA: intermetatarsal angle.
a Values are expressed as the mean and the standard deviation.
As the figures showed, the average HVA improved from preoperatively 35.91 (20–64) to 10.49 (−17 to 37) at early postoperative follow-up. However, the average HVA increased to 15.39 (−32 to 59) at the latest follow-up (average time for latest X-ray was 67.84 (50 to 126) months) (Figure 1).
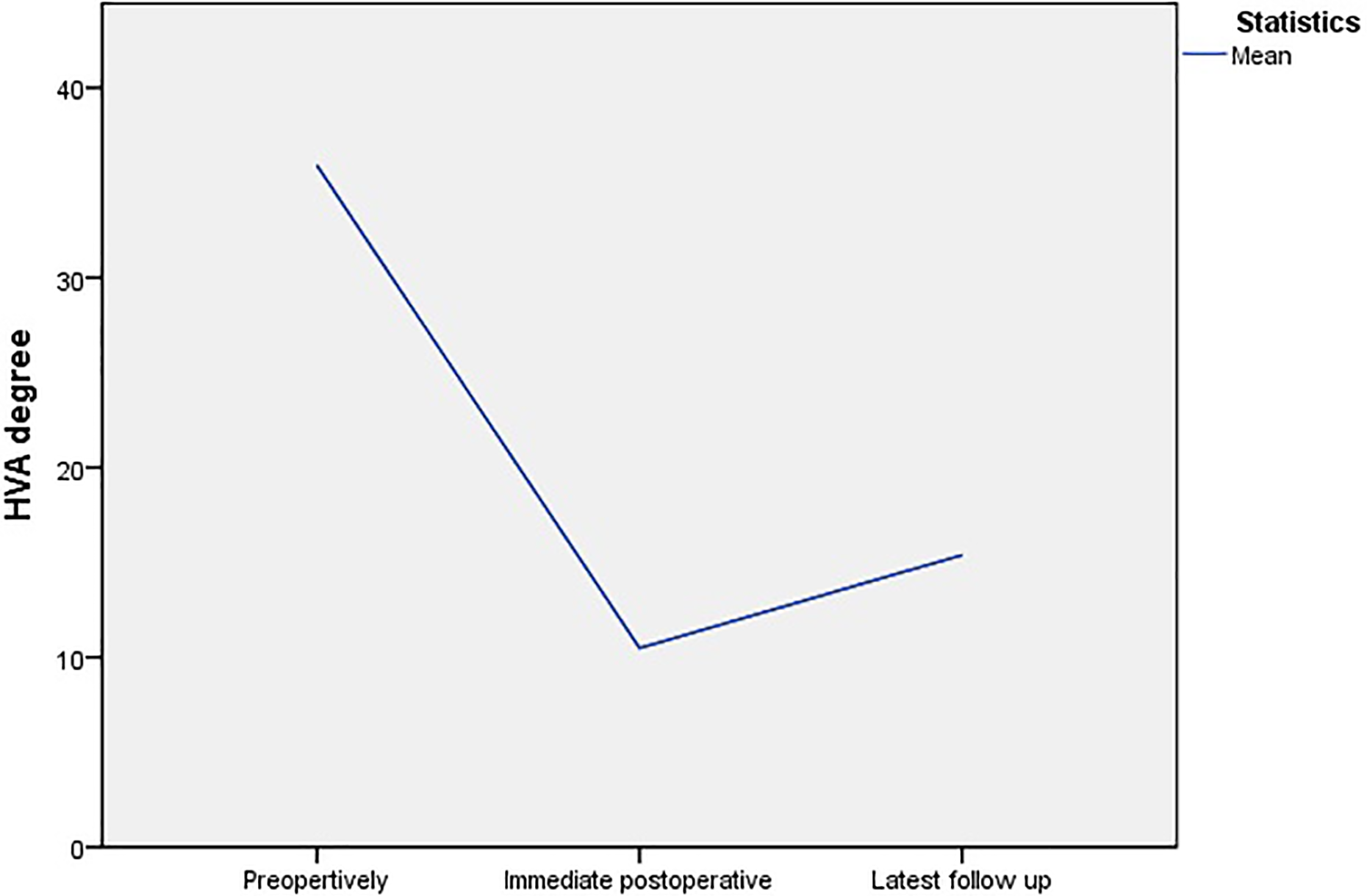
Development of HVA preoperatively and at the intermediate and latest follow-up. HVA: hallux valgus angle.
Recurrence
In this study, it was defined that HVA > 20° as recurrence. 10 The radiographic recurrence occurred in 28 (31.80%) of the 88 feet at the time of the latest follow-up (Figure 2). Incomplete correction was noted in 5 feet at immediate postoperative follow-up. Seventeen (60.71%) of them with symptom and two (7.14%) of them need a secondary operation.
Recurrence percent.
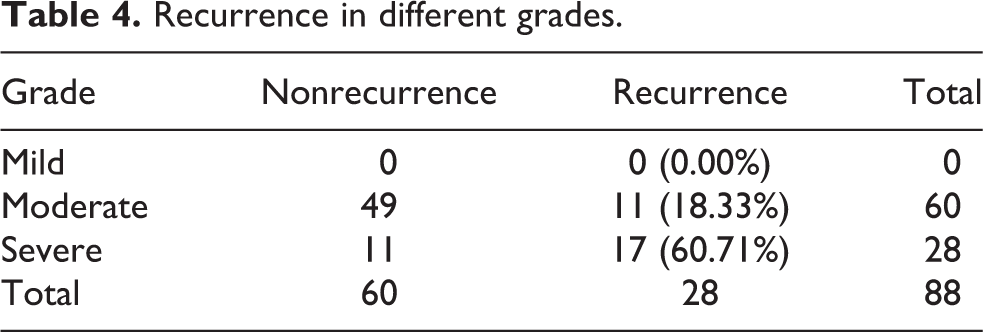
There were 11 recurrence cases noted in moderate deformity group (18.33% of all the 60 feet) and 17 recurrence cases were noted in severe deformity group (60.71% of all the 28 feet) (Table 4).
Recurrence in different grades.
To study what risk factors had significant influence on recurrence, a statistical test (logistic regression) was employed. Gender, laterality of deformity, number of feet with operations, age at operation, Akin procedure, preoperative HVA, preoperative IMA, and preoperative DMAA were studied for possible correlations with recurrence. It was shown that only preoperative HVA was the significant risk factor related to recurrence. It was found that the higher the preoperative HVA was, the higher the recurrence rate it would be. It was found that for every 1° of HVA increased, the recurrence rate was increased by 1.172 times (Table 5).
Recurrence factors analysis.
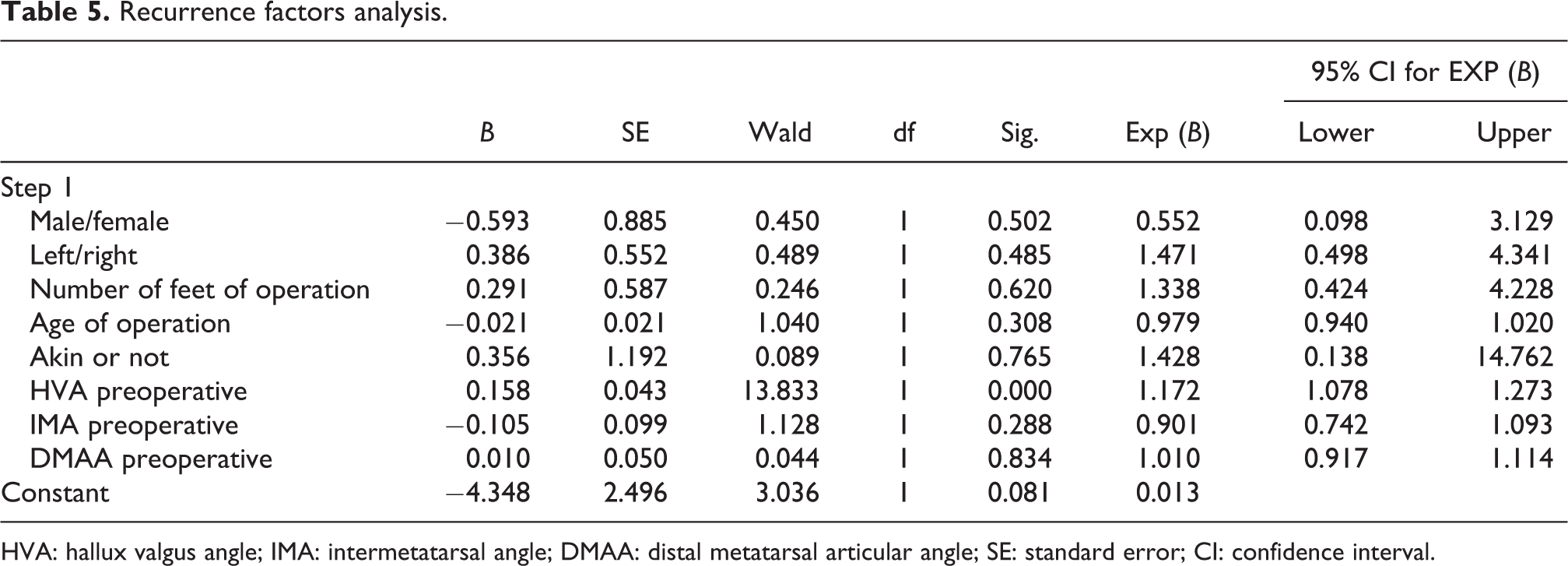
HVA: hallux valgus angle; IMA: intermetatarsal angle; DMAA: distal metatarsal articular angle; SE: standard error; CI: confidence interval.
Complications
In addition to recurrence, other complications were also noted in this study. Firstly, hallux varus were noted in 7 feet (7.95%). Secondly, superficial wound infection was seen in 1 foot (1.14%) and improved after a course of antibiotics treatment. Thirdly, skin impingement by sutures was found in 2 feet (2.27%) and the removal of stitches under local anesthesia was performed. Lastly, three cases (3.41%) of screw impingement were found, and all of them were treated with the removal of screws.
Discussion
Scarf osteotomy has been shown to be an effective procedure for hallux valgus deformity correction, 11,12 which has been widely used in recent decades. However, there was scarce literature review regarding the long-term result of this procedure. 5 Therefore, this study provides insight on efficacy of this procedure, long-term complications, and the risk factors for recurrence in a local hospital here.
In our study, there was a significant improvement in the AOFAS scales, VAS, HVA, and IMA. Our results were similar to other prior published papers. 3,5,11,12
Although the present study demonstrated that the scarf osteotomy resulted in a significant improvement in symptom and radiographic parameters earlier on, however, a relatively high radiographic recurrence rate was found at our latest follow-up. In other published studies, recurrence was a known common complication, with short- to mid-term recurrence rate of 3.57–10% 11 –15 and long-term recurrence rate of 30%. 5 Long-term recurrence rate of our study was 31.80%, which was similar to other published studies. 5 In our recurrence cases, 60.71% of the patients were symptomatic and 7.14% (two patients) of them required a secondary operation.
The risk factors of recurrence have generally been mentioned, including high preoperative HVA, IMA, DMAA, joint incongruity, insufficient reduction of the sesamoid bones, insufficient correction, and the steep surgical learning curve. 9,15,16 Based on our study, preoperative HVA influenced the recurrence rate most. Yet the preoperative IMA and DMAA did not significantly affect the outcome.
Limitations of this study
It was difficult to trace every single patient back for review, especially those who had had operations for almost 10 years. The loss of those would definitely lead to insufficiency of data collection on clinical assessment and imaging findings. It might be one of bias for our data analysis. Furthermore, some patients were called back after missing follow-up for years, which caused difficulty to assess the time of occurred recurrence.
Besides, the Department of Radiology in our hospital merely began digitization in 2005, illustrating an imperfection of collecting all the preoperative radiographs of a major part of patients received scarf osteotomy before 2006; also, diverse types of operation were performed for hallux valgus before 2006, instead of concentratedly or massively applying scarf osteotomy; we, therefore, decided the data collection of this study started from 2006. In terms of the insufficient of a few data before 2006, it assuredly limits our finding of a valid long-term result.
Conclusions
Scarf osteotomy is an effective procedure for achieving satisfactory angular improvement in hallux valgus deformity, symptom control, and functional improvement. However, relatively high recurrence rate was noted and a proportion of those recurrence would be symptomatic. The higher degree of preoperative HVA was correlated with higher recurrence. Patients in severe group would have higher recurrence rate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.