
Abstract
Old simultaneous complex fracture–dislocation of the first metatarsophalangeal (MTP), Lisfranc, and naviculocuneiform joints as an overwhelming injury has not been reported in the literature yet. In a 29-year-old man, 6 months following the trauma, the medial column of foot was reconstructed using iliac tricortical bone graft from navicular to the first metatarsal. Arthrodesis of the second and third tarsometatarsal joints and resection arthroplasty of the first MTP joint were done. His clinical and radiographic evaluation after 18 months revealed an acceptable function with returning to pre-injury job but with some limitations in recreational activities.
Level of evidence: level 4
Introduction
Midfoot fractures are uncommon injuries with estimated prevalence of 1.7 for either navicular or cuboid and 0.2 for cuneiform bones in 105 people per year. Mechanism of midfoot injuries, commonly occur among young patients, mostly is falling down, twisting injuries, and traffic accidents. 1 Lisfranc injuries are seen more, with the incidence of about 9 in 105 person per year. 2 Undiagnosed Lisfranc injuries are usually seen in about 20% of cases. 3 Moreover, first metatarsophalangeal (MTP) joint dislocation is uncommon injury with dorsal, lateral, or plantar direction of dislocation. 4 –6 Old first MTP, Lisfranc, or Chopart injuries could result in the functional loss with lifelong disabilities such as midfoot collapse, fixed deformity, pressure ulcer, arthrosis, and bothersome pain. Operative management of these injuries is fraught with several possible complications such as soft tissue coverage breakdown, wound dehiscence, infection, painful devices, iatrogenic injuries to adjacent joints and neurovascular bundles, and inability to achieve anatomic reduction.
Few studies have presented acute floating metatarsal and floating cuneiform bones 7 –9 ; however, to the best of our research and knowledge, the presented case is the first in the literature that describes simultaneous complex fracture–dislocation of the first MTP, Lisfranc, and naviculocuneiform joints in association with malunion of second and third metatarsal neck fractures, treated 6 months after a high energy trauma.
Case report
A 29-year-old wheelchair-bound man was consulted because of severe deformity and pain of the right foot. He had a history of motorcycle to car accident about 6 months previously. He had associated fractures of right distal radius, both bones of right forearm, supracondylar of right humerus, and posterior cruciate ligament avulsion fracture of right knee which had been undergone surgical reduction and fixation. He was admitted in the intensive care unit (ICU) for about 2 months because of head trauma.
The right foot examination showed swollen fixed midfoot rocker bottom, forefoot abduction, big toe extension, and heel valgus deformities. Neurovascular status of the foot was normal. Although he completely recovered from head trauma with well union of previous fractures, he could not walk independently due to significant foot pain and severe elbow stiffness. Radiographs revealed generalized osteoporosis with malunion of the second and third metatarsal neck fractures. Furthermore, dorsomedial fracture–dislocation of right first MTP joint; dorsal fracture–dislocation of the first, second, third, fourth, and fifth tarsometatarsal (TMT) joints; and plantar lateral fracture–dislocation of cuneiform bones from naviculocuneiform joint were detected (Figure 1). Computed tomography (CT) scan confirmed the diagnosis. Interestingly, sesamoid bones were intact with multiple free fractured fragments in plantar of the first metatarsal head from plantar surface of dorsally dislocated proximal phalanx (Figure 2).
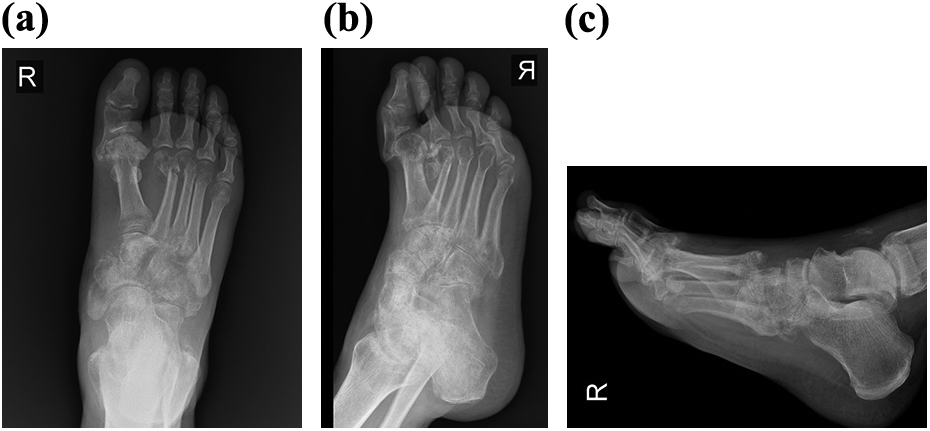
Anteroposterior (a), oblique (b), and lateral (c) radiographs showing dorsal fracture–dislocation of the first MTP and plantar floated cuneiform bones. Malunion of the second and third metatarsal neck fractures is obvious. MTP: metatarsophalangeal.
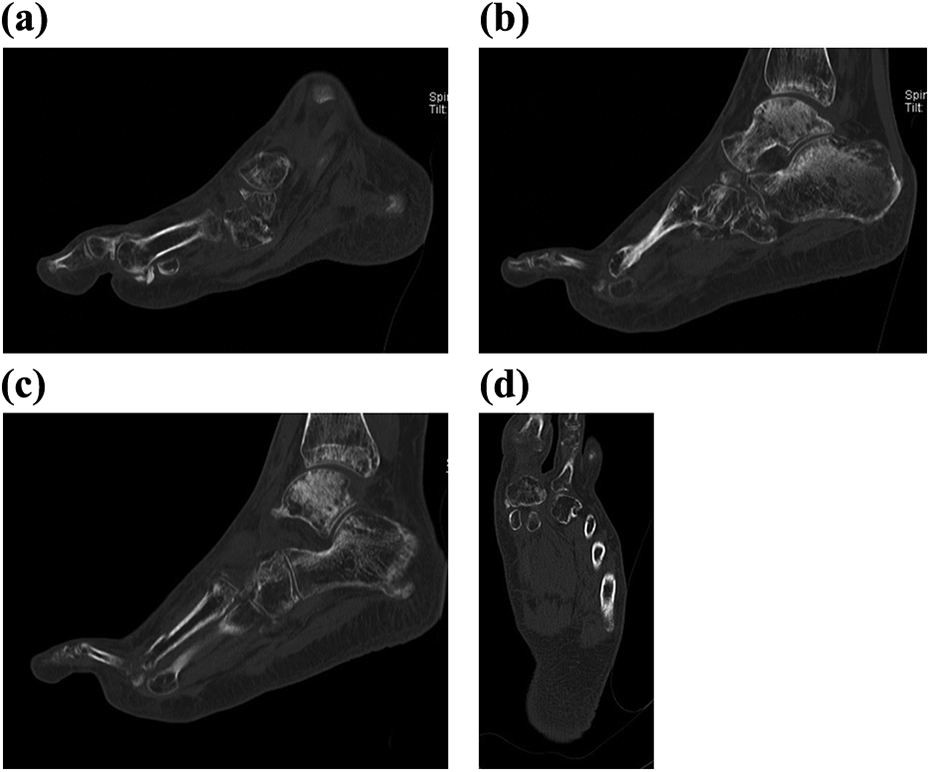
Sagittal CT scan cuts from first metatarsal to the third one (a to c) revealed dislocated TMT and naviculocuneiform joints. Intact sesamoid bones with free bone fragments in plantar of the first metatarsal head are seen in the coronal (d) and sagittal (a) sections of the foot. CT: computed tomography; TMT: tarsometatarsal.
In the operating room, first through medial approach, the first MTP joint was exposed. As expected, reduction was impossible, so plan was resection arthroplasty because of the next stage, arthrodesis of TMT and naviculocuneiform joints. After removal of the adhesion around hallux tendons and fibrotic tissues around the MTP joint and sesamoid ligaments, base of proximal phalanx and free bony fragments in the plantar aspect of the first metatarsal head were resected to achieve reduction of the joint. It appeared that sesamoid bones, intersesamoid ligaments, and the plantar plate did not have any break. The first MTP joint was reduced and fixed using two K-wires. Then through long dorsal longitudinal incision from the talus to shaft of the first metatarsal bone after lateral retraction of extensor hallucis longus and neurovascular bundle, the first and second TMT, intercuneiform, and naviculocuneiform joints were exposed. Also via longitudinal dorsal incision between the third and fourth TMT joints, the third, fourth, and fifth TMT joints were exposed. The bone was very osteoporotic and resorption of some parts of medial and almost all parts of middle cuneiforms was seen. Remnant of cartilages were removed after excision of several free osteocartilaginous fragments from TMT joints. Due to bone loss in the medial of the foot, a tricortical bone graft harvested from right ilium was inserted in the location of bone loss to reconstruct medial and middle cuneiforms. Perfect anatomic reduction was impossible due to severe contracture of soft tissues and tendons. Arthrodesis of the first TMT, intercuneiform, and naviculocuneiform joints was fixed using a locking plate 3.5 from Synthes Company, Switzerland under the guide of fluoroscopy. To have a rigid fixation, talonavicular joint fixation was inevitable. Moreover, arthrodesis of the second TMT and middle cuneiform to the navicular joints was fixed using a locking plate 2.7 from Synthes Company. Then, the third TMT joint was fused after impaction of bone graft and fixed by another locking plate 2.7. The fourth and fifth TMT joints were reduced spontaneously with adequate stability, without fixation (Figure 3).
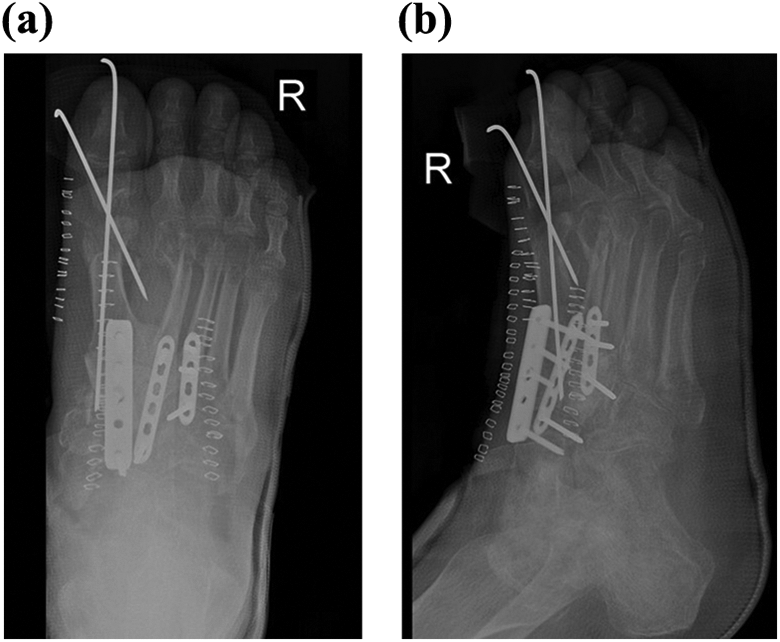
The first post-op radiographs (a and b).
Postoperatively, as per our institutional protocol, non-weight-bearing short leg cast was applied for 6 weeks, followed by a non-weight-bearing short leg slab to initiate range of motion till healing of the arthrodesis, which was about 3 months following the surgery. Two K-wires of first MTP joint were removed 6 weeks after the surgery. Gradually he could start weight bearing without using any aid but wear bigger shoes due to swelling. He complained of pain especially on talonavicular joint; hence, after 1 year, all devices were removed, after confirming the bony union using CT scan.
At 18 months following the primary surgery, he was satisfied without any significant pain and he could return to his pre-op activities and job. On examination, the foot and ankle were stable with little acceptable hindfoot valgus and deformities (Figure 4). Although the range of motion of right big toe interphalangeal joint was 0–40° of flexion, no motion was detected in the first MTP joint, despite resection arthroplasty it became fused. Also the range of motion of right ankle joint was from 10° dorsiflexion to 40° plantar flexion. No passive inversion or eversion was identified in subtalar and talonavicular joints. The outcome was evaluated by American Orthopaedic Foot & Ankle Society (AOFAS) midfoot score, Foot Function Index, and Visual Analogue Scale (VAS) for pain. AOFAS midfoot score was 78 from 100 (mild pain, no limitation of daily activities but limitation in recreational activities, bigger comfort footwear, and some degree of midfoot malalignment observed). Foot Function Index was 16% (pain scale: 26%, disability scale: 12%, activity limitation scale: 10%) and pain VAS score was 2. The last radiographs showed loss of normal longitudinal arch and complete fusion of naviculocuneiforms, medial three TMT, and first MTP joints with slight arthritic changes in the other joints; however, it may be seen more in the future (Figure 5).
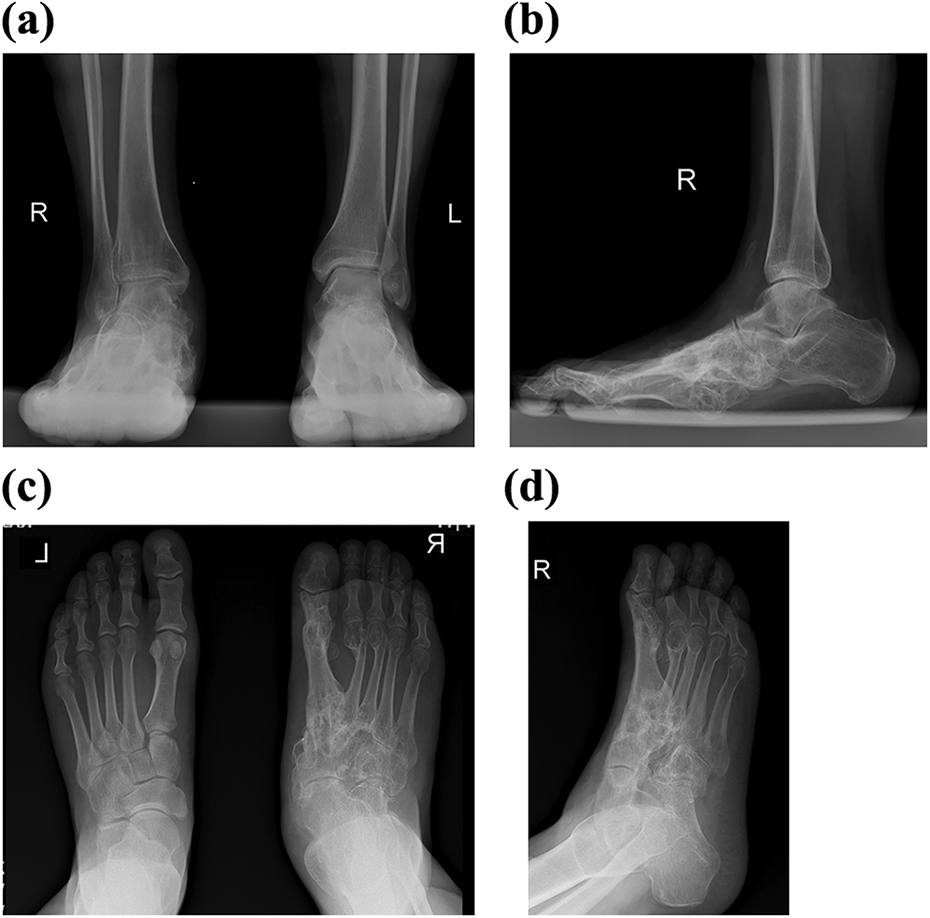
At 18 months postoperatively, arthrodesis of all medial joints except talonavicular is obvious with little loss of medial longitudinal arch (a to c).
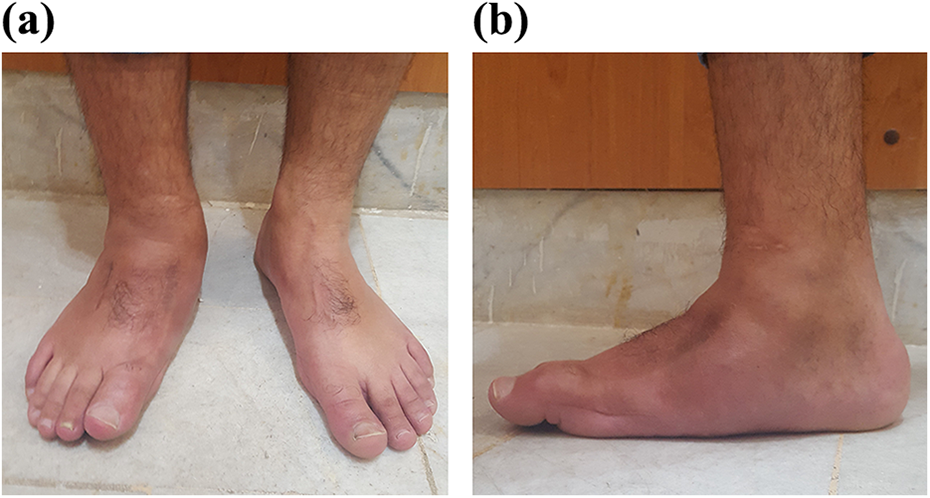
Clinical photography shows loss of medial arch of the foot with little extension deformity of the first MTP joint (a and b). MTP: metatarsophalangeal.
It should be mentioned that informed consent for publication of this case report has been obtained from the patient.
Discussion
The foot is one of the most complex structures of the human beings with many articular surfaces, strong capsules, unique ligaments, multiple fasciae, small functional muscles, and various important tendons in order to support the weight and have a normal locomotion. Complicated injuries to each section of the foot may eventually lead to changes in biomechanics with permanent disabilities.
Neglected foot injuries are very rare terrible injuries with poor outcomes. Subtle midfoot injuries are more common to be missed than first MTP joint fracture–dislocations. Midfoot, especially Lisfranc, injuries can be overlooked in patients with multiple traumas, especially in developing countries, due to lack of surgeon’s knowledge and experience, lack of adequate expert medical personnel, inadequate diagnostic evaluation, and the patient not requesting any medical cares because of several reasons such as being homeless. In neglected cases, more than 6 weeks after trauma, the surgical reconstruction is a dilemma with osteoporotic bones, destroyed cartilages in the dislocated joints, contracture of the soft tissues, shortened tendons, and obvious fixed deformities. 10 Several surgical techniques have been described for old midfoot injuries such as open reduction and internal fixation, arthrodesis, and staged management using external fixators as distractor followed by open reduction and internal fixation. 10,11 While the presented case had been admitted in an ICU for about 2 months, the surgeon and nurses had not been aware of possible foot injuries, although ankle foot orthosis had been applied during his admission in the ICU. As it was an old complex injury with involvement of different parts of the foot and cartilage loss in the joints, it was decided to do reconstructive arthrodesis instead of staged management to preserve the joints.
Missed first MTP joint fracture–dislocations are extremely rare injuries. There are only few reports of old dislocation of the first MTP joint. A 46-year-old man underwent surgical reduction of a dislocated first MTP joint after 6 months with an acceptable result and range of motion at 12 months postoperatively. 12 Another reported case is a 78-year-old man presented 4 months after trauma with inability to move his big toe. He suffered from dislocated first MTP joint with complete disruption of the plantar plate from the proximal phalanx. 13 Although there are several classifications for first MTP joint dislocation, 4 no one has described any cases of fracture–dislocation either acute or missed one. It may be suggested to classify fracture–dislocations as a new subtype. Our presented case is unique with old fracture–dislocation of first MTP joint with significant shortening. We had decided to do resection arthroplasty by shortening of base of proximal phalanx because simultaneous arthrodesis of naviculocuneiform, TMT, and MTP joints may result in a stiffed foot with disabilities; however, in the last follow-up visit, fusion of the first MTP joint was seen with acceptable outcome.
In conclusion, old complex fracture–dislocation of foot should be reconstructed and fused using bone grafts. Simultaneous arthrodesis of the first TMT and the first MTP joint could lead to acceptable outcome without incapacitating disability in the long term.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.